









Although the presence of three and four root canals are the most common anatomic configuration of the maxillary molar, other morphologies have also been reported. The purpose of this report is to show a series of clinical cases of maxillary first molars with five root canals. Improved understanding of these uncommon anatomic configurations should lead to better clinical outcomes. The use of the dental operating microscope and cone beam computer tomography was an important auxiliary when approaching the reported cases.
Apesar da presença de três e quatro canais radiculares ser a configuração anatómica mais comum no primeiro molar superior, é possível identificar outras morfologias. O objectivo deste trabalho é apresentar uma série de casos clínicos de primeiros molares superiores com cinco canais radiculares. O conhecimento de anatomias menos comuns pode levar a melhores resultados clínicos. A utilização do microscópio operatório e o recurso a imagens de cone beam podem ser meios auxiliares importantes na abordagem destes casos.
Most studies on maxillary first molar anatomy report it to be a three rooted tooth with three or four root canals.1–4 However, not only the number of the roots and root canals are variable,5–10 but also the shape of the pulp cavity.11 The failure of identifying the presence of an anatomic variation may compromise the success of the treatment.12 A review study on the anatomy of the maxillary first molar from Cleghorn et al.1 reported an incidence of the mesiopalatal canal (MP) of 56.8% and a prevalence of the distopalatal canal (DP) of 1.7%.
The aim of this paper is to show unusual maxillary first molar anatomic configurations with a presence of both mesiopalatal and distopalatal root canals.
Case reportsThe presented cases had endodontic treatment performed in private clinics in the area of Lisbon. After diagnosis formulation and the treatment proposed and accepted, all the teeth were anaesthetized with a buccal infiltration using 1.8ml of 4% articaine with 1:200,000 epinephrine (Artinibsa, Inibsa, Spain), proper rubber dam isolation was obtained, the decay was excavated and the proper access cavity was achieved. The root canals were identified and then negotiated with a stainless steel ISO size .08 hand files to the working length as determined by radiograph and electronic apex locator (Root Zx II, Morita, USA). Apical enlargement with hand files was performed until a manual glide path was achieved with stainless steel ISO size .15 hand files. The mechanical instrumentation was performed with the Protaper NiTi rotary files (ProTaper Universal, Dentsply Maillefer, Switzerland) as instructed by the manufacturer. All the instrumentations were performed with a continuous irrigation with 5.25% sodium hypochlorite. Because of the time required to accomplish the therapy none of the teeth were finished in one appointment. After the bio-mechanical preparation the root canals were dried with paper points and a paste of calcium hydroxide (Ultracal, Ultradent, USA) was used as intracanal medication. Cavit (Cavit W, 3M ESPE, Germany) was used as a provisional restorative filling between visits. At the second appointment one last rinse with 5.25% sodium hypochlorite was performed and the canals dried. Gutta-percha master points were fit. AH plus (AH Plus, Dentsply, Germany) was used as sealer. The obturation technique chosen was the continuous wave of condensation technique, the downpack was accomplished with a System B unit (System B, Sybron Endo, USA) and the backfill with an Obtura II unit (Obtura II, Obtura Spartan, USA). The pulp chambers were cleaned with a cotton pellet of alcohol and restored provisionally with Cavit temporary filling. All the teeth were scheduled for a permanent restoration as soon as possible.
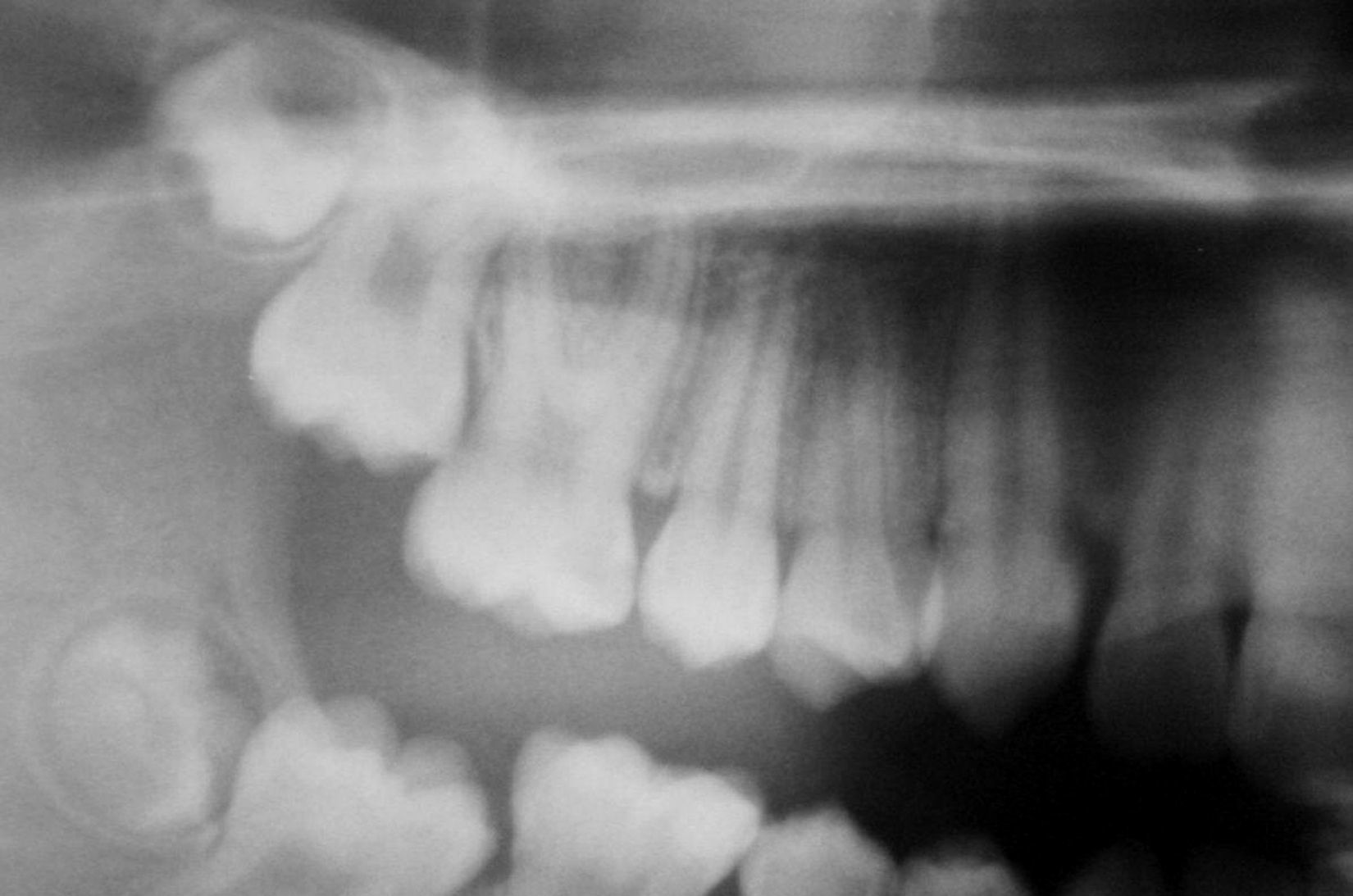
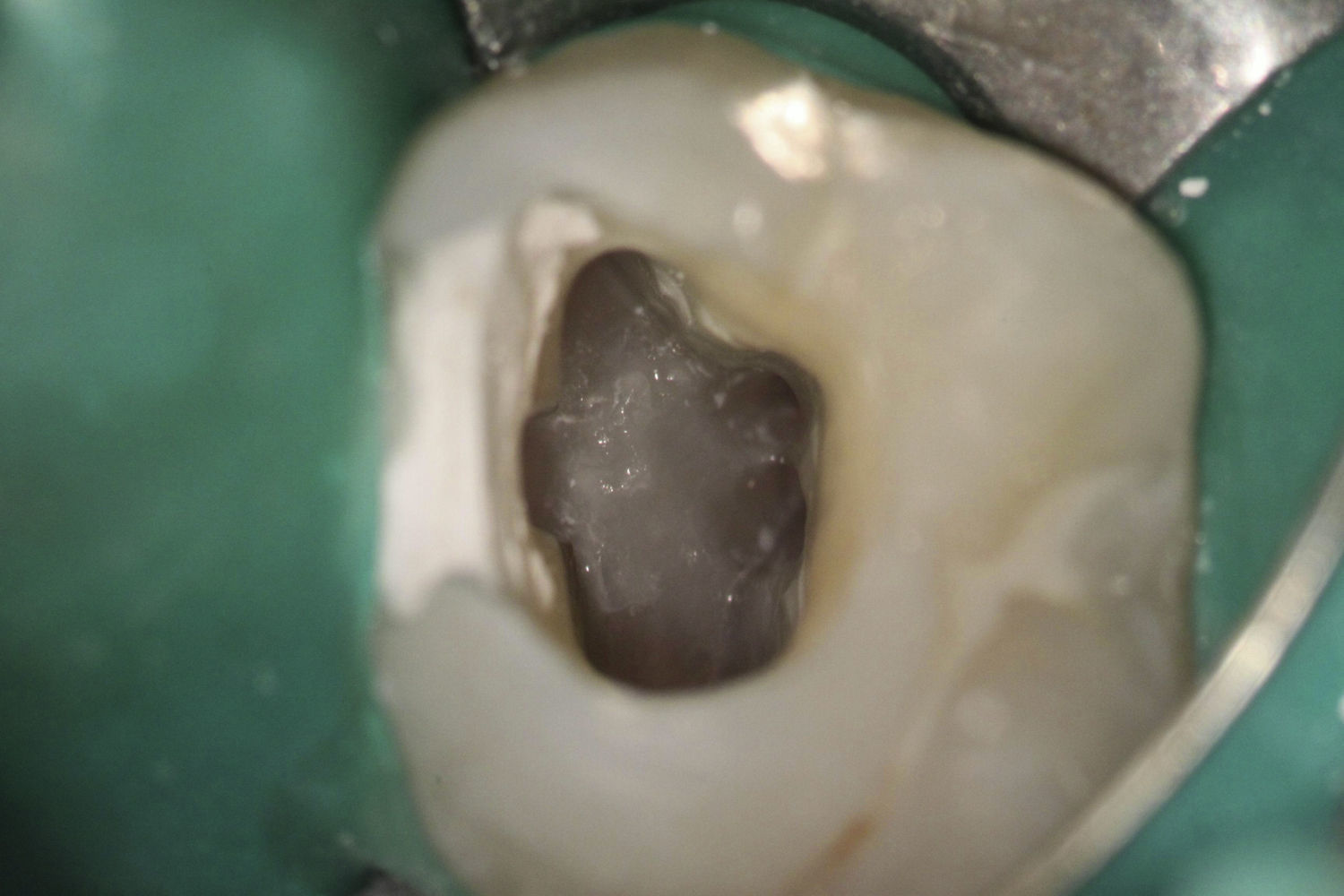
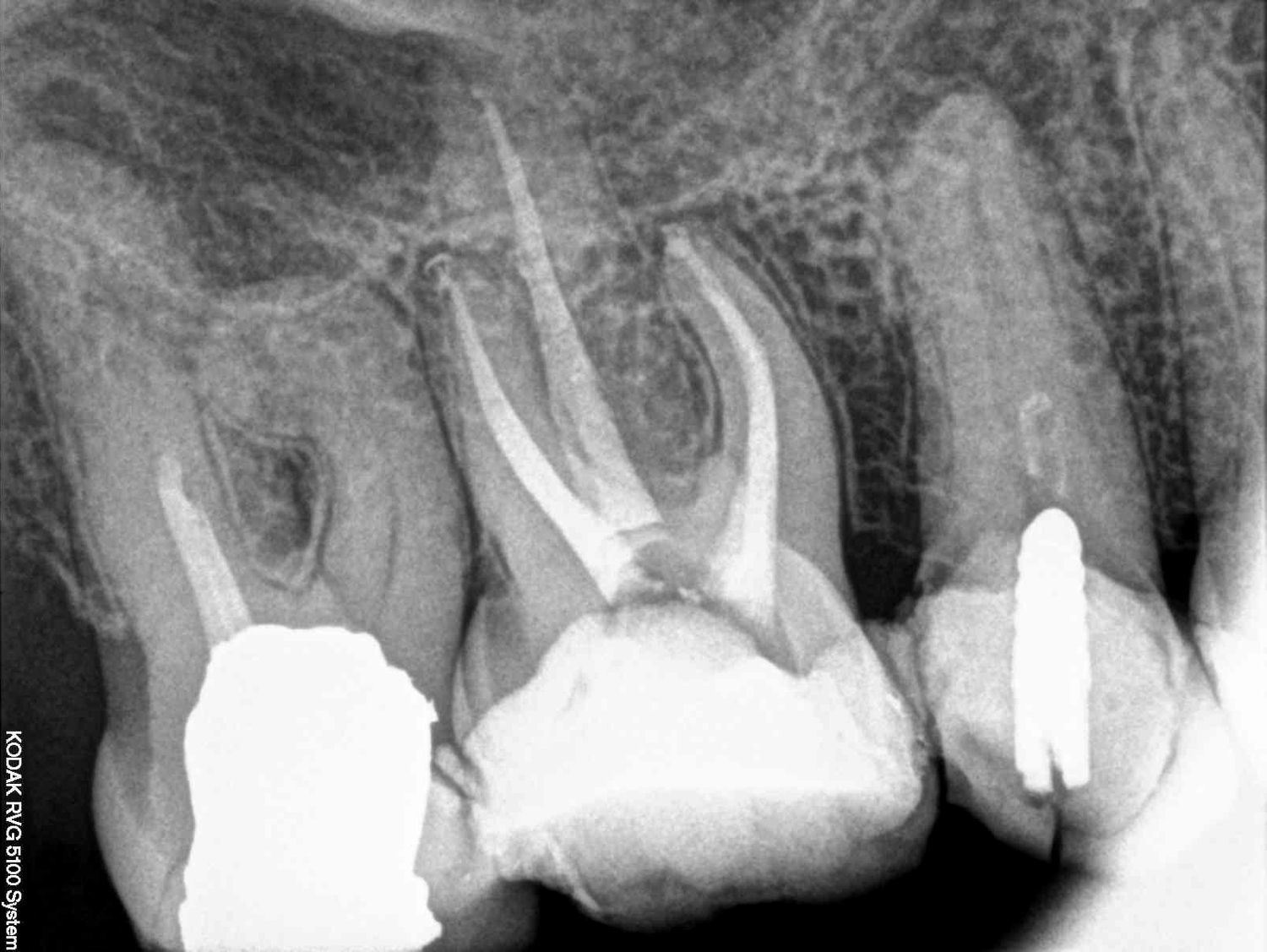
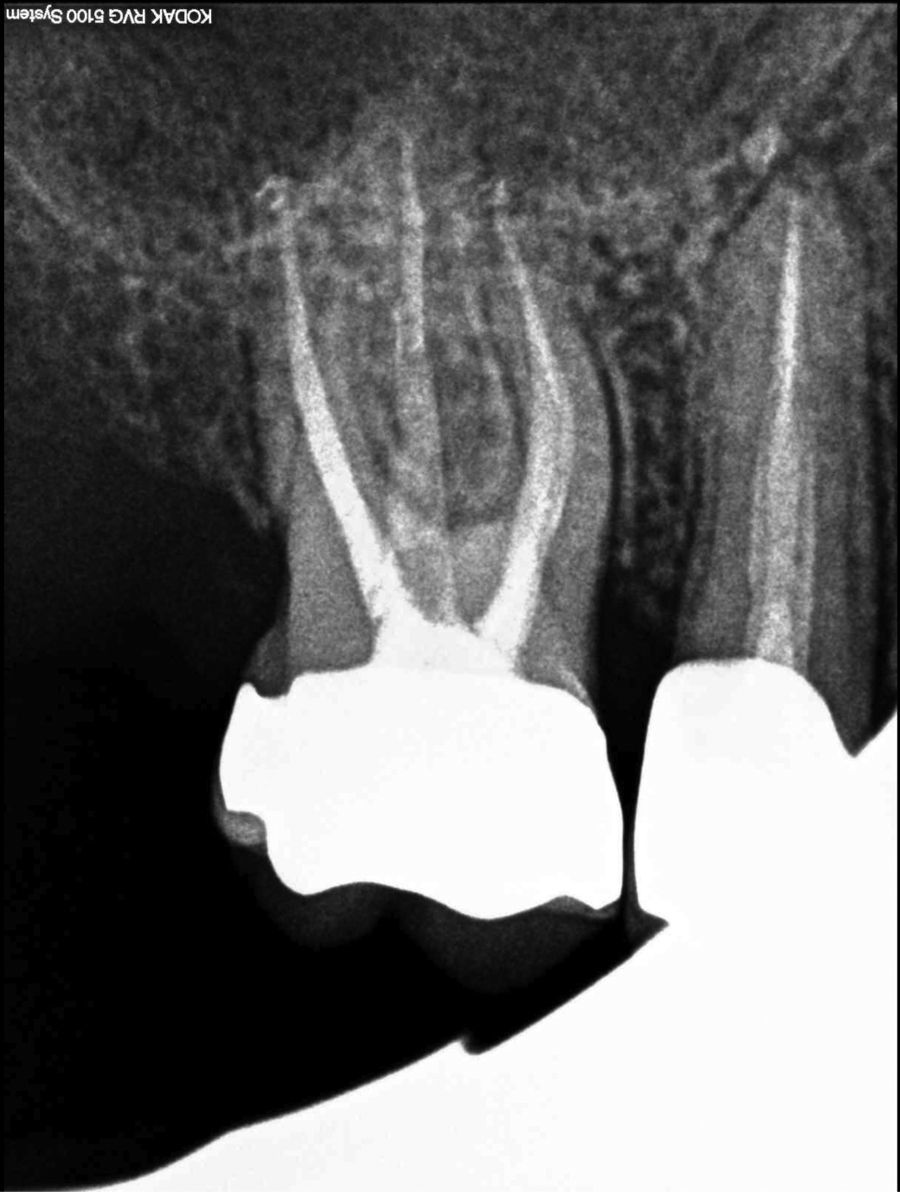
Case report 1A 16-year-old female presented to an emergency endodontic appointment with a chief complaint of spontaneous pain, and increasing pain to temperature variations in the maxillary right side. The medical history was non-contributory. A clinical and radiographic examination revealed a carious lesion on the mesial buccal side of the maxillary right first molar (tooth 16) (Figs. 1 and 2). The reaction to the ice sensibility test was an intense pain that remained present for more than one minute. The adjacent teeth had a normal response to this test. The diagnosis was an irreversible pulpitis on tooth 16. The endodontic therapy was proposed and accepted.


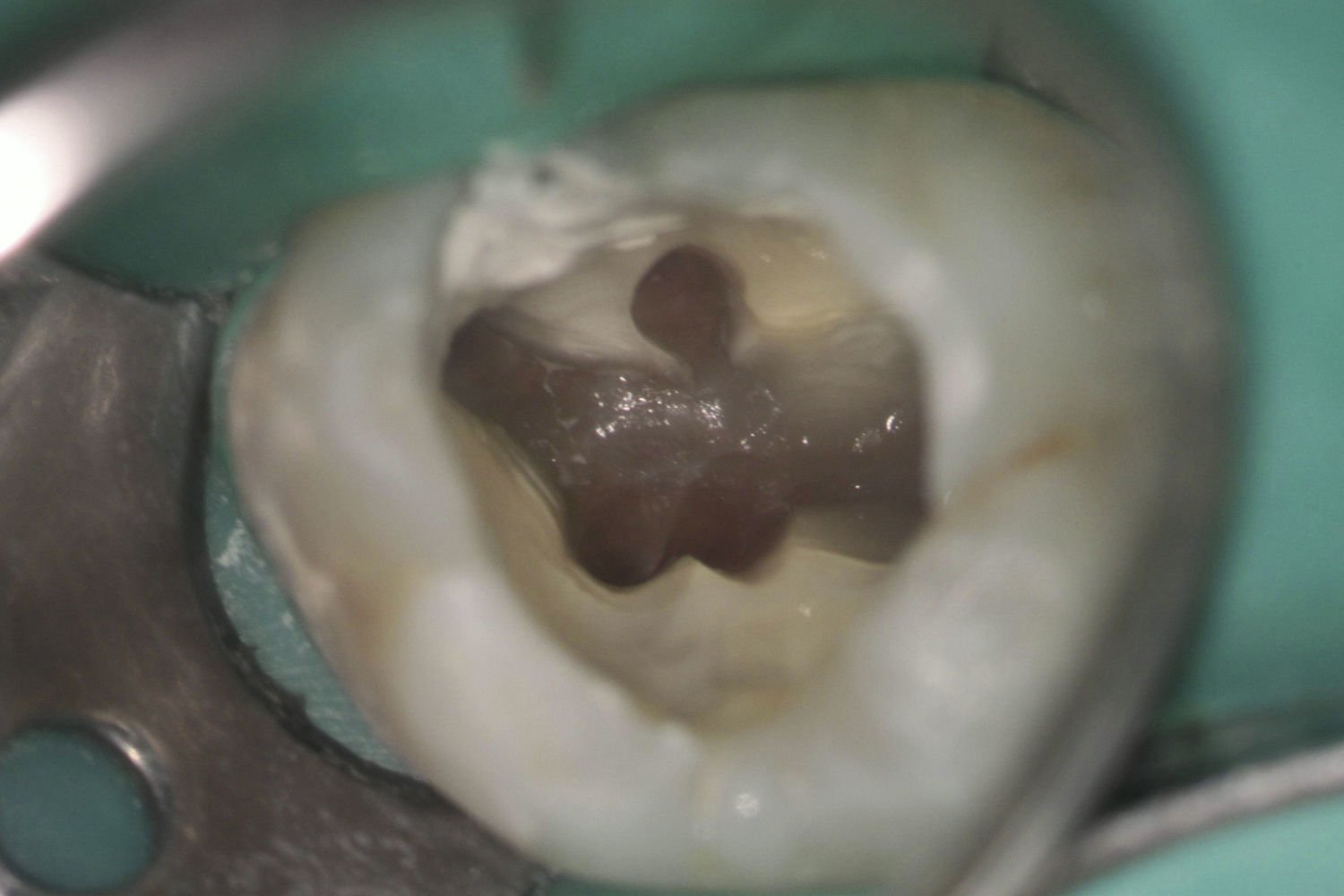
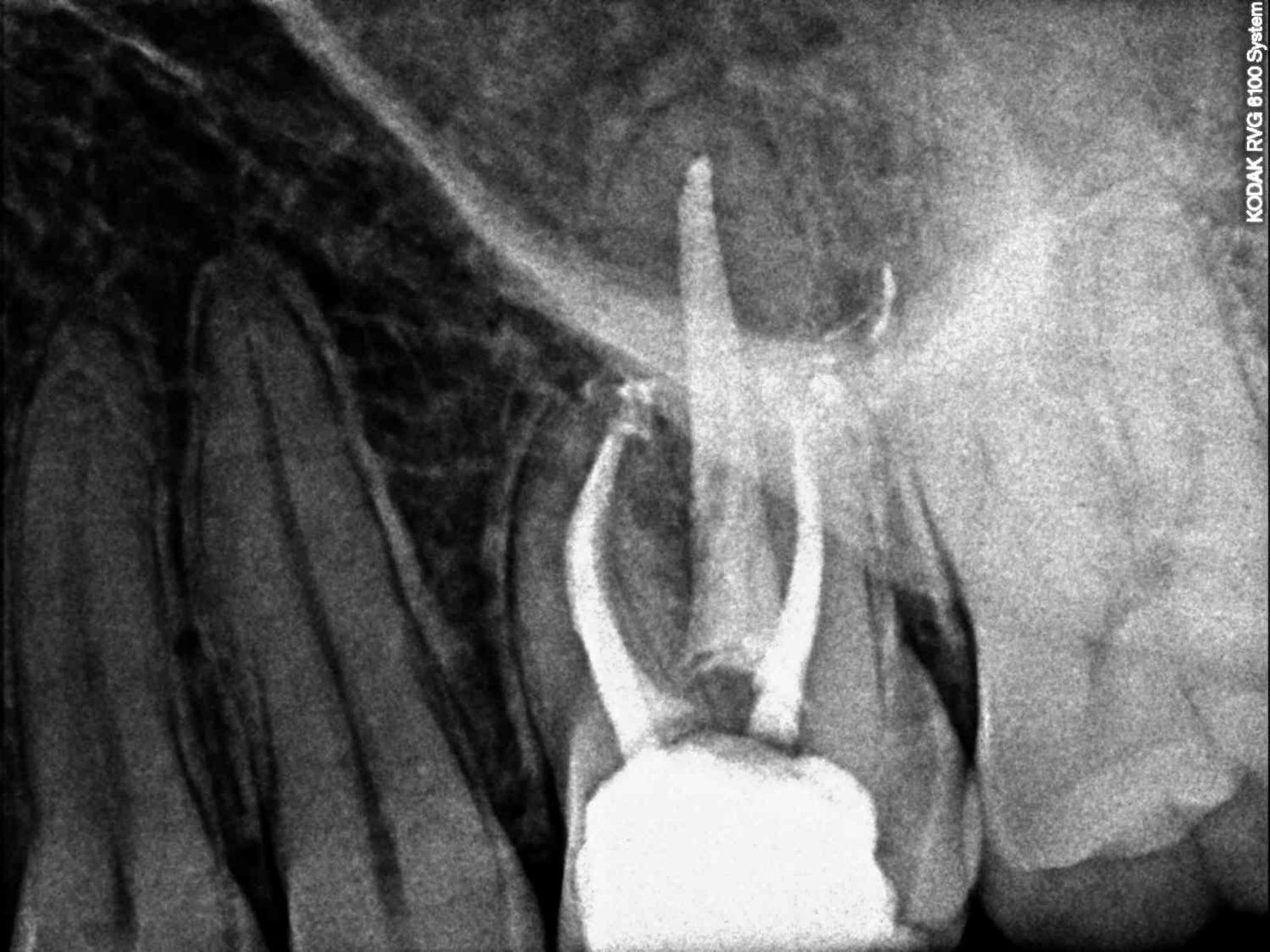
After proper anaesthesia and rubber dam isolation, the access cavity was prepared. During the exploration of the pulp chamber floor with a dental operating microscope (Opmi Pico, Carl Zeiss Surgical, Germany) it was possible to identify five canal orifices: two in the mesiobuccal root (MB and MP canals), two in the distobuccal root (DB and DP canals) and one in the palatal root (Fig. 3). During the root canal negotiation it became apparent that both canals in the mesiobuccal root were joining together in the apical third of the root. The same was happening in the distobuccal root. After measuring the working length, the rotary instrumentation was finished to an F2 Protaper in the buccal canals and with an F3 file in the palatal. After bio-mechanical preparation, the canals were dried and filled with a calcium hydroxide paste. The access cavity was provisionally restored. At the second visit, two weeks later, the root canal obturation was performed (Figs. 4 and 5).
Case report 2


A 28-year-old male was referred to endodontic treatment from a primary dentist. The patient did not have any complaint. The clinical and radiographic examination was able to detect a large carious lesion on the mesial surface of the maxillary first left molar (tooth 26) (Fig. 6). The response to the ice sensibility test was normal. The clinical diagnosis was a normal pulp on tooth 26, but because the extensive decay was impossible to excavate without pulp exposure the endodontic therapy was proposed and accepted by the patient.

After proper anaesthesia and rubber dam isolation, the decay was excavated and the access opening was prepared. With the help of a dental operating microscope the pulp chamber was examined. An anatomic configuration similar to the previous case report (Fig. 7) was noted. The endodontic treatment process was similar to previous case (Figs. 8 and 9).
Case report 3


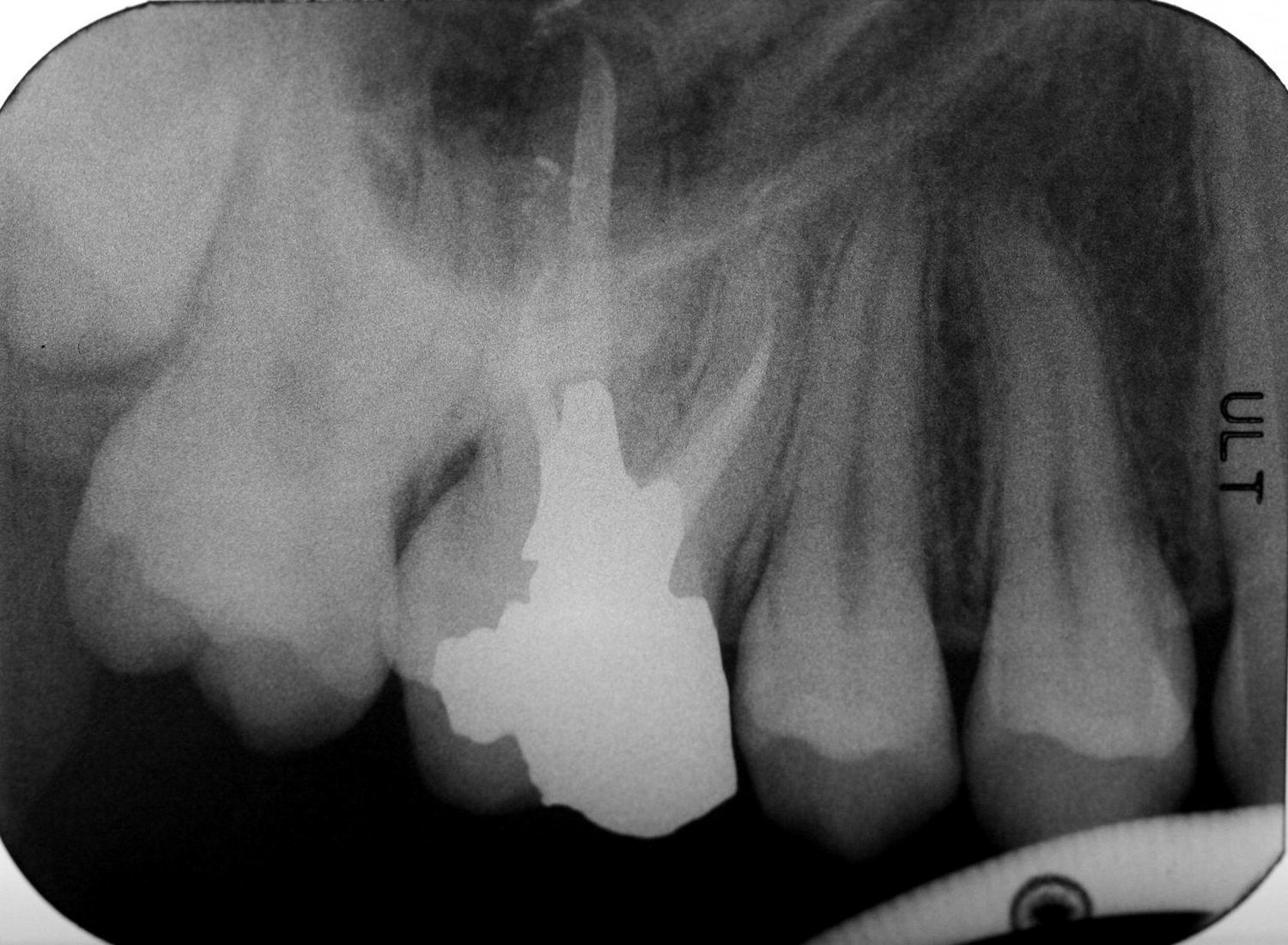
A 63-year-old female was presented for endodontic evaluation of the maxillary first right molar (tooth 16). The patient had no complaint on that specific tooth upon clinical examination and it was possible to detect a large amalgam filling without decay (Fig. 10). The diagnosis was a normal pulp on tooth 16. The primary doctor requested endodontic therapy on tooth 16 for oclusal correction as part of the overall treatment plan.

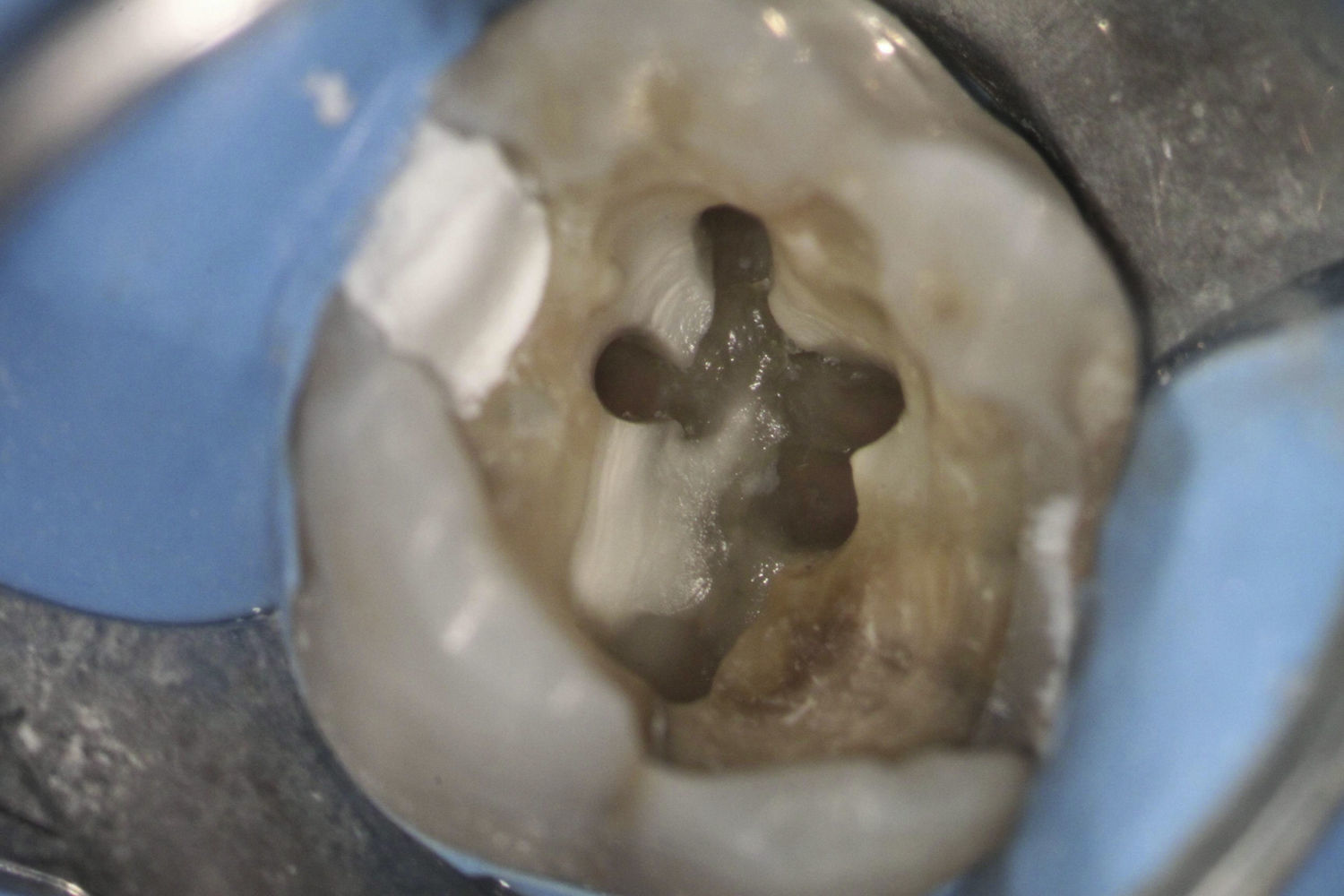
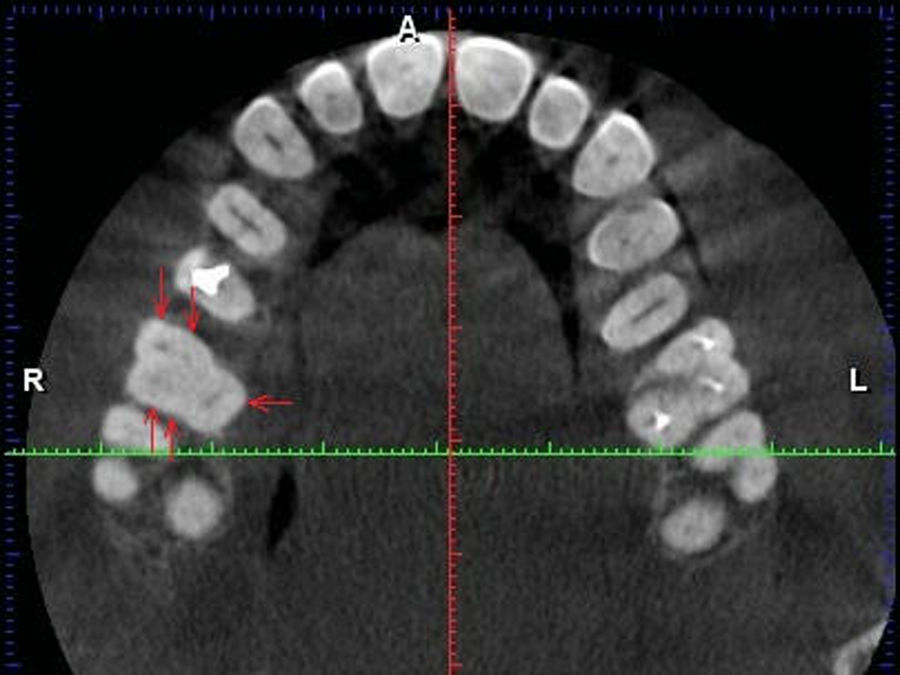
The tooth was anaesthetized and the rubber dam was placed. The amalgam filling was removed and the access preparation was performed. The examination of the pulp chamber floor utilizing a dental operating microscope was able to detect three orifice openings (MB, DB and PT canals) that were negotiated and bio-mechanical prepared to an F2 Protaper file. Two grooves were noted emerging from both buccal canals in the direction to palatal canal. Time limitation did not allow the exploration of the grooves at the first visit. The canals were dried and then dressed with a paste of calcium hydroxide. The access opening was provisionally closed with Cavit filling. At the second visit the two grooves were opened with #2 ProUltra ultrasonic tip (ProUltra, Dentspy Maillefer, USA) troughing and two extra canals were detected, one in each buccal root (MP and DP canals) (Fig. 11). The Cone Beam Computer Tomography (CBCT) scan obtained during the implant treatment planning was analysed to confirm the tooth anatomy (Fig. 12). Upon exploration of the two extra root canals, two independent root canals were noted on the mesiobuccal root and two merging canals were noted in the distobuccal root. The bio-mechanical preparation to an F2 Protaper rotary file was accomplished. The obturation procedures were accomplished at this appointment (Figs. 13 and 14).

.")


Several anatomic variations of the configuration of the maxillary first molar have been reported in the scientific literature. The work from Cleghorn et al.1 makes a review of the available literature. Regarding the mesiobuccal root, in a combined sample of 8399 roots from 34 laboratorial and clinical studies it was possible to identify one canal (MB) in 43.1% of the cases and two canals (MB and MP) in 56.8%. The incidence of one apical foramen in the mesiobuccal root was 61.6%. The distobuccal root review had a combined sample of 2576 roots from 14 laboratorial and clinical studies. The incidence of a single canal (DB) was 98.3% and the presence of two canals (DB and DP) was found in 1.7% of the cases. One apical foramen had a prevalence of 98%.
The present study presents three cases reporting a similar configuration on the pulp chamber floor with the presence of both a MP and DP canals. Two different root canal configurations were presented. The first and second case reports showed a Vertucci type II configuration on both mesiobuccal and distobuccal roots, while the third reported case presents a Vertucci type IV configuration on the mesiobuccal root and a Vertucci type II on the distobuccal root.
Because of the reported advantages,13,14 the examination of the pulp chamber floor was performed with a dental operating microscope. Several studies report a significant difference on the number of located canals when comparing examinations of the pulp chamber with or without magnification.15–17 The use of CBCT has also been described as useful when trying to understand the root canal anatomy.9,18–20 On the third reported case both MP and DP were only identified after exploring the anatomic grooves that were emerging from the MB and DB orifices and taking a palatal direction. Rectifying the access cavity and exploring this grooves and opening them using an ultrasonic troughing technique has been described as helpful on locating extra canals.21,22 Despite the attempts to schedule the recall appointment, it was not possible to bring back the second reported case, but the other two recalls show no clinical or radiographic findings (Figs. 15 and 16).


These cases confirm the necessity of a meticulous reading of the pulp chamber floor. Although the incidence is low, possible variations in the most common anatomic configurations may be present and should be explored. The use of the dental operating microscope may help detect these anatomies and, when present, the grooves surrounding the canal orifices should be explored.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data and that all the patients included in the study received sufficient information and gave their written informed consent to participate in the study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors have no conflict of interest to declare.