

We analyzed the 124 deaths reported in Portugal form flu pandemic. The estimated mortality rate was 1.17/100000 population. 60% were males, the average age was 47.6 and 66.1% had at least one risk factor. Chronic lung and heart diseases were the most common risk factors. Viral pneumonia was the major cause of death. 11% of the deceased had no treatment with neuraminidase inhibitors and none was vaccinated against the pandemic strain of flu. Compared to average life expectancy, we estimated that 3859 years of potential life were lost.
In the future, we should work on improved strategies for risk communication for health professionals and general public.
Em Portugal, durante a pandemia de gripe A(H1N1) 2009 foram reportados 124 óbitos. A taxa de mortalidade estimada foi de 1,17/100000 habitantes. 60% dos falecidos eram do sexo masculino, a média das idades foi de 47,6 anos e em 66,1% havia pelo menos um factor de risco. As doenças crónicas respiratórias e cardíacas foram os factores de risco mais comuns. A pneumonia viral primária foi a principal causa de morte. 11% dos falecidos não receberam terapêutica com antivíricos e nenhum foi vacinado com a vacina pandémica. Em relação à esperança média de vida, os anos potenciais de vida perdidos foram 3859 anos.
No futuro em circunstâncias semelhantes, devemos melhorar as estratégias de comunicação do risco para os profissionais de saúde e população em geral.
Um relatório preliminar deste estudo foi publicado na Revista Portuguesa de Medicina Intensiva (Rev Port Med Int 2010; 17(4):11–19). A preliminar report of this study has been published in Revista Portuguesa de Medicina Intensiva (Rev Port Med Int 2010; 17(4):11–19). This report is dedicated to the families of victims of pandemic influenza.
Portugal activated their Contingency Plan1 for the flu pandemic on 24 April 2009 and it remained in force until 21 August 2009. The first case notified in the country was diagnosed on 29 April 2009.
As in other countries in Portugal all deaths associated with Flu A (H1N1) 2009 were reported. Throughout the pandemic only related deaths were mandatory to be registered. From the start of the Contingency Plan through to the end of the pandemic, which was officially declared over by the World Health Organization (WHO) on 10 August 2010, there were 124 deaths. The first occurred on 23 September 2009 and the last on 3 March 2010. The results of our analysis of reported deaths in Portugal from the flu pandemic have a great deal to contribute to our understanding of the characteristics of infection from the flu virus A (H1N1) 2009, and can help to improve standards of preparation for future pandemics.
ObjectivesTo make a thorough examination of the deaths from the flu pandemic according to sex, age group, risk factors from severe disease, hospital admission, length of hospital stay, causes of death, antivirus treatment, vaccination status and the estimated mortality rate and years of expected life lost.
Materials and methodsAll deaths were confirmed by laboratory tests using RT-PCR. We analyzed the data from the database of the Directorate-General for Health (Direção-Geral da Saúde [DGS]) of the Ministry of Health, which was subsequently validated by telephone, email or by visits from representatives of DGS to the hospitals.
The following were considered severe risk factors in the context of flu pandemic (H1N1) 20092:
- 1.
No risk factors
- 2.
Pregnancy/postpartum (≤15 days after birth)
- 3.
Chronic lung disease (e.g. asthma, COPD, cystic fibrosis)
- 4.
Chronic kidney disease
- 5.
Chronic heart disease (excluding isolated Arterial Hypertension)
- 6.
Chronic liver disease
- 7.
Chronic hematologic disease (e.g. hemoglobinopathies, excluding oncological disorders)
- 8.
Neurological disease/chronic neuromuscular disease
- 9.
Chronic metabolic disease (e.g. diabetes)
- 10.
Cancer (e.g. solid and haematological tumours)
- 11.
Immunosuppression (e.g. congenital, associated with HIV and organ transplant, post-chemotherapy, immunotherapy, steroids at immunosuppressant levels.)
- 12.
Morbid obesity (<10 years old: IMC ≥25; ≥10 and <18 years old: IMC ≥35; ≥18 years old: IMC ≥40)
- 13.
Chronic therapy with salicylates in patients aged <18 years
The following were considered as causes of death:
- 1.
Viral infection, including primary viral pneumonia and other causes of viral infection (e.g. encephalitis or myopericarditis)
- 2.
Secondary bacterial pneumonia (concurrent or as a result of viral infection and not contracted in hospital)
- 3.
Decompensation due to comorbidity
- 4.
Complications or intercurrent disease during hospitalization (e.g. haemorrhage, stroke, pulmonary embolism, barotraumas, nosocomial infections)
Figures from the Institute of National Statistics for the Portuguese population on 31/12/20083 were used to calculate the mortality rate. To calculate the expected years of life lost, the age of each individual at the time of death was subtracted from the average life expectancy at birth in Portugal for the three-year period 2007–2009, specified by sex.4–7 The number of years of potential life lost per 100000 population was calculated by dividing the total number of years lost by the estimate of the Portuguese population younger than the average life expectancy.
To analyze the data we used PASW Statistics® version 18 and Microsoft Excel 2003. The comparison of the mean age was calculated using the p value of Student's t test and ANOVA. We considered all non-significant differences in those where the p-value was greater than 0.05.
ResultsIn Portugal 124 deaths caused by the flu pandemic were reported. With the exception of one death which occurred at home, all the patients (123: 99.2%) died in National Health Service hospitals. The death toll represents a mortality rate of 1.17 per 100000 population. There were no deaths among health professionals.
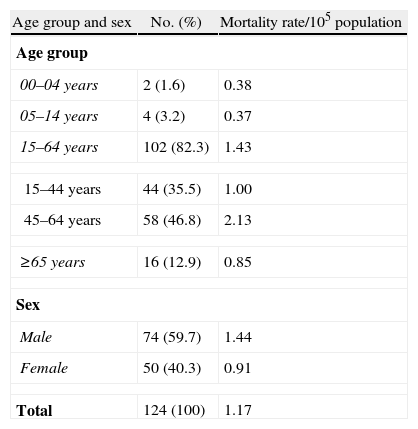
Age and sexThere were 74 male deaths (59.7%) and 50 female (40.3%). The average age of death was 47.6 and the median age 49, there was no statistically significant difference (p=0.873) between the sexes, the average and median ages were 47.9 and 50 for males and 47.3 and 47 for females, respectively. The youngest who died was 5 months old and the oldest was aged 88. Almost half the deaths (46.8%) happened between the ages of 45 and 64 and around ⅓ (35.5%) were between the ages of 15 and 44. Only 16 (12.9%) deaths occurred in the age group ≥65 (Table 1).
Distribution of deaths from flu pandemic (H1N1) 2009 according to age group, sex and mortality rate per 100000 population, from April 2009 to August 2010, Portugal.
| Age group and sex | No. (%) | Mortality rate/105 population |
| Age group | ||
| 00–04 years | 2 (1.6) | 0.38 |
| 05–14 years | 4 (3.2) | 0.37 |
| 15–64 years | 102 (82.3) | 1.43 |
| 15–44 years | 44 (35.5) | 1.00 |
| 45–64 years | 58 (46.8) | 2.13 |
| ≥65 years | 16 (12.9) | 0.85 |
| Sex | ||
| Male | 74 (59.7) | 1.44 |
| Female | 50 (40.3) | 0.91 |
| Total | 124 (100) | 1.17 |
Of the 124 deaths, 82 (66.1%) had at least one risk factor for serious disease. The average age for these patients was 48.5, which was higher than the 46.0 for those who had no risk factor (n=42; 33.9%), but without statistical significance (p=0.471).
Of the 82 patients with risk factors, 52 (63.4%) had only one risk factor and 30 (36.6%) had more than one risk factor. Of the 6 (7.3%) cases that had 3 or more risk factors all of them were over 45. Among the paediatric cases (aged <18), 6 (85.7%) of the 7 who died had, at least, 1 risk factor. The presence of risk factors was 68.8% in the age group ≥65 and was lowest (56.8%) among the age group 15–44.
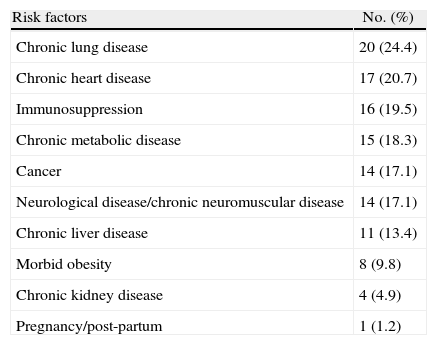
Lung disease and chronic heart disease were the most common risk factors identified in respectively 20 (24.4%) and 17 (20.7%) patients, followed by immunosuppression in 16 (19.5%) cases (Table 2). Among the paediatric patients the most common risk factor was neuromuscular disease, which was present in 4 (66.7%) of the 6 children who had risk factors.
Number and percentage of deaths from flu pandemic (H1N1) 2009, according to risk factor, from April 2009 to August 2010, in Portugal.
| Risk factors | No. (%) |
| Chronic lung disease | 20 (24.4) |
| Chronic heart disease | 17 (20.7) |
| Immunosuppression | 16 (19.5) |
| Chronic metabolic disease | 15 (18.3) |
| Cancer | 14 (17.1) |
| Neurological disease/chronic neuromuscular disease | 14 (17.1) |
| Chronic liver disease | 11 (13.4) |
| Morbid obesity | 8 (9.8) |
| Chronic kidney disease | 4 (4.9) |
| Pregnancy/post-partum | 1 (1.2) |
Obesity classes I and II (IMC: ≥30 and <40) were not considered a risk factor. However, it was mentioned in 18 cases, 12 of which had no risk factor. In the group with chronic metabolic diseases only one suffered from diabetes mellitus. Of the 14 cases with chronic neurological/neuromuscular disease, three had Down's syndrome.
Admission to hospital and to ICUOf 124 deaths, 123 (99.2%) occurred in National Health Service hospitals. The other death happened at home. The average length of internment for those who died was 15.0 days, the median was 11, the maximum was 68 and the minimum 0 days. The average length of internment was 5.2 days for children <18 years, 15.5 days for patients between 18 and 64 years and 17.1 days for those ≥65. For patients with no risk factor the average length of internment was 19.9 days and for those with risk factors it was 13.0 days.
Of the 123 patients hospitalized, 95 (77.2%) were treated in Intensive Care Units. 94 (98.9%) of these patients were treated with invasive mechanical ventilation. Three of the patients also had ECMO (Extra Corporeal Membrane Oxygenation) out of a total of 6 patients who have been treated with this procedure in Portugal during flu pandemic.
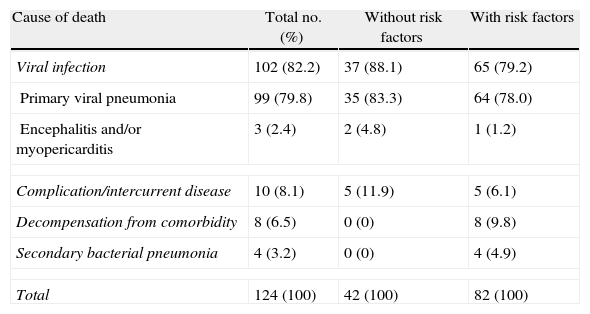
Cause of deathPrimary viral pneumonia diagnosed in 99 (79.8%) of the 124 patients, was the most common cause of death, followed by complications/intercurrent disease while in hospital and decompensation caused by comorbidity, which occurred in 8.1 and 6.5% of cases respectively. Secondary bacterial pneumonia was diagnosed in only 4 (3.2%) cases (Table 3).
Number and percentage (in descending order) of deaths from flu pandemic (H1N1) 2009, according to the cause of death; the total and the presence or absence of risk factors, from April 2009 to August 2010, Portugal.
| Cause of death | Total no. (%) | Without risk factors | With risk factors |
| Viral infection | 102 (82.2) | 37 (88.1) | 65 (79.2) |
| Primary viral pneumonia | 99 (79.8) | 35 (83.3) | 64 (78.0) |
| Encephalitis and/or myopericarditis | 3 (2.4) | 2 (4.8) | 1 (1.2) |
| Complication/intercurrent disease | 10 (8.1) | 5 (11.9) | 5 (6.1) |
| Decompensation from comorbidity | 8 (6.5) | 0 (0) | 8 (9.8) |
| Secondary bacterial pneumonia | 4 (3.2) | 0 (0) | 4 (4.9) |
| Total | 124 (100) | 42 (100) | 82 (100) |
The most common cause of death in the 7 children aged <18was primary viral pneumonia in 6 cases (85.7%). In the other case the cause of death was decompensation from chronic respiratory disease.
Neuraminidase inhibitor therapyIn 6 cases out of the 124 deaths it is not known if they were treated with neuraminidase inhibitors. We do know that it was used with 105 patients (89.0%), but it was not possible to establish the length of time between the onset of symptoms and starting the therapy. They were all given oseltamivir, and 3 were also given zanamivir intravenously. 13 (11.0%) patients had no antivirus therapy; 7 of these died in the first 24h after admission and in 9 cases laboratory confirmation of disease (RT-PCR) was post-mortem.
Vaccination status82 (66.1%) of the patients had risk factors and therefore should have been vaccinated. One of the patients contracted the disease in the first week after being vaccinated and two, with serious immunosuppression (hematologic malignancy) had fallen ill in the interval between the 1st and 2nd vaccines. None of the other 79 who had risk factors had been vaccinated. In 64 of these cases it was possible to work out how long it would have been between the date they were admitted to hospital and the completion of the vaccination scheme, if they had been vaccinated according to guidelines for groups at risk, according to the schedule of national vaccinations.
The length of time was as follows:
- -
for 29 (45.3%), more than or equal to 4 weeks;
- -
for 5 (7.8%), more than 3 weeks but less than 4;
- -
for 30 (46.9%), less than 3 weeks.
3859 was the estimated figure for the number of potential years of life lost, which is equivalent to 40.0 years per 100000 population. The average number of potential years of life lost for each person who died was 31.
DiscussionIn Portugal notification of death from flu pandemic was mandatory. This study covers the 124 reported deaths which were confirmed by laboratory tests RT-PCR. However, we must accept that there might have been other deaths, where this diagnosis was not considered and so patients were not tested or cases of false negative results due to technical problems in sample collection or problems with the quality of laboratory testing. Despite these possible limitations, which would have also been true of other studies of the same kind, we are confident that the DGS database is reliable and if it does not cover all, it does include the great majority of the deaths in Portugal.
It is the first time in a flu pandemic that only the death toll, confirmed by laboratory tests, has been recorded, which may help to explain discrepancies in comparisons with the impact of earlier pandemics. It should also be noted that laboratory testing for confirmation is not used to assess the mortality rate during annual epidemics of seasonal flu.
These 124 deaths represent a mortality rate of 1.17/100000 population, about a third of the estimate of the ECDC (up to 3 per 100000 population) in its “reasonable worst case scenario”.8 This specific mortality rate, although higher than the average for countries in the European Union,9 is within the reference ranges for this region, and it is also higher than the estimates for the United States (USA) of 0.97/100000.10
Without knowing the exact number of patients who were affected and symptomatic we cannot establish an overall case fatality rate or the case fatality rate for symptomatic illness. In the USA11 and United Kingdom,12 the case fatality rate for symptomatic illness has been estimated at 0.048% and 0.026%, respectively.
The average age of patients who died was 47.6, with a slight predominance of males (59.7%); there was no significant difference in average ages of the sexes. The age group most affected was 15–64, in particular the subgroup between 45 and 64 which had a mortality rate of 2.13/100000 population. The overrepresentation of males was noted in other European countries, for example France13 (57%) and Holland14 (55%). The fact that it affected younger age groups is also in line with other studies, the average age at death in the United Kingdom15 was 43 and it was 52 in Holland.14
In Portugal, 87.1% of deaths happened in the under 65s, which corroborated the global estimate that approximately 90% of those who died were under 65.16 This contrasts significantly with figures for seasonal flu in this country, where more than 80% of deaths occur in people who are 75 and over.17
25–50% of those who died were estimated to have no risk factors for the flu pandemic.16 In Portugal 33.3% of deaths occurred in people with no risk factor; in United Kingdom it was 23%.15 Although the values found in our country are within the reference ranges, the variations found could have been partially influenced by the fact that the methodologies used were not uniform and different weight was given to some of the risk factors, for example, obesity. In this analysis morbid obesity (BMI≥40 in adults and the corresponding value for patients <18 years) was considered a risk factor. If non-morbid obesity is also included (IMC≥30 in adults with a corresponding value for children) means that there were only 23.6% patients without a risk factor.
The distribution of risk factors that were found in the Portuguese population is very much the same as the international picture with the exception of pregnancy/post-partum. Only one patient in Portugal died in these circumstances (0.8% of total deaths), whereas the values described in the literature in other countries were between 6% and 9%.18,19 In our study it was not possible to come to any conclusions about this difference. Only one (14.3%) of the children did not have a risk factor and almost half (43.2%) of the deaths between 15 and 44 years did not present risk factors. In the United Kingdom, it was also among those between 25 and 44 years of age that there was the highest percentage (32%) of deaths without risk factors.15
Diffuse viral pneumonitis was the most common cause of death (79.8%), which was independent of age group or the existence of risk factors. This very high percentage of cases of primary viral pneumonia, usually associated with ARDS (Acute Respiratory Distress Syndrome), severe hypoxaemia, septic shock and kidney failure, matches what is described in other studies, for example in Australia18 and Canada19 and probably explains why so many of the patients were put on mechanical ventilation and had complications and intercurrent diseases (8.1%). Throughout the period of the pandemic although there was often a considerable delay before hospital admission there were no reports of shortage of hospital beds in the ICUs.
Data from other studies indicate percentages of 26–38% for deaths from bacterial pneumonia,18–21 whereas here according to our data it was only 3.2%; we did not have enough information to explain this disparity, but it could be related to the effectiveness of the diagnosis by microbiological testing and antibiotic treatment prior to the collection of samples.
In 11.0% of deaths there had been no specific treatment with neuraminidase inhibitors. In a similar study in South Korea this percentage was 13%22 and 24% for patients who died in hospital in the USA in September and October 2009.23 In our series, even though the majority died in the first 24h of hospitalization, the delay in starting antiviral treatment in the serious cases, because of, for example, waiting for confirmation of the results of laboratory tests, can be considered a breach of the national technical guidelines issued by the DGS.
In addition, for the first time in the history of pandemics, there was a vaccine available. In Portugal a pandemic vaccine with an adjuvant (Pandemrix) was available from 26 October 2009 according to a schedule set down according to risk factors. None of the people who died had been vaccinated for pandemic flu, not even those whose risk factors should have made them a priority. In a study of 25 adults aged between 20 and 48 who were given a vaccine similar to the one available in Portugal, the levels of seroconversion were 78% and 88% at 14 and 21 days, respectively.24 In our study more than 40% of those with a risk factor and who died could have been vaccinated in time to prevent serious illness or death, but this did not happen. On the contrary the national technical guidelines were not respected and there was a lack of communication and proper understanding of the risks involved on the part of health professionals and the general public.
Using estimates as a base for potential years of life lost allows us to have a different perspective on the implications of the pattern of death which we do not get by just looking at the numbers of deaths, in isolation.25 In this way we can see that in Portugal the number of potential years of life lost was 3859 years, which corresponds to 40.0 years per 100000 population, giving us a clearer picture of the effect of the 124 registered deaths.
ConclusionThe mortality rates in Portugal were in general comparable to those found in other developed countries. However in future crises the Public Health Services should be prepared to impose mandatory reporting for all the most serious cases, for example admission to a hospital ward or to an ICU, which would be in line with best practice in epidemiology, both clinical and resource management. Equally there should be measures in place to improve risk communication strategies for health professionals and the general public. An analysis of potential years of life lost, because it shows the impact of death in real terms rather than looking at the bald number of actual deaths, gives more insight into the effect of these deaths, and for this reason should be included wherever possible in the evaluation of the effect of illness that can be classed as pandemics.
Conflicts of interestThe authors have no conflicts of interest to declare.
The authors express their appreciation for the Portuguese Public Health Medical Doctors, General Practitioners and Hospital Specialists, who with dedication and sense of mission played a key role in the containment and mitigation of pandemic influenza.
The authors would like to thank all the institutions that took part in the national register of deaths and Drs. Francisco George, Graça Freitas, José Robalo, Ana Leça, Teresa Fernandes and Margarida Mesquita for their collaboration.