



The aims of this study are to: compare the condylar position in articular fossa after static and dynamic registration; analyze symmetry between right and left condyles and examine the relationship between articular eminence and condylar position.
MethodsTwenty completely edentulous patients were included in this study, after signing a written informed consent. Static registration was obtained by mandibular manipulation and dynamic registration was performed by Gothic Arch Tracing. Patients were submitted to one cone beam in static registration, followed by another with dynamic registration. Radiographic image measurements in lateral and frontal cuts were made.
ResultsNo statistically significant differences between the two methods were found. In dynamic registration all the distances were smaller, more consistent and equidistant. Condyles stayed in a closer position to the articular fossa and in a centred position. For this registration a higher symmetry between left and right condyle exists, revealed by homogeneous results. Static registration had a higher heterogeneity of results, due to the fact that it is dependent upon a number of factors.
ConclusionsDynamic registration seems a reliable and an accurate method to use. With the higher condylar symmetry and the centred position in articular fossa, it seems that this registration reproduces a physiologic condylar position.
Os objetivos deste estudo são a comparação da posição condilar, após registo estático e dinâmico; análise da simetria entre o côndilo direito e o côndilo esquerdo e a análise da relação entre a eminência articular e a posição condilar.
MétodosVinte desdentados totais participaram neste estudo, após assinarem um consentimento informado. O registo estático foi realizado através da manipulação mandibular e o dinâmico através do registo do traçado do Arco Gótico. Os doentes foram submetidos à primeira tomografia com o registo estático, tendo sido realizado a segunda com o registo dinâmico. Foram realizadas medições nos cortes tomográficos laterais e frontais.
ResultadosNão foram encontradas diferenças estatisticamente significativas entre os dois registos. No registo dinâmico todas as distâncias foram menores, mais consistentes e equidistantes. Os côndilos estavam numa posição mais centrada e próxima da fossa articular. Com este registo verificou-se uma maior simetria entre côndilos, através de resultados mais homogéneos. O registo estático teve maior heterogeneidade de resultados.
ConclusõesO registo dinâmico parece ser o método mais fidedigno e preciso. A maior simetria condilar e a posição mais centrada dos côndilos na fossa articular, parece que com que este registo se produz uma posição condilar fisiológica.
For an appropriate oral rehabilitation it is fundamental to take into account the functional and orthopaedic condylar position.1 In cases of bimaxillary edentulous patients, incorrect planning and execution of the rehabilitation procedures may result in unsuitable prosthesis and risk of temporomandibular disorders.2–5
The determination of the correct intermaxillary relation and condilar position is one of the most sensitive and rigorous procedures in the rehabilitation. Several authors1,5–7 referred the centric relation (CR) as the appropriate position for extended rehabilitation.
Various methods for determining the CR have been suggested in the literature.8–13 Static (mandibular manipulation) and graphical methods (Gothic Arch Tracing) are the most often used.4,14
The use of conventional radiographic techniques, such as orthopantomography (OPG) and computerized tomography (CT), may indicate whether the condyle is in the CR position. CT provides three-dimensional images but with high radiation, whereas OPG overcomes the radiation exposure, but limited to bidimensional images.5,15–18
Evaluating the condylar position by cone beam computed tomography (CBCT) has become an essential tool to obtain three-dimensional images. The capture of the area of interest with rapid scan time (10–70s) minimizes the exposure of adjacent structures, while exposing the patient to low radiation doses.19–23
The aim of this study was to compare the condylar position, using frontal and lateral CBCT images, after static and dynamic registration, to understand which of the two methods contributes to the best radiographic CR position. The secondary objectives were to: analyze symmetry between right and left condyles and examine the relationship between articular eminence and condylar position.
Following this the null hypothesis formulated were:
- (1)
There are no differences in condylar position determined by the measurements, obtained for the sagittal and frontal views, for static and dynamic registrations.
- (2)
There are no differences between right and left condilar position, for both methods of registration.
The study was designed to include twenty adult edentulous patients, seeking for a conventional removable rehabilitation in the Dentistry Department, Faculty of Medicine, University of Coimbra (FMUC) that met the following inclusion criteria:
- •
Never submitted to radiotherapy;
- •
No history of symptoms of the temporomandibular joint;
- •
Classified as ASA 1 or 2 (normal healthy patient or with mild systemic disease, according to the American Society of Anaesthesiologists Physical Status Classification System);
- •
Willing to participate and to sign a written informed consent form.
This study was approved by the Ethic Committee of the Faculty of Medicine, University of Coimbra (FMUC), with reference n° 042-CE-2013.
For static registration, over the definitive maxilla and mandibular models, a stabilized base with light-curing resin plate (Elite® LC tray, Italy) was made and prepared to support a wax rim (Modelling Wax, Anutex, Kemdent®, England) necessary for obtaining static registration.
This registration was obtained by a pre-graduate student in his/her last year, supervised by a tutor (an experienced prosthodontist and clinical instructor). In this method the operator applied pressure against the chin area of the mandible, pressing downwards and slightly backwards with both thumbs, to position the condyle in the articular fossa. The wax rims were simultaneously closed in contact, maintaining the bases adapted to support tissues at the vertical dimension of occlusion (VDO) required and blocked in the intermaxillary position defined, with a rigid impression material (Temp Bond-NE™, Type I, Kerr®, Italy).
The static registration made in that consultation was repositioned in the mouth. Two facial landmarks on the tip of the nose and on the tip of the chin were drawn using a black permanent marker (Lumocolor®, medium – 1mm, Staedtler®, Germany). A Willis gauge was used to register the vertical dimension of occlusion established during the static registration, in order to assure that both dynamic and static registrations were done at the same VDO.
The radiographic examination was then made with CBCT IS i-CAT® CBCT unit (Imaging Sciences International, Hatfield, PA, USA). The device was operated at 5mA and 120kVcP.
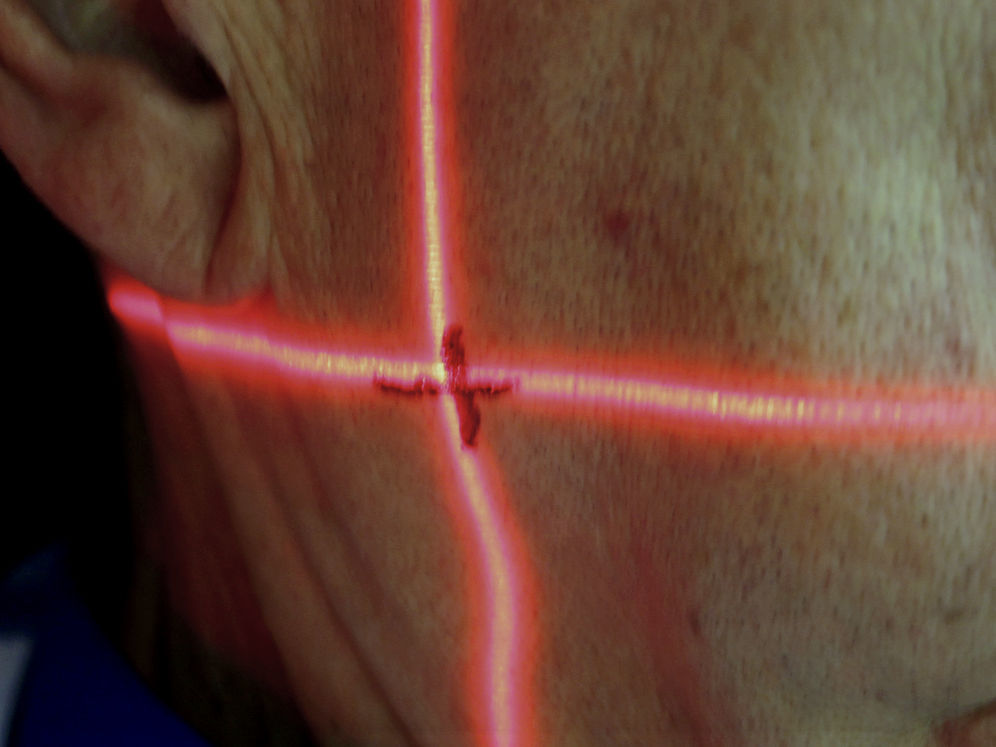
A preview image was made before the final acquisition to evaluate sagittal orientation. Then, marks were made with a black permanent marker on the patient's face, coinciding with laser marks (Fig. 1). These marks had the objective of allowing the reposition of the patient's head, in the same position, in the next CBCT after dynamic registration. Then, a single 360° rotation, 8.9s scan was done for each patient, with a 16cm×10cm field of view, 0.3voxel. All images were acquired using IS i-CAT Vision™, Imaging Sciences International.

For Dynamic Registration, over the mandibular model a new stabilized base (light-curing resin plate: Elite® LC Tray) was prepared with an intraoral Gothic Arch tracer (Massad intra-oral Establisher®, Tulsa, USA), supporting the central pin. In the upper base a sliding platform of the same device was placed and stabilized with impression compound (type I, Kerr™, Czech Republic).
The platform was painted with a blue permanent marker (Lumocolor®, medium – 1mm, Staedtler®, Germany) and the two plates of intermaxillary registration were placed in the mouth. The pin was placed at the height corresponding to the established VDO.
The patient was instructed to carry out extreme lateral and protrusive mandibular movements and a Gothic Arch Tracing was made, corresponding to the stability of CR position (Fig. 2). A transparent plastic disc with a small opening in the middle was secured with sticky wax on the mandibular plate, so that the centre of the opening was superimposed on the apex of the Gothic Arch Tracing.
. This apex corresponds to the position of the mandible in centric relation.")
The patient's mandible was then directed so that on closing, the pin entered the plastic disc hole. Then, silicone bite registration material (Jet Bite®, type 1, Coltène/Whaledent AG©, Switzerland) was injected into the interarch space. For the second scan, the patient's head was placed in the same position as previously explained using the laser marked lines.
After registrations and cone beam tomographies, the images were analyzed and selected in InVivo Dental Application, version 5.0 (Anatomage, USA).
To confirm that the images analyzed coincided, an overlapping procedure was followed.
In this sense, all the images and cuts selected previously were identified and converted to an image negative using Adobe® Photoshop® CS6, version 13.0×64 and an impression in acetate sheet was performed.
Then a manual overlapping was done to confirm and validate that the image cuts selected were the same.
An expert, blinded to the study, did a direct observation of the acetate sheets images and analyzed the condylar position. After which, the expert indicated the image (corresponding to one of the methods), that would be the registration of choice to rehabilitate each patient. The results were registered on a digital table.
The measurements of distances were made using ImageJ Software, 1.48v (Wayne Rasband, National Institutes of Health, USA) with the original selected images.
The measurements for sagittal and frontal cuts were performed based on the methodology followed by previous authors.5 The same operator performed all the measurements. The entire measuring process was conducted identically on the lateral cuts of the left side and the operator recorded three measurements in three sagittal cuts (Figs. 3 and 4). Measuring of the frontal cuts started with the Right Frontal cut (Figs. 5 and 6).

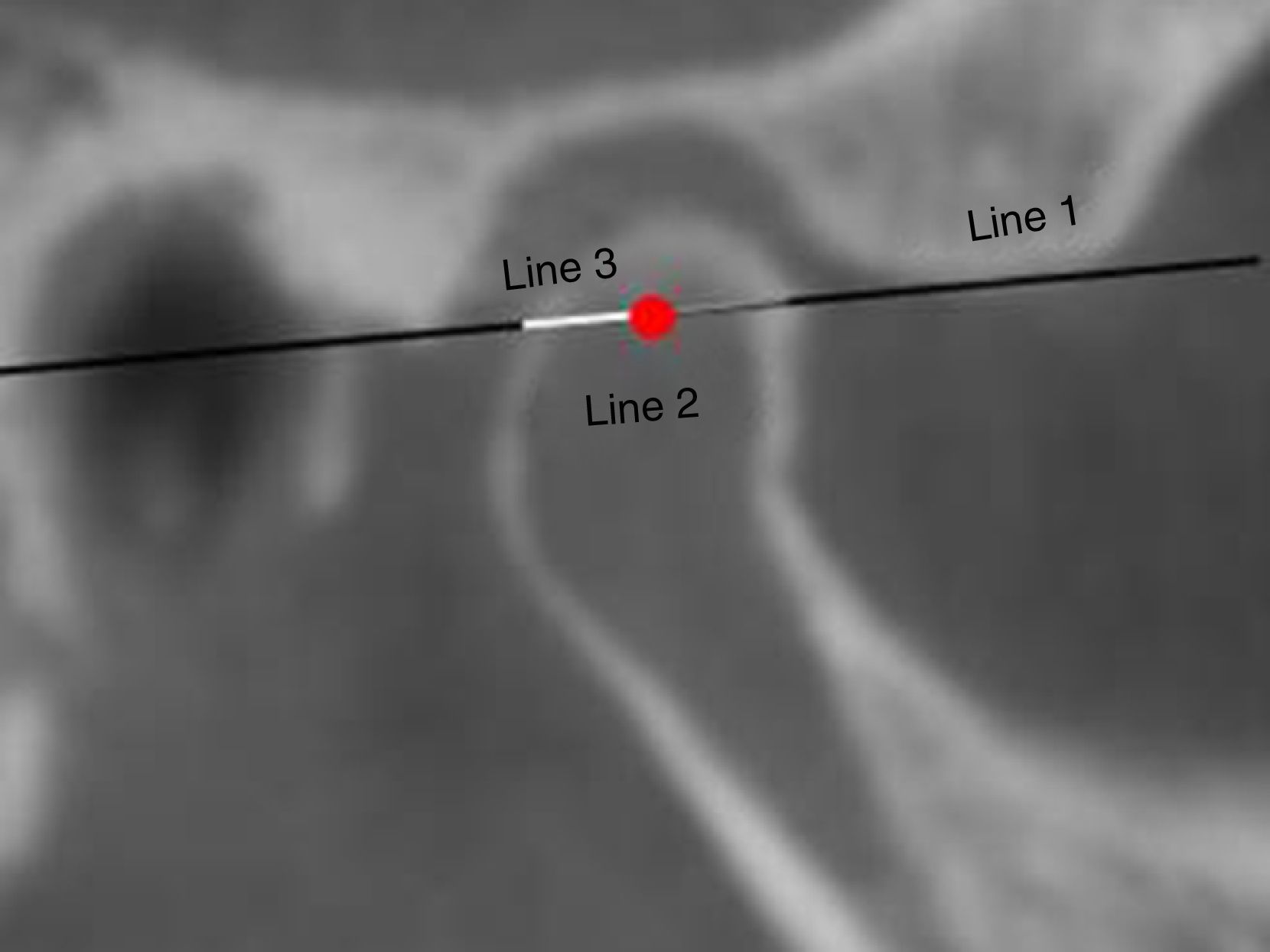
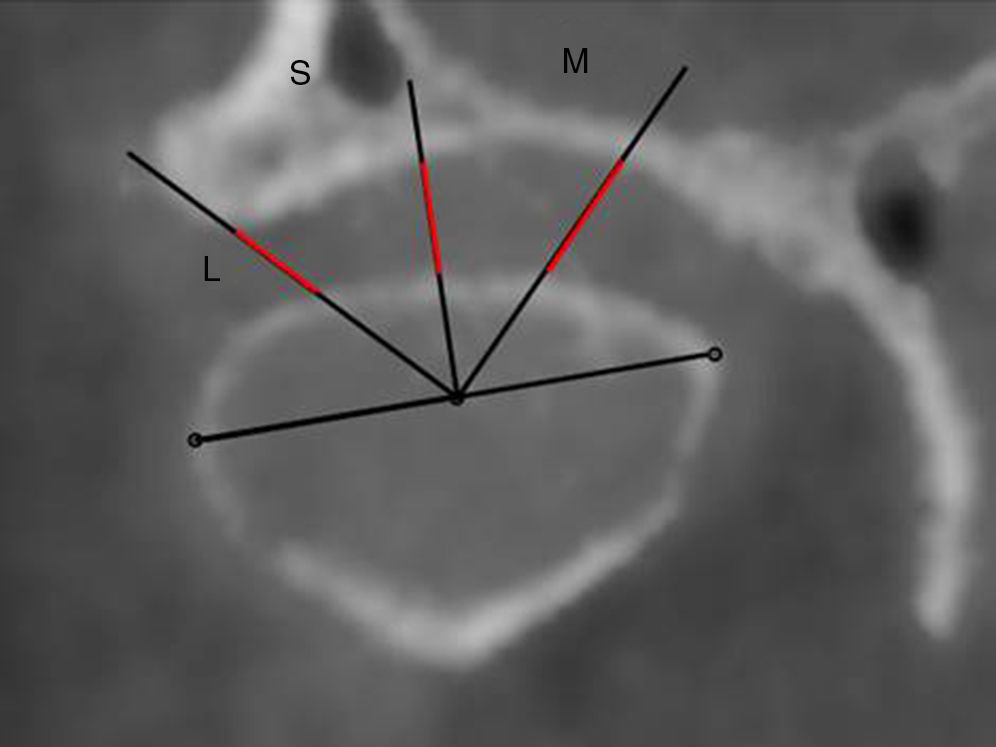
Sagittal view of the right condyle. A reference line 1 was traced tangentially to the lowest posterior and anterior extremities of the articular fossa. Reference line segment 2 was then traced on a segment of line 1 overlapping the condylar process and the middle point was recorded, based on a reference line segment 3 over half of line 2.
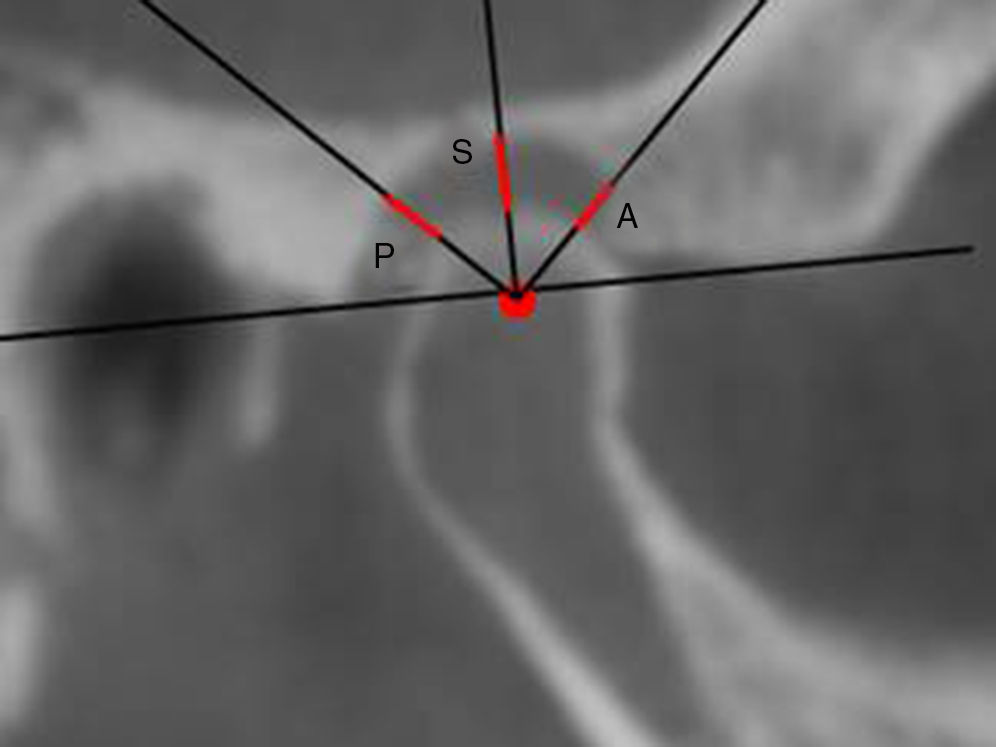
. Another measurement, named “anterior” (A) was obtained in a similar fashion, except for an anterior variation of 45° and a final measurement, named “posterior” (P) was obtained in the same way, except for a posterior variation of 45° with line 1.")
Sagittal view of the right condyle. An angle tool was then used to form a 90° angle with reference line 1. Then, the distance was measured between the uppermost point of the condyle and the closest internal point of the articular fossa overlapping the vertical line of the angle tool and this measurement was named “superior” (S). Another measurement, named “anterior” (A) was obtained in a similar fashion, except for an anterior variation of 45° and a final measurement, named “posterior” (P) was obtained in the same way, except for a posterior variation of 45° with line 1.

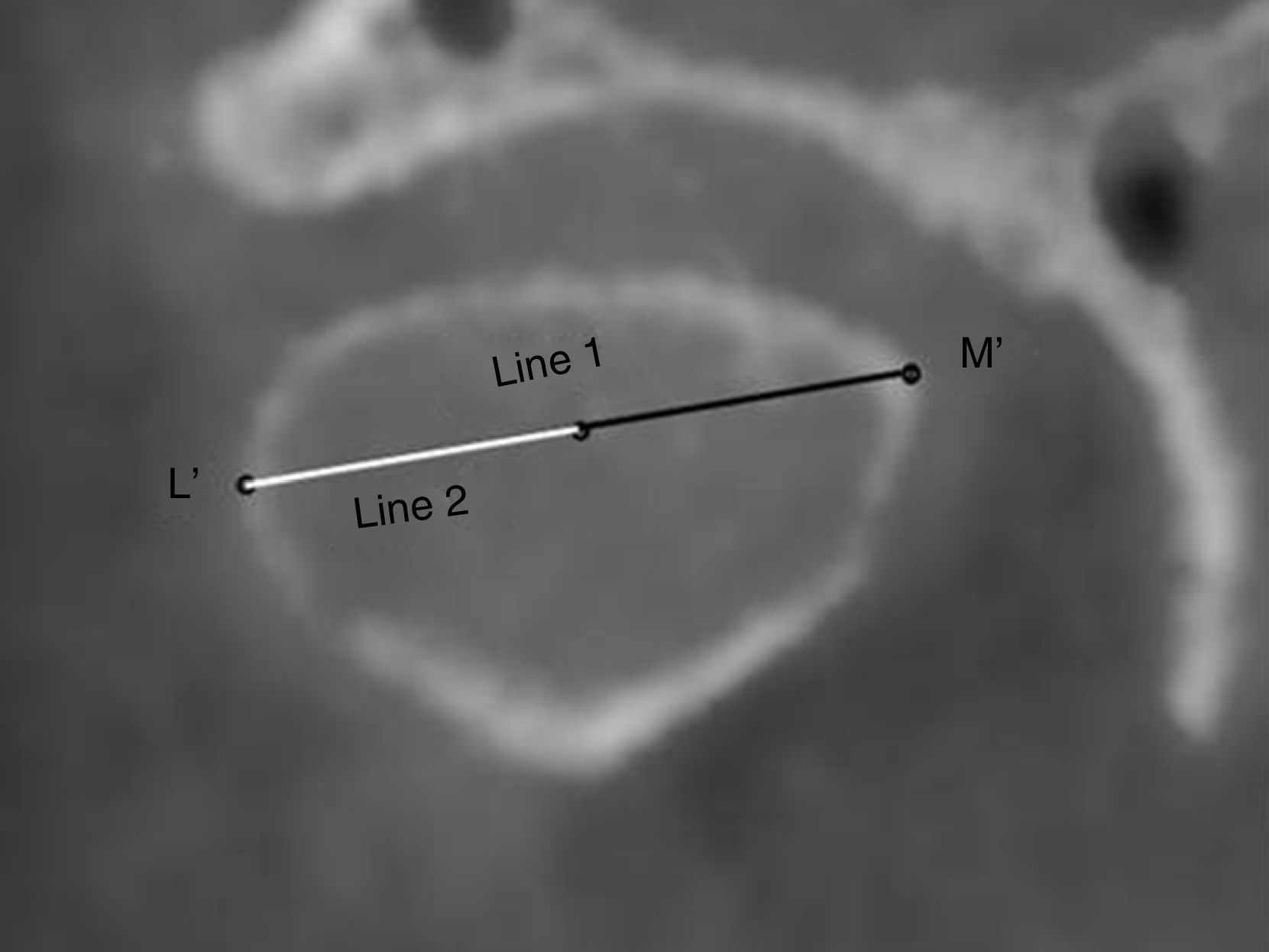
Frontal view of the right condyle. The most medial and lateral points of the condylar head were identified. The line measuring tool was used to connect these points to produce line 1. A segment line was then traced overlapping the line 1 up to exactly half of its length and this line was termed the line 2. A point at the end of the line 2 was named the middle point of reference for the frontal cut.

Frontal view of the right condyle. The angle tool was used to form a 90° angle, which was then placed at a 45° angle placed to line 1 and the angle's vertex was adjusted to meet the middle point of reference, and then the “superior”, “medial” and “lateral” measurements were obtained.
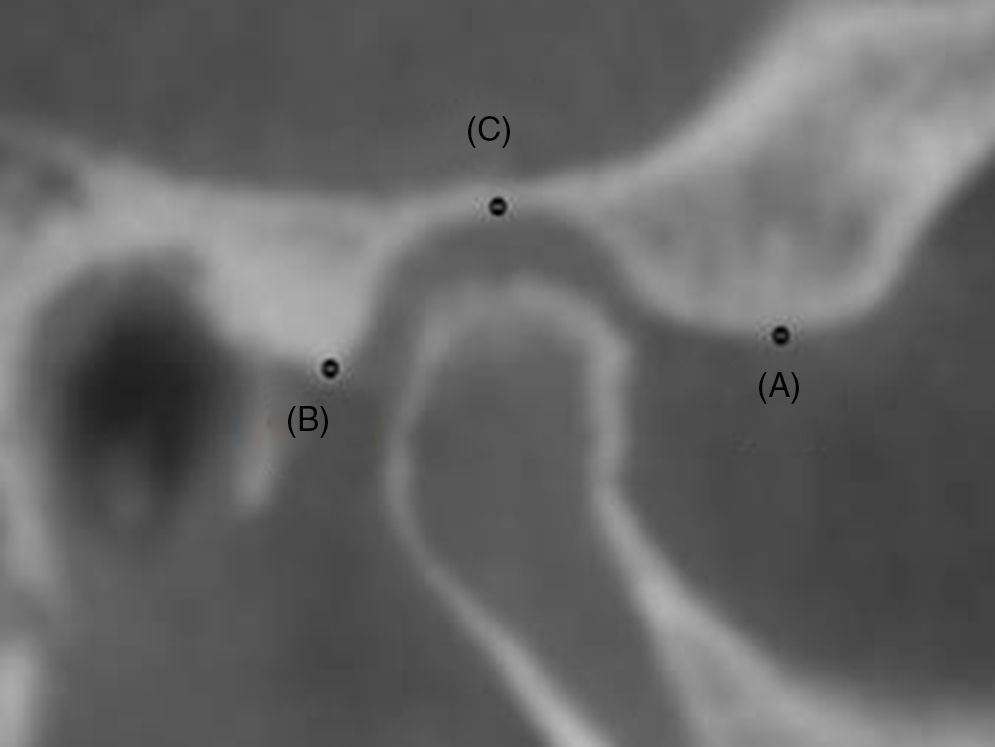
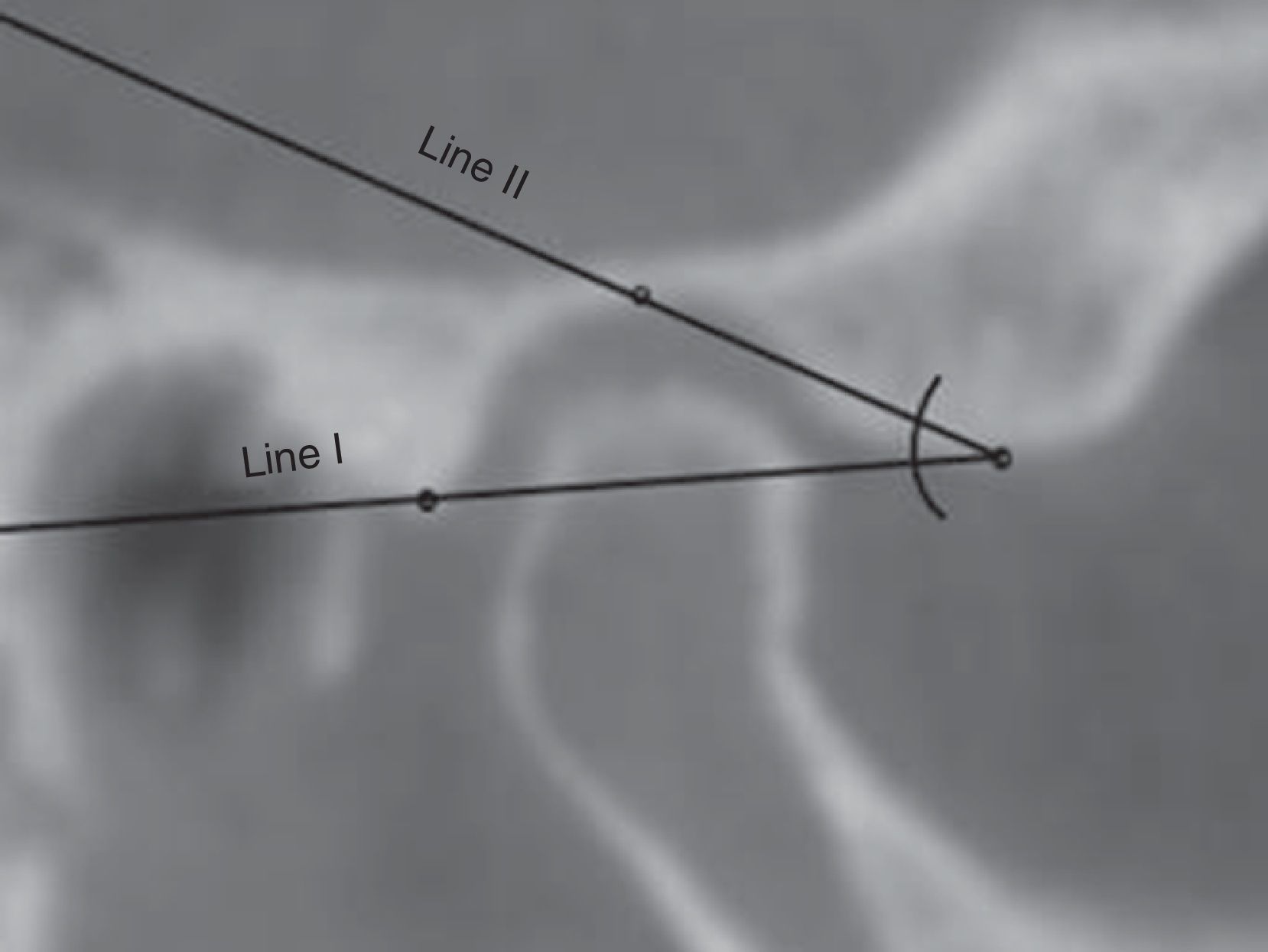
Authors did an adaptation based on previous studies.24 for articular eminence inclination, axial views of the condylar processes were seen and measurements were made (Figs. 7 and 8).
; lowest point of the posterior wall of the articular fossa (B); highest point of the fossa (C).")
; a straight line passing through C and A (line II).")
The values were then introduced on a digital table for subsequent statistical analysis.
Statistical analysis was carried out using IBM® SPSS® Statistics version 20 for Windows.
The comparison of sagittal and frontal measurements, for static and dynamic registration was carried out using a t-test for paired samples.
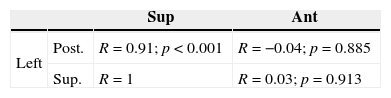
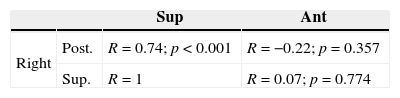
The mean differences between right and left measurements in the sagittal plane, were determined to analyze the symmetry of the two condyles within the joint. Also, for each registration method, a Pearson correlation was established between the posterior, anterior and superior measurements of the left and right sides.
To determine the influence of the angle of articular eminence on the measurement obtained for superior space, a Pearson correlation was executed.
All analyses were performed at a significance level of α=0.05.
ResultsTwenty edentulous patients (9 males and 11 females) with a mean age of 63.3±9.0 years were enrolled in this clinical trial. The patient enquiry determined a mean maxillary edentulism of 13.3±11.16 years and mandibular edentulism of 7.35±10.50 years.
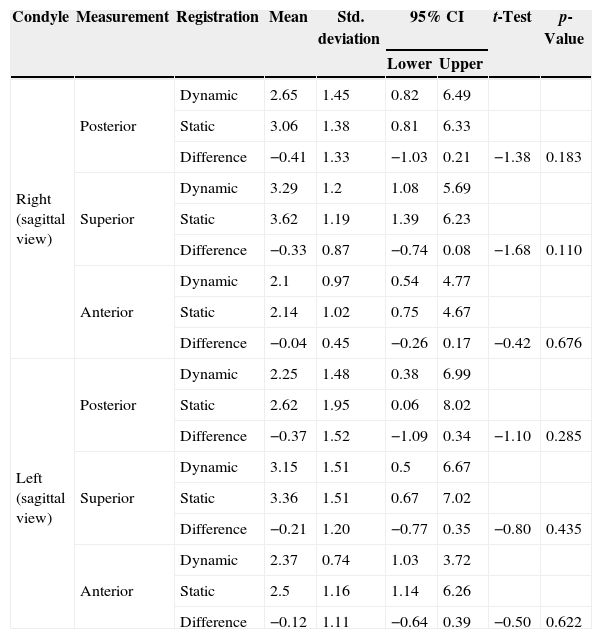
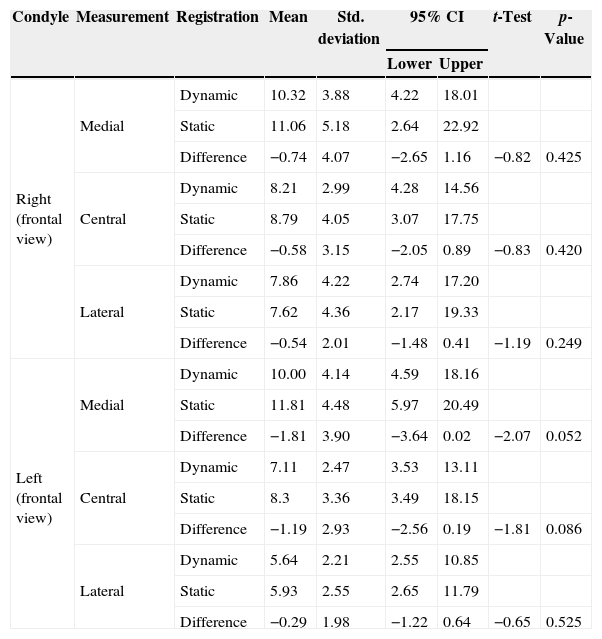
The descriptive statistics of the three measurements obtained for the sagittal and frontal planes for the right and left condyles, as well as the difference between static and dynamic registration are summarized in Tables 1 and 2. For the right and left condyles, in both sagittal and frontal views, no statistically significant differences were determined between the two methods of intermaxillary registration (p>0.05).
Comparison of sagittal measurements (mm), for static and dynamic registration. Paired-samples t-test for a significance level of α=0.05. 95% CI – 95% confidence interval for the difference.
| Condyle | Measurement | Registration | Mean | Std. deviation | 95% CI | t-Test | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Right (sagittal view) | Posterior | Dynamic | 2.65 | 1.45 | 0.82 | 6.49 | ||
| Static | 3.06 | 1.38 | 0.81 | 6.33 | ||||
| Difference | −0.41 | 1.33 | −1.03 | 0.21 | −1.38 | 0.183 | ||
| Superior | Dynamic | 3.29 | 1.2 | 1.08 | 5.69 | |||
| Static | 3.62 | 1.19 | 1.39 | 6.23 | ||||
| Difference | −0.33 | 0.87 | −0.74 | 0.08 | −1.68 | 0.110 | ||
| Anterior | Dynamic | 2.1 | 0.97 | 0.54 | 4.77 | |||
| Static | 2.14 | 1.02 | 0.75 | 4.67 | ||||
| Difference | −0.04 | 0.45 | −0.26 | 0.17 | −0.42 | 0.676 | ||
| Left (sagittal view) | Posterior | Dynamic | 2.25 | 1.48 | 0.38 | 6.99 | ||
| Static | 2.62 | 1.95 | 0.06 | 8.02 | ||||
| Difference | −0.37 | 1.52 | −1.09 | 0.34 | −1.10 | 0.285 | ||
| Superior | Dynamic | 3.15 | 1.51 | 0.5 | 6.67 | |||
| Static | 3.36 | 1.51 | 0.67 | 7.02 | ||||
| Difference | −0.21 | 1.20 | −0.77 | 0.35 | −0.80 | 0.435 | ||
| Anterior | Dynamic | 2.37 | 0.74 | 1.03 | 3.72 | |||
| Static | 2.5 | 1.16 | 1.14 | 6.26 | ||||
| Difference | −0.12 | 1.11 | −0.64 | 0.39 | −0.50 | 0.622 | ||
Comparison of frontal measurements (mm), for static and dynamic registration. Paired-samples t-test for a significance level of α=0.05. 95% CI – 95% confidence interval for the difference.
| Condyle | Measurement | Registration | Mean | Std. deviation | 95% CI | t-Test | p-Value | |
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| Right (frontal view) | Medial | Dynamic | 10.32 | 3.88 | 4.22 | 18.01 | ||
| Static | 11.06 | 5.18 | 2.64 | 22.92 | ||||
| Difference | −0.74 | 4.07 | −2.65 | 1.16 | −0.82 | 0.425 | ||
| Central | Dynamic | 8.21 | 2.99 | 4.28 | 14.56 | |||
| Static | 8.79 | 4.05 | 3.07 | 17.75 | ||||
| Difference | −0.58 | 3.15 | −2.05 | 0.89 | −0.83 | 0.420 | ||
| Lateral | Dynamic | 7.86 | 4.22 | 2.74 | 17.20 | |||
| Static | 7.62 | 4.36 | 2.17 | 19.33 | ||||
| Difference | −0.54 | 2.01 | −1.48 | 0.41 | −1.19 | 0.249 | ||
| Left (frontal view) | Medial | Dynamic | 10.00 | 4.14 | 4.59 | 18.16 | ||
| Static | 11.81 | 4.48 | 5.97 | 20.49 | ||||
| Difference | −1.81 | 3.90 | −3.64 | 0.02 | −2.07 | 0.052 | ||
| Central | Dynamic | 7.11 | 2.47 | 3.53 | 13.11 | |||
| Static | 8.3 | 3.36 | 3.49 | 18.15 | ||||
| Difference | −1.19 | 2.93 | −2.56 | 0.19 | −1.81 | 0.086 | ||
| Lateral | Dynamic | 5.64 | 2.21 | 2.55 | 10.85 | |||
| Static | 5.93 | 2.55 | 2.65 | 11.79 | ||||
| Difference | −0.29 | 1.98 | −1.22 | 0.64 | −0.65 | 0.525 | ||
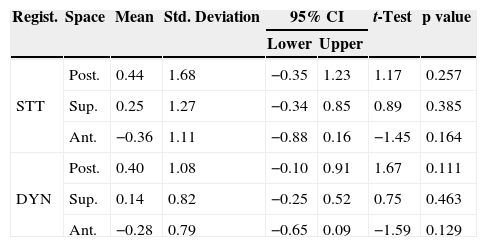
No statistically significant differences between the position of the right and left condyles, for either form of registration, were found (Table 3).
Differences between right and left side of the condyles, for static and dynamic registration. 95% CI – 95% confidence interval for the difference (Difference=right−left). STT – static; DYN – dynamic; Regist. – registration; post. – posterior; ant. – anterior; sup. – superior.
| Regist. | Space | Mean | Std. Deviation | 95% CI | t-Test | p value | |
|---|---|---|---|---|---|---|---|
| Lower | Upper | ||||||
| STT | Post. | 0.44 | 1.68 | −0.35 | 1.23 | 1.17 | 0.257 |
| Sup. | 0.25 | 1.27 | −0.34 | 0.85 | 0.89 | 0.385 | |
| Ant. | −0.36 | 1.11 | −0.88 | 0.16 | −1.45 | 0.164 | |
| DYN | Post. | 0.40 | 1.08 | −0.10 | 0.91 | 1.67 | 0.111 |
| Sup. | 0.14 | 0.82 | −0.25 | 0.52 | 0.75 | 0.463 | |
| Ant. | −0.28 | 0.79 | −0.65 | 0.09 | −1.59 | 0.129 | |
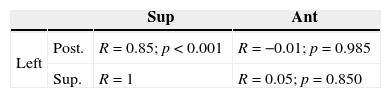
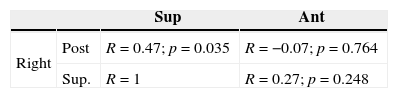
In both condyles and for the two methods of determining the intermaxillary relationship, a strong positive correlation was obtained between the posterior and superior measurements, meaning that larger posterior spaces correspond to larger superior spaces. No statistically significant correlations were established, with the anterior measurement (Tables 4–7).
There was a tendency to a moderate positive correlation between the angle of the articular eminence and its superior space, with statistical significance limited to the static registration on the right side (r=0.52, p=0.019).
DiscussionAccording to several authors,25,26 when joint structures are anatomically correctly positioned, mandibular equilibrium is met. CR seems to be a correct position that ensures space for the articular disc and avoids temporomandibular disorders.1,19,25,27
Comparing static with dynamic registration, the first one is dependent upon a number of factors, for example: muscle tone, tissue resiliency, guidance of the mandible and pressure applied.4,9,28 It requires stabilized bases and tissue resiliency or advanced alveolar ridge resorption could affect their stability. Wax on the stabilized bases can undergo dimensional instability, leading to greater inaccuracy in the intermaxillary registration.13
In the dynamic method, to guarantee a correct registration, all procedures for the correct execution were followed with demanding criteria. Stabilized bases, correct VDO and correct Gothic Arch Tracing were considered fundamental for their acceptance and validation. Patients with advanced alveolar ridge resorption or with a macroglossia had more problems doing this registration.13,29 However, as seen in this study, this method seems more accurate and easier and all the patients included were capable of doing it.
An expert, blinded to the study, observed the cone beam images of the two registrations and evaluated, at two separate times, which image corresponded to a theoretically better condylar position.
According to Cohen's Kappa, a statistical measurement of agreement, there was a high variance in the selected images from the first to the second observation (measurement of agreement: 0.286, p=0.199. Values of Cohen's Kappa<0.20 means poor strength of agreement. Values between 0.81 and 1, means a very good strength of agreement). This higher variation means that only based on articular radiographic images, it is almost impossible to define the rehabilitation position.
Despite this, the results may be of clinical relevance, because in dynamic registration, all the distances were smaller, more consistent and equidistant. It seems that condyles stayed in a closer position to articular fossa, for sagittal and frontal view. Based on these results, we can suspect that with dynamic registration the condyles were in a centred position in the articular fossa and this fact can be observed in both sides simultaneously. Comparatively to static registration, values were more homogeneous, when we consider the two, or each side separately.
Anterior and superior spaces are smaller for dynamic registration, due to the fact that the static method was influenced by jaw manipulation and muscular symmetry. Condylar position during dynamic registration may promote higher muscular symmetry.
In 2014, some authors18 analyzed in magnetic resonance imaging (MRI) the effects of different registration positions on the condyle–disc position, in maximal intercuspation, Gothic Arch Tracing and retruded contact position (RCP). Dynamic Registration position ensures the widest posterior space for the retrodiscal tissues and the slightest sagittal difference between condyle zenith and articular fossa. The results obtained in our study were in concordance with these findings. Gothic Arch Tracing seems to best fulfil this criterion of a physiologic or centric condylar position, with symmetry between condyles.
A strong correlation between the posterior and superior measurements was ascertained, for both condyles and the two methods of determining the intermaxillary relationship. This could be a sign of antero-inferior sliding of the condyles in the joint. Thus, an inverse relationship would be expected between the posterior and/or superior measurements with their corresponding anterior measurements. Despite the fact that there is a trend in this direction, it was not possible to establish a statistically significant correlation.
Values for right and left condyles for dynamic registration had a smaller variation and also a stronger correlation between them. This means that for Gothic Arch Tracing a higher symmetry exists.
For static registration, a greater heterogeneity of results was seen. This could be possibly due to the fact that in static registration, wax rims could promote higher mucosal pressure on one side, resulting in a condylar displacement. In dynamic registration, less pressure should be expected, because the forces are concentrated on a central pin and not on a wax block.
For dynamic registration, only the patient participated in his mandibular movement; left condyle reveals a tendency to stay more posterior, even for static and dynamic registration, but with a higher difference in static. This could be explained during static registration, because the operator exerts force to the posterior and left direction when manipulating, for the reason that all the operators were right-handed.
Results demonstrated a correspondence between the angle of the articular eminence and the length of superior articular space: the higher the angle the bigger this length is.
An author25 stated that the steeper the eminence, more the condyle is forced to move inferiorly as it shifts anteriorly. This could be a physiological position of comfort.
Another important fact ascertained in this clinical investigation was that a significant correlation between the anterior position of the right condyle and the period of edentulism was found, which was also in concordance with other authors.17
Regardless the promising results presented in the study, care should be taken in the interpretation in the results, due to the limited number of patients.
ConclusionFrom the results of this study, we can conclude that the success of these procedures was not dependent on the method used, because no significant discrepancies were seen between CBCT images, when using static or dynamic registration methods. Nevertheless, dynamic registration values showed more reliability and accuracy in defining a symmetric and equilibrated CR position. It seems that this method reproduces a physiologic condylar position.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Conflict of interestThe authors have no conflicts of interest to declare.