




Suicide is a current public health problem and among the main causes of mortality in adolescents and young adults. The main goal of this study was to analyse suicidal ideation in a representative sample of Spanish adolescents. Specifically, the prevalence rates of suicide ideation, the psychometric properties of the Paykel Suicide Scale (PSS) scores, and the socio-emotional adjustment of adolescents at risk for suicide were analysed.
Material and methodsThe sample consisted of 1664 participants (M=16.12 years, SD=1.36, range 14–19 years), selected by stratified sampling by clusters. The instruments used were the PSS, the Strengths and Difficulties Questionnaire, the Personal Wellbeing Index-School Children, and the Oviedo Infrequency Scale.
ResultsThe results showed that 4.1% of the sample indicated that they had tried to commit suicide in the previous year. Statistically significant differences were found according to gender but not according to age in the PSS mean scores. The analysis of the internal structure of the PSS showed that the one-dimensional model presented excellent goodness of fit indexes. This model showed measurement invariance across gender. The reliability of the scores, estimated with ordinal alpha, was 0.93. Participants who reported suicide ideation showed poorer mental health status and lower life satisfaction compared to the non-suicide ideation group.
ConclusionsSuicidal ideation is present during adolescence and is associated with poor subjective well-being and increased emotional and behavioural problems. PSS seems to show adequate psychometric behaviour to assess suicidal ideation in adolescents. These findings have clear implications, both in health and education systems, to improve the promotion of emotional well-being and prevention of psychological and psychiatric problems in this sector of the population.
El suicidio es un problema sociosanitario de primer orden. El propósito de este estudio fue analizar la ideación suicida en una muestra representativa de adolescentes españoles. Concretamente, se examinó las tasas de prevalencia, se validó la Escala Paykel de Ideación Suicida (Paykel Suicide Scale, PSS) y se analizó el ajuste socioemocional de aquellos adolescentes con ideación suicida.
Material y métodosLa muestra la formaron 1.664 participantes (M=16,12 años; DT=1,36; rango 14-19 años) seleccionados mediante muestreo estratificado por conglomerados. Los instrumentos empleados fueron la PSS, el Strengths and Difficulties Questionnaire, el Personal Wellbeing Index–School Children y la Escala Oviedo de Infrecuencia de Respuesta.
ResultadosEl 4,1% de la muestra informó haber intentado quitarse la vida en el último año. Se encontraron diferencias estadísticamente significativas en las puntuaciones medias de la PSS en función del género pero no en función de la edad. El modelo unidimensional de la PSS presentó excelentes índices de bondad de ajuste y se mostró invariante en función del género. La fiabilidad de las puntuaciones de la PSS, estimada con el alfa ordinal, fue de 0,93. Los participantes con ideación suicida informaron de un peor estado de salud mental y menor satisfacción con la vida respecto al grupo de comparación.
ConclusionesLa ideación suicida se encuentra presente en población adolescente y se asocia a un peor bienestar emocional subjetivo y a mayores problemas emocionales y comportamentales. La PSS parece mostrar un adecuado comportamiento psicométrico para evaluar la ideación suicida en adolescentes. Estos resultados tienen claras implicaciones, tanto a nivel sanitario como educativo, de cara a mejorar la promoción del bienestar emocional y la prevención de los problemas psicológicos y psiquiátricos en este sector de la población.
Mental disorders are among the main causes of associated disability and disease burden in the 10–24 year old age group.1 Suicide stands out within this set of problems due to its impact, severity and associated social and healthcare cost. Suicide is one of the main causes of loss of years of life due to premature death,2,3 and it is the second causes of death among adolescents and young adults aged from 15 to 29 years old.4 The worldwide suicide rate in 2012 stood at 11.4 per 100,000 inhabitants. In that specific year in Spain the standardised suicide rate was 8.1 per every 100,000 inhabitants. In the period 2000–2012 42,905 individuals over the age of 15 years old died due to suicide. The average annual incidence during this period was 95 suicides/million inhabitants. The highest rates of mortality due to suicide occurred in the south and North West of Spain.5 According to the National Statistics Institute6 in 2013 310 children and young people under the age of 30 years old took their own lives. This datum amounts to 7.77% of the total number of suicide victims. In the same year the suicide rates in the young population aged from 15 to 19 years old were 2.65 for every 100,000 inhabitants.7
The impact of this problem is not restricted to rates of consummated suicide, as it also arises due to suicidal ideation or previous attempted suicides. Suicidal ideation and previous attempts are often precedents of a consummated suicide. For example, Gabilondo et al.8 found that the probability of attempting suicide among those who had suicidal ideation (who had prepared a plan for suicide) was clearly higher (73%) than it was for those who had no plan (14.4%). The prevalence of suicidal ideation during life in Spain stands at 4.4–7.8%, while for attempted suicide it is 1.5–1.8%.8,9 The result differ slightly in the adolescent population respecting those found for the adult population.10–15 For example, in a multicentre study in different European countries using the Paykel Suicide Scale, PSS)16 a prevalence of suicidal ideation was found in adolescents to stand at 32.3%, while the prevalence of attempted suicide was 4.2%.10 In Spain, using the PSS in a representative sample of adolescents, it was found that the prevalence of suicidal ideation was 7.4%.11 The heterogeneity found in rates may be due, among other factors, to the measuring instrument and statistical criterion used to define suicidal ideation.
Suicidal behaviour and ideation seem to vary depending on sociodemographic variables such as sex and age.8,10,17 More specifically, men have a higher number of consummated suicidal behaviours than women (at a ratio of 3:1 in developed countries). At world level, the corresponding figures are 15 men per 100,000 men and 8 women per 100,000 women.3 Nevertheless, the ratio of attempted suicides is 1:3 in favour of women. Moreover, women tend to have a higher rate of suicidal ideation.8 Regarding age, the older and younger age groups have higher rates of consummated suicide.3 Suicidal plans or ideas gradually decrease with increasing age.8 In samples of adolescents, suicidal ideation as well as attempted suicide seem to be more common in girls that they are in boys, and they increase as they grow older.10
Reducing these rates of prevalence and the associated costs involves, among other aspects, the design and implementation of mental health promotion and prevention strategies (e.g., universal, selective and indicated).18 An appropriate preventative strategy requires correct detection and identification on the one hand, so that a tool is needed that makes it possible to reliably and validly evaluate suicidal ideation and behaviour. On the other hand empirically validated effective treatments are required. It is possible to find many suicidal behaviour evaluation tools in the literature, together with their associated constructs.19–22 More specifically, evaluation of the risk of suicide is not a simple task, given that many factors are involved (e.g., the tests used and its multifactorial aetiology, etc.). It is possible that due to its brevity the PSS stands out from the broad range of existing instruments.16 This scale was designed to evaluate suicidal ideation behaviour, although it evaluates thoughts of death, suicidal ideation and previous attempts. It is composed of a total of 5 items with a dichotomic yes/no system of answering. This tool has been used in patient studies23 as well as in international studies in which Spanish adolescents take part (the SELYE project)10,11; nevertheless, its psychometric properties are not yet known in Spain.
Scientific evidence shows that suicidal behaviour is associated with mental health problems in adolescents. These include depressive episodes, attenuated psychotic experiences, substance abuse and consumption and bullying at school, to mention just a few.11,24–28 Thus those adolescents considered to be at risk, based on plans for suicide or previous attempts, have a high rate of psychological and physical symptoms and comorbid disorders. It is therefore necessary to analyse the mental health state of younger individuals before implementing an early detection and intervention programme for those individuals who are at risk. The eventual purpose is to develop skills that make it possible to reduce and/or prevent suicidal ideation and consummated suicide, with the consequent positive effects at personal, family, social and healthcare levels.
Few empirical studies have been undertaken to date with the aim of analysing and understanding suicidal ideation in representative samples of Spanish adolescents. Additionally, no information is available about the psychometric properties of the PSS in Spain. There is a lack of knowledge about the mental health and emotional wellbeing of those young people who describe suicidal ideation and/or previous attempted suicide. Within this research context, the general aim was to study suicidal ideation in a representative non-clinical sample of Spanish adolescents. Its specific objectives were: (a) to examine the prevalence of suicidal ideation and its association with sex and age; (b) to analyse the psychometric properties of the PSS; and (c) to study the emotional and behavioural difficulties of those participants who report suicidal ideation and/or previous attempted suicide.
MethodParticipantsWith the purpose of guaranteeing the representative nature of the sample, stratified random sampling was used, in groups and at classroom level in a population of approximately fifteen thousand students in the Autonomous Community of La Rioja. The strata were created on the basis of schools (state/private-semi-private) and school level (basic education, secondary or technical college), where the probability of extraction of the classroom from the school was determined depending on the number of students.
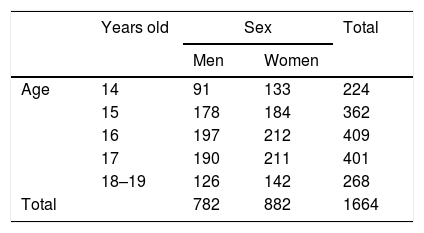
The initial sample was composed of 1881 students, eliminating those participants who had a high score in the Oviedo Scale of Response Infrequency (more than 3 points) (n=104) or an age older than 19 years (n=170). In this way a total of 1664 students were selected and took part in the study. They were 782 males (47%) and 882 (53%) females, belonging to 34 schools and 98 classrooms. Their average age was 16.12 years old (TD=1.36), ranging from 14 to 19 years old. Due to the low number of participants aged 19 years old it was decided to combine them with the group aged 18 years old. The distribution of the total sample according to sex and age is shown in Table 1.
The distribution according to participant nationality was as follows: 89.9% Spanish, 3.7% Latin American (Bolivia, Argentina, Colombia and Ecuador), 0.7% Portuguese, 2.4% Rumanian, 1% Moroccan, 0.7% Pakistani and 2% other nationalities.
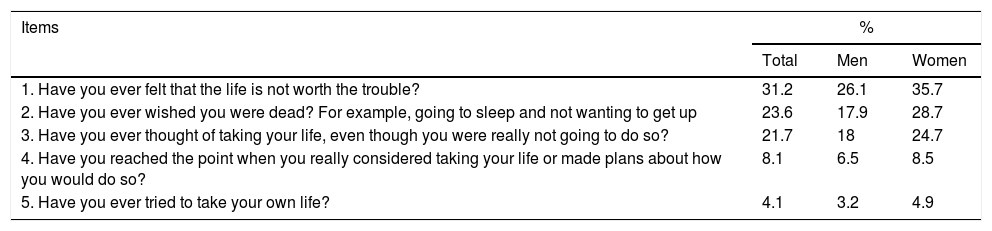
InstrumentsThe Paykel Suicide Scale16This tool was designed to evaluate suicidal ideation. More specifically, it evaluates thoughts about death (items 1 and 2), ideation (items 3 and 4) and attempted suicide (item 5). Although as its name indicates this tool evaluates suicidal ideation, the fact is that some of its items ask about suicidal behaviours (e.g., item 5). It is composed of a total of 5 items with a Yes/No dichotomic response system (scoring 1 and 0, respectively). Scores run from 0 to 5. The time frame for the questions is the last year. The higher the score, the greater the risk and severity of suicidal ideation. The items of the PSS are shown in Table 2.
The percentage of students who answered affirmatively to items in the Paykel Suicidal Ideation Scale, in the total sample and according to sex.
| Items | % | ||
|---|---|---|---|
| Total | Men | Women | |
| 1. Have you ever felt that the life is not worth the trouble? | 31.2 | 26.1 | 35.7 |
| 2. Have you ever wished you were dead? For example, going to sleep and not wanting to get up | 23.6 | 17.9 | 28.7 |
| 3. Have you ever thought of taking your life, even though you were really not going to do so? | 21.7 | 18 | 24.7 |
| 4. Have you reached the point when you really considered taking your life or made plans about how you would do so? | 8.1 | 6.5 | 8.5 |
| 5. Have you ever tried to take your own life? | 4.1 | 3.2 | 4.9 |
The Strengths and Difficulties Questionnaire (SDQ) is a measuring instrument used to evaluate behavioural and emotional difficulties as well as social capacities.30 It has been used as a mental health state screening and epidemiological analysis tool in populations of children and the young.31,32
The SDQ is composed of 25 items with a Likert 3 option response format: 0 (No, never), 1 (Sometimes) and 2 (Yes, always). The items are grouped in 5 subscales (each with 5 items): emotional difficulties, behavioural problems, hyperactivity problems, problems with schoolmates and prosocial behaviour. The first 4 subscales form a total score of difficulties: the higher the score, the higher the level of emotional and behavioural difficulties. The exception is the prosocial behaviour subscale, where a lower score corresponds to poorer behavioural adjustment.
The metric properties of the SDQ have been analysed in previous national and international studies.33,34 In this work the estimated reliability of the scores using Cronbach's alpha for the total difficulties was 0.75.
The Personal Wellbeing Index–School Children35,36The Personal Wellbeing Index–School Children (PWI-SC) was developed to evaluate the subjective wellbeing of children and school-age adolescents.35,36 The authors of the PWI-SC basically consider emotional wellbeing to consist of cognitive evaluation of the quality of an individual's own experiences. Subjective emotional wellbeing may be considered an indirect indicator of quality of life.
The PWI-SC is composed of a total of 8 items, and the response options run from 0 (Very unhappy) to 10 (Very happy). The items in the PWI-SC evaluate subjective satisfaction with a specific area of life in a relatively generic and abstract way. The first item in the scale analyses “life as a whole”. The other 7 items include satisfaction with: health, level of life, things achieved in life, how safe they feel, the groups of people they are a part of, surety about the future and relationships with other people. The overall scale is the result of adding all 7 items (except item 1). The total score may therefore vary from 0 to 70 points.
The PWI-SC has displayed appropriate psychometric properties in previous national and international studies.35,37,38 In this work the estimated reliability of the scores using Cronbach's alpha for the total score was 0.83.
The Oviedo Response Infrequency Scale39The Oviedo Response Infrequency Scale (INF-OV) was developed to detect those participants who have responded randomly, semi-randomly or dishonestly. The INF-OV is a self-reporting measuring instrument composed of 12 items in a Likert-type format of 5 categories of degree of agreement. They run from 1 (Completely disagree) to 5 (Completely agree). Once the items have been dichotomised, the students who score more than 2 items incorrectly are eliminated from the study. The INF-OV has been used in previous works.40
ProcedureThis research was approved by the General Board of Education of La Rioja Government and the La Rioja Clinical Research Committee (CEICLAR) (reference PI-221).
The instruments were administered by computer and collectively in groups of from 10 to 30 participants. One classroom in each school was used, after it had been prepared for this purpose. The instruments were always administered during school hours. Subjects were always informed of the confidentiality of their answers, as well as the voluntary nature of participation, and no gratification of any kind was given for collaborating in the study. Whenever necessary informed consent was requested to authorise the participation of an adolescent in this research.
This study took place within the framework of broader research into emotional wellbeing during adolescence. This evaluated other questions such as neurocognitive functioning, bullying at school and the risk of a severe mental disorder.
Data analysisThe following data analyses were performed to study the proposed objectives.
Firstly the prevalence of suicidal ideation was examined, in the total sample as well as according to sex and age. For this the percentages of affirmative answers were computed for each item in the PSS as well as in the total score. Additionally, to analyse the existence of statistically significant differences in the scores of the PSS the chi-squared and t-tests for independent samples were used.
Secondly, the psychometric properties of the PSS scores were analysed. To obtain evidence of internal structure validity different factorial analyses were undertaken to confirm this. There is no information in previous literature about other possible dimensional models, so that only a one-dimensional model was subjected to testing. The Weighted Least Squares Mean and Variance Adjusted (WLSMV) calculation method was used. The goodness of fit indexes used were: the comparative fit index (CFI), the Tucker–Lewis Index (TLI), the root mean square error of approximation (RMSEA), and its confidence interval at 95% (CI 95%), together with the weighted residual mean square root (WRMR). For there to b ea good fit in the model data, the CFI and TLI values had to be greater than 0.95, and the RMSEA values had to be lower than 0.08 for a reasonable fit, and lower than 0.05 for a good fit.41,42
Invariance of measurement was also analysed as a function of sex for the one-dimensional model. The invariance of measurement or factorial equivalence checks whether the factorial structure of the measuring instrument is equivalent depending on the groups which are being compared.43 For this the successive parameter restriction steps were followed. Considering the dichotomic nature of the scores the configural measurement invariance and the strong measurement invariance were subjected to testing.44 The strong invariance model is conceptually equivalent to the study of the differential functioning of the item.45
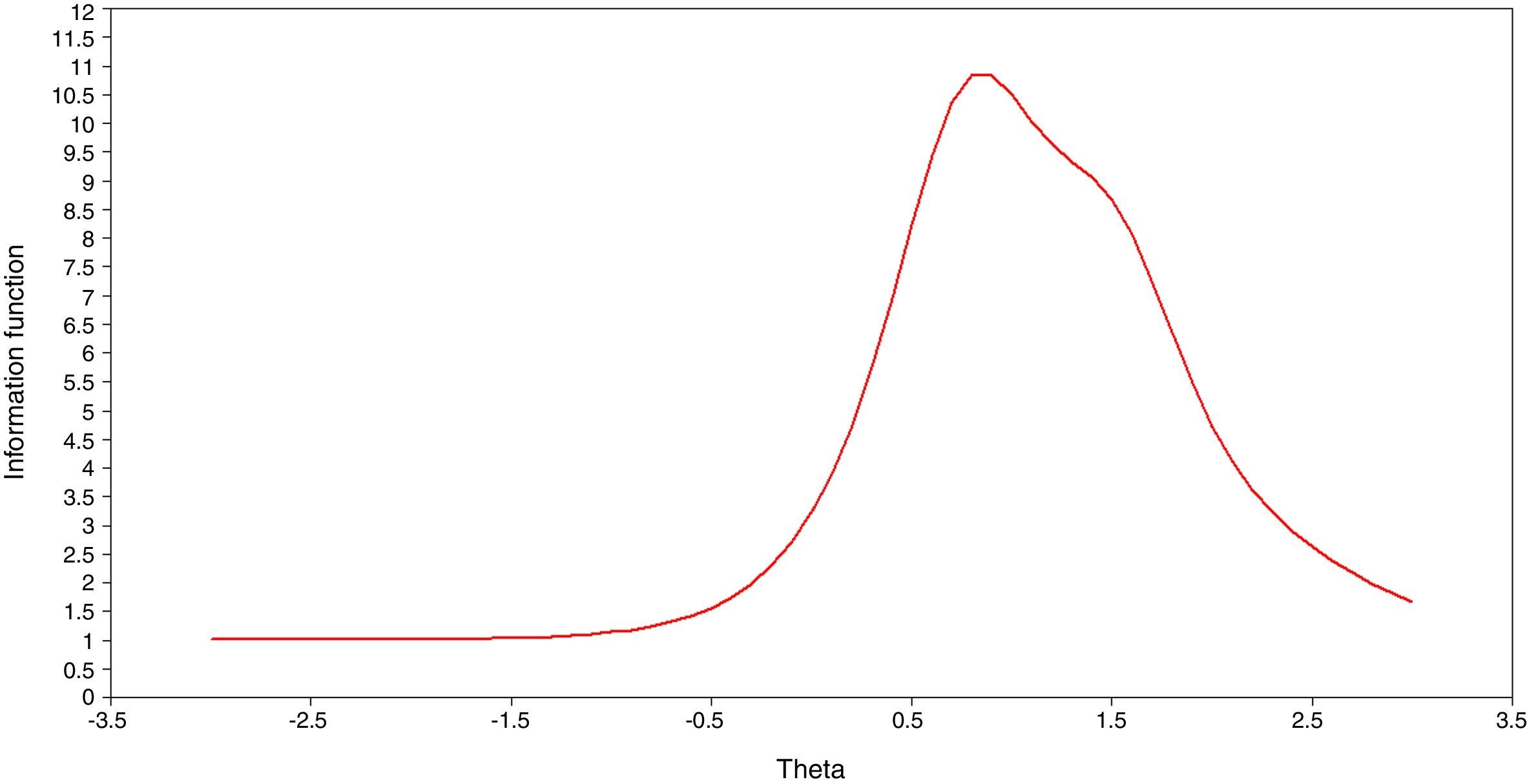
The reliability of the scores was estimated by the ordinal alpha that permits appropriate estimation of the measurement error when the scores are ordinal or dichotomic.46 As an indicator of the precision of the measuring instrument the information function was also calculated using the Item Response Theory.47 The information function makes it possible to analyse the precision with which the construct is measured depending on the position (score) of the person in the latent variable.
Thirdly, those participants who responded affirmatively to at least one item in the PSS were selected (items 3–5). Those who had not answered affirmatively to any of these 3 items were selected as a group for comparison. A MANCOVA was performed where the groups of suicidal ideation and the comparison group were considered to be fixed factors. The total score of difficulties in the SDQ, item 1 and the total score of the PWI-SC were considered to be dependent variables. Sex and age were covariables.
Data analysis took place using the SPSS v2248 statistics programme, FACTOR 10.5.0149 and Mplus 7.4.44
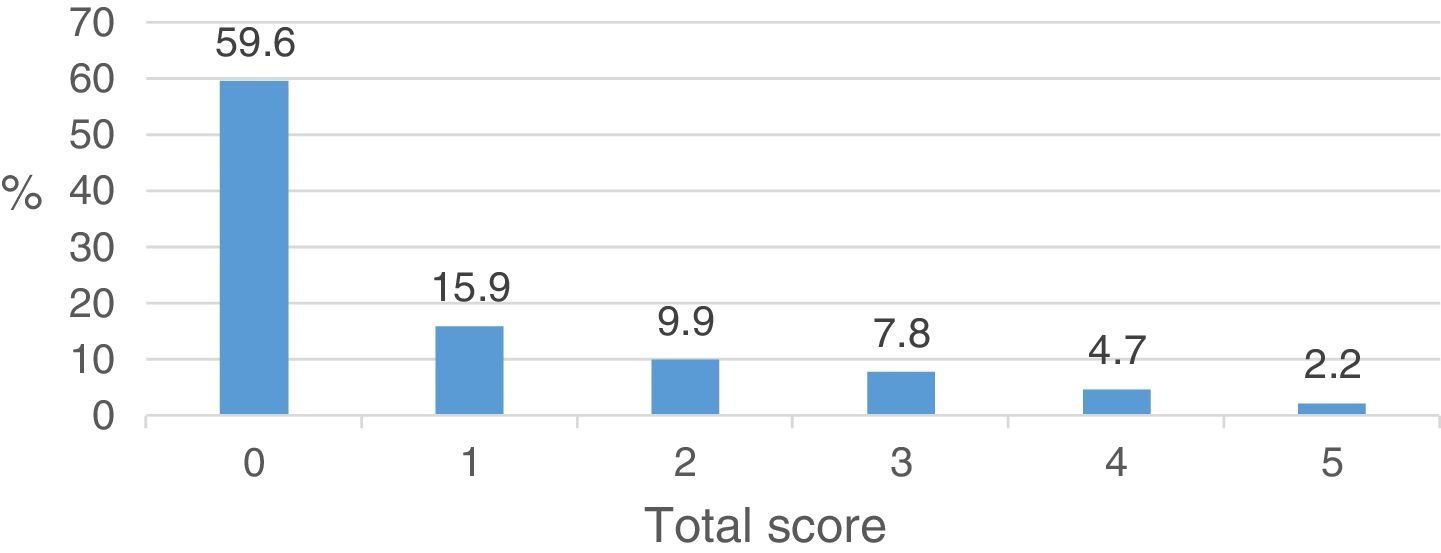
ResultsThe prevalence of suicidal ideation and its expression depending on sex and ageTable 2 shows the percentage of participants who answered affirmatively to the items of the PSS, for the total sample as well as according to sex. Approximately 4% of the sample indicated that they had attempted suicide in the past year. The percentage of participants in the total score of the PSS was also examined. As may be seen in Fig. 1, 2.2% of the sample obtained a score of 5, while 4.7% of the sample answered affirmatively to at least 4 items. Thus from 2.2% to 6.9% of the sample scored 4 or more.

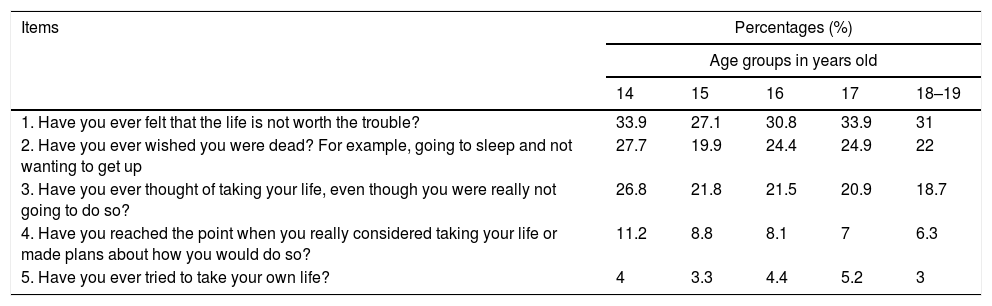
The results showed statistically significant differences depending on sex in items 1 (χ2(1)=17.901; P<.01), 2 (χ2(1)=26.711; P<.01), 3 (χ2(1)=11.659; P<.01) and 4 (χ2(1)=5.011; P=.025) and in the total score (Mmen=0.72 [DT=1.22]; Mwomen=1.04 [DT=1.40]; t(1662)=−4.937; P<.001, d=.228). No differences were found in item 5 (suicidal intention) (χ2(1)=2.979; P=.084). In all of the cases the women had a higher proportion of affirmative replies than the men. The expression of suicidal ideation was also examined, to see whether it varied depending on age. The results are shown in Table 3. No statistically significant differences were found in the 5 items or in the total score of the PSS (P>.05) depending on age group.
The percentage of students who answered affirmatively to items in the Paykel Suicidal Ideation Scale according to age.
| Items | Percentages (%) | ||||
|---|---|---|---|---|---|
| Age groups in years old | |||||
| 14 | 15 | 16 | 17 | 18–19 | |
| 1. Have you ever felt that the life is not worth the trouble? | 33.9 | 27.1 | 30.8 | 33.9 | 31 |
| 2. Have you ever wished you were dead? For example, going to sleep and not wanting to get up | 27.7 | 19.9 | 24.4 | 24.9 | 22 |
| 3. Have you ever thought of taking your life, even though you were really not going to do so? | 26.8 | 21.8 | 21.5 | 20.9 | 18.7 |
| 4. Have you reached the point when you really considered taking your life or made plans about how you would do so? | 11.2 | 8.8 | 8.1 | 7 | 6.3 |
| 5. Have you ever tried to take your own life? | 4 | 3.3 | 4.4 | 5.2 | 3 |
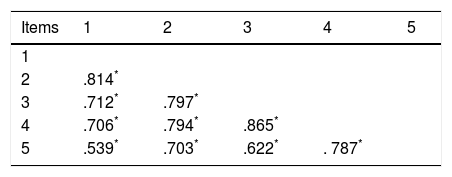
Before analysing the internal structure of PSS scores, the degree of association between the items in the PSS was studied. The matrix of correlations between the items is shown in Table 4. As can be seen, the 5 items are strongly associated, and all of the correlations are statistically significant (P<.01).
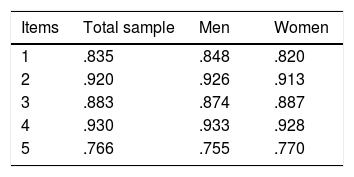
The one-dimensional model that considered the presence of a single general dimension of suicidal ideation had suitable goodness of fit indexes (χ2=45.91; df=5; CFI=.993; TLI=.985; RMSEA=.070 (CI 95%=.057–.089); WRMR=1.326). The standardised factorial weightings are shown in Table 5.
The hypothesis of measurement invariance depending on sex was then subjected to testing. The resulting goodness of fit indexes for men (χ2=24.27; df=5; CFI=.991; TLI=.982; RMSEA=.070 [CI 95%=.044–.089]; WRMR=.888) and for women (χ2=24.001; df=5; CFI=0.994; TLI=.988; RMSEA=.066 [CI 95%=.041–0.093]; WRMR=1.020) were excellent. The standardised factorial weightings for men and women are shown in Table 5.
These results indicated that the data fit the model in both groups, so that it is possible to undertake analysis of factorial equivalence. The model of configural measurement invariance (first step) showed suitable goodness of fit indexes (χ2=47.87; df=10; CFI=.993; TLI=.986; RMSEA=.067 [CI 95%=.049–.087]; WRMR=1.322). This model is considered to be the basal model against which the supposition of a strong measurement invariance (second step, more restrictive) is compared. Likewise, the goodness of fit indexes of the strong measurement invariance model and the restriction of equality of the thresholds between both groups were also appropriate (χ2=46.73; df=13; CFI=.994; TLI=.990; RMSEA=.056 [CI 95%=.039–.074]; WRMR=1.377). The ΔCFI, which was lower than .01, and the Δχ2, which was not statistically significant (χ2(3)=1.639; P=.650), led to acceptance of the strong measurement invariance hypothesis, that is, the factorial equivalence of the PSS scores for men and women, and therefore the absence of differential functioning of the PSS items depending on sex.
Estimation of the reliability of the PSS scores using the ordinal alpha was .93. Fig. 2 shows the information function for the total PSS score. As may be seen, the measuring instrument evaluates medium to high values of the latent variable (θ) with greater precision, while it evaluates lower values with far less precision (θ≤0).
The relationship between the risk of suicidal ideation, emotional and behavioural problems and emotional wellbeing
23.2% (n=386) of the sample answered at least one item in the PSS affirmatively (items 3–5) which asked about suicidal ideation or previous attempted suicide.
The MANCOVA revealed the existence of statistically significant differences when all of the variables were taken together (Wilks’ λ=.791, F(3, 1658)=146.069, P<.001, η2partial=.209). The ANOVA showed statistically significant differences between the groups for suicidal ideation and for comparison with the Total score for problems of the SDQ (Mrisk=15.11(5.25); Mno-risk=10.28(4.71); F(1, 1664)=284.58, P<.001, η2partial=.146) and for item 1 (Mrisk=7.83(1.65); Mno-risk=6.06(2.05); F(1, 1664)=300.49, P<.001, η2partial=.153) and the total score of the PWI-SC (Mrisk=56.80(7.73); Mno-risk=49.50(20.32); F(1, 1664)=221.04, P<.001, η2partial=0.118). The sizes of the effect were moderate. The participants in the group of suicidal ideation and previous attempted suicide reported, on average, more emotional and behavioural problems and lower levels of emotional wellbeing and satisfaction with life than was the case in the comparison group.
DiscussionThe main aim of this work was to analyse suicidal ideation in a representative sample of Spanish adolescents. To this end the prevalence of suicidal ideation was studied together with its expression depending on sex and age. The psychometric properties of the PSS16 were analysed, and the socio-economic adjustment of the participants who reported suicidal ideation and/or previous attempted suicide was examined.
Firstly, the results obtained show that approximately 4% of these adolescents had attempted suicide at some time in their lives. Even more, 6.9% of these young people reported a level of suicidal ideation that could be considered high (with a score of 4 points or more). Additionally, the first item in the PSS, which refers to passive ideas of death, was highly prevalent among the adolescents studied. The rates of prevalence found in this research, with some differences, are similar to those found in previous studies of adolescents.10–15 For example, in a multicentre study of European adolescents using the PSS,16 the prevalence of suicidal ideation was found to stand at 32.3%, while the prevalence of attempted suicide stood at 4.2%.10 Using the same measuring instrument in Spain, rate of suicidal ideation prevalence were found to stand at 7.5% while the corresponding figure for attempted suicide was 3%.11 In previous reviews similar results were found for suicidal behaviours as well as self-harm in samples of adolescents.12 It should be pointed out that depending on the type of behaviour researched, the type of sample or the instrument used, prevalences and their expression according to different sociodemographic correlates (such as sex, age, culture, etc.) may vary considerably. Moreover, if the difficulties inherent in defining behaviours of this type and recording them by competent authorities are taken into consideration, these aspects clearly influence the rates of prevalence found. In general terms, many of the suicidal behaviours reported by the general adult and adolescent populations who are not in care are hidden, and only the “tip of the iceberg” reaches the health system, so that there may be clear underestimation of this phenomenon.
Secondly, the women had a higher rate of suicidal ideation but not of previous attempts in comparison with the men. Suicidal ideation does not vary depending on the age of the adolescents. Regarding sex, previous studies of adolescent10,11 and adult8 populations find totally similar results. For example, Carli et al.10 found that women have a higher rate of suicidal ideation as well as previous attempts than men. Bousoño et al.,11 in a representative sample of Asturian adolescents, found that the women reported more previous attempted suicides but not a higher prevalence of suicidal ideation than the men. Whatever the cause, all forms of suicidal behaviour seem to show different patterns depending on sex.17 Even more, it seems that during adolescence women are in a situation of greater risk of suicidal behaviour than men in comparison with other life stages. These results agree with those of previous studies which show that women report greater internalising difficulties32,50,51 that are associated with emotional problems. This aspect would partially explain the reason why for the differences found in suicidal ideation, logically together with other biological, psychological and social variables.52,53 In connection with age, although no differences were found in this study, previous works in adolescent populations found that the rates of suicidal ideation as well as attempts seem to vary according to age, and that they are higher in older adolescents.10 In the adult Spanish population previous studies have shown that suicidal ideas or plans fall with increasing age.8
Thirdly, the PSS seems to show appropriate psychometric properties in the representative sample used in this research. The results show that the one-dimensional model had an excellent fit with the data. Moreover, this general factor was proven not to vary depending on sex, showing that the items in the PSS do not function differentially, thereby guaranteeing equivalence in the measurement process.54 Its estimated reliability was better than 0.90. Additionally, based on the item Response Theory paradigm, the PSS measured those participants who had higher scores for latent risk (suicidal ideation) with greater precision (less measurement error). From this result it is deduced that the PSS is a more precise tool for measuring participants who have high scores in the latent variable. Although no previous studies that analyse the psychometric quality of the PSS in Spain are yet available, the results seem to indicate that it is a short and suitable instrument for evaluating phenomena of this type in the Spanish adolescent population. New studies should replicate these findings in other samples of interest and analyse their predictive capacity. However it is undertaken, reliable and valid evaluation of suicidal ideation is highly relevant as by detecting and recognising persons at risk, the preventive approach can be improved while implementing specific prophylactic interventions. These results are added to other tools at clinicians’ and researchers’ disposal for the evaluation of these phenomena and their associated constructs.19–22
Fourthly, the results showed that in comparison with the contrast group those adolescents who reported suicidal ideation and/or attempts also expressed less emotional wellbeing and satisfaction with life (an indirect quality of life indicator), as well as more emotional and behavioural problems. These results agree completely with those of previous studies. Thus a broad range of works consistently demonstrate that those adolescents who have suicidal behaviour or intentions report, among other things, a higher number of emotional and behavioural problems, heavier substances consumption, worse quality of life, worse levels of perceived social support, less self-esteem and more behaviour involving risk and impulsiveness.10–12,52,55 All of these factors are also possible risk markers. This group is highly vulnerable, not only in terms of the risk of future suicidal acts but also in terms of a broad range of mental health problems, so that they may require the intervention of a psychologist and/or teacher.
This work is not free of limitations, and some of them are described below. Firstly, suicidal ideation was evaluated using a self-reporting instrument, with the corresponding limitations of tools of this type. Secondly, the PSS is a short scale composed of 5 items, so that the information gathered is limited solely to thoughts of death, suicidal ideation and previous suicide attempts. Thirdly, the sample is composed of inhabitants of a Spanish Autonomous community (La Rioja). Although random stratified sampling by groups was performed, this partially limits the generalisation of the results to the whole Spanish territory. Fourthly, this is a transversal study, so that it is impossible to establish cause–effect relationships.
In spite of these limitations, this study rigorously analyses a social and health problems with major repercussions that affect families and society as well as individuals. The prevention and detection of this problem is highly important.56 A proof of this is the emergence of numerous reports, guides, programmes and recommendation that have included the prevention of suicidal behaviour within the areas of priority action for good mental health and the promotion of emotional wellbeing. Examples of these include the European Pact for Mental Health and Well-being57 or the report by the WHO on the prevention of suicide as a global imperative.3 Future studies may carry out longitudinal follow-ups and gather information from multiple levels of analysis (such as genetic, physiological, cerebral and cultural data, etc.) as well as its connections with other psychological risk factor (such as bullying, substance abuse, Internet use and psychotic experiences, etc.).58–61 In the same way, it is extremely interesting to implement new information technologies (such as smartphones and apps) as well as new psychometric models in the study of suicide.62 The last two decades have seen a growth of interest in the study of the mental health and emotional wellbeing of children and adolescents, although the work in this field is still insufficient. It is clear that many questions remain to be worked on and resolved.
Ethical responsibilitiesProtection of human and animal subjectsThe authors declare that the procedures followed comply with the ethical norms of the applicable human experimentation committee and the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they followed the protocols of their centre of work regarding the publication of patient data.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referred to in this paper. This document is held by the corresponding author.
FundingThis research was financed by the Spanish Ministry of Science and Innovation (MICINN), by the Carlos III Institute, the Mental Health Centre for Networked Biomedical Research (CIBERSAM) and by the 2015 Round of Grants by the BBVA Foundation for Researchers and Cultural Creative Workers. Project references: PSI2011-28638, PSI 2011-23818 and PSI2014-56114-P.
Conflict of interestsThe authors have no conflict of interests to declare.
Please cite this article as: Fonseca-Pedrero E, Inchausti F, Pérez-Gutiérrez L, Aritio Solana R, Ortuño-Sierra J, Sánchez-García MÁ, et al. Ideación suicida en una muestra representativa de adolescentes españoles. Rev Psiquiatr Salud Ment (Barc). 2018;11:76–85.