




Only a few scales have been validated in Spanish for the assessment of suicide risk, and none of them have achieved predictive validity.
ObjectiveTo determine the validity and reliability of the Beck Hopelessness Scale in patients with suicide risk attending the specialist clinic.
MethodsThe Beck Hopelessness Scale, reasons for living inventory, and the suicide behaviour questionnaire were applied in patients with suicide risk attending the psychiatric clinic and the emergency department. A new assessment was made 30 days later to determine the predictive validity of suicide or suicide attempt.
ResultsThe evaluation included a total of 244 patients, with a mean age of 30.7±13.2 years, and the majority were women. The internal consistency was .9 (Kuder–Richardson formula 20). Four dimensions were found which accounted for 50% of the variance. It was positively correlated with the suicidal behaviour questionnaire (Spearman .48, P<.001), number of suicide attempts (Spearman .25, P<.001), severity of suicide risk (Spearman .23, P<.001). The correlation with the reasons for living inventory was negative (Spearman −.52, P<.001). With a cut-off ≥12, the negative predictive value was 98.4% (95% CI: 94.2–99.8), and the positive predictive value was 14.8% (95% CI: 6.6–27.1).
ConclusionThe Beck Hopelessness Scale in Colombian patients with suicidality shows results similar to the original version, with adequate reliability and moderate concurrent and predictive validity.
Pocas escalas se han validado en castellano para el riesgo suicida y en ninguna de ellas se ha hallado la validez predictiva.
ObjetivoDeterminar la validez y confiabilidad de la Escala de Desesperanza de Beck en pacientes con suicidabilidad que acuden a consulta especializada.
MétodosSe aplicaron la Escala de Desesperanza de Beck, el Inventario de Razones para Vivir y el Cuestionario de Comportamiento Suicida a pacientes con suicidabilidad que asistieron a consulta externa y urgencias. A los 30 días se realizó una valoración para determinar la validez predictiva del intento suicida o suicidio.
ResultadosSe evaluaron 244 pacientes con una edad promedio de 30,7 años±13,2; la mayoría de ellos fueron mujeres. La consistencia interna de la Escala de Desesperanza de Beck es de 0,9 (fórmula 20 de Kuder-Richardson). Se encontraron 4 dimensiones que explican el 50% de la varianza. Tuvo una correlación positiva con el Cuestionario de Comportamiento Suicida (Spearman 0,48, p<0,001), número de intentos suicidas (Spearman 0,25, p<0,001), y severidad del riesgo suicida (Spearman 0,23, p<0,001). La correlación con el Inventario de Razones para Vivir fue negativa (Spearman −0,52, p<0,001). Con un punto de corte ≥12 el valor predictivo negativo fue de 98,4% (IC 95%: 94,2-99,8), y el valor predictivo positivo fue de 14,8% (IC 95%: 6,6-27,1).
ConclusiónLa Escala de Desesperanza de Beck en pacientes colombianos con suicidabilidad presenta unas dimensiones similares a la versión original, con adecuada confiabilidad y moderada validez, tanto concurrente como predictiva.
In the sixty-sixth World Health Assembly in 2013 the WHO Mental Health Action Plan was adopted. Suicide prevention is an integral part of the said plan, with the aim of reducing the suicide rate by around 10% in all countries by the year 2020.1 The annual standardised age suicide rate was 11.4 per 100,000 inhabitants (15 for men and 8 for women). Nevertheless, this figure is considered to be an under-estimate as suicide is a sensitive subject. It is even illegal in several countries, so that it is not reported; additionally, in countries where it is properly reported it is often poorly classified as accidental death or other causes of death.2 For every suicide there are many people who attempt suicide every year. Attempting suicide is the most important risk factor for suicide in the general population.
In Colombia in 2014 the medical system reported a mortality rate due to suicide of 4.33 cases per 100,000 inhabitants, which is similar to the reported rates for the last 9 years. The highest rate per 100,000 inhabitants (6.5) is reported for the 20 to 24 year old and 70 to 74 year old age groups.3
Suicide is a public health problem that can be prevented by low-cost evidence-based interventions.2 It is therefore important to implement tools for the early detection of patients at risk of suicide.
These tools have to evaluate risk factors. A great many risk factors have been described in the literature, and they include hopelessness.2
Self-administered scales and instruments have been shown to be a good alternative for this evaluation in emergency and out-patient departments, as they are easy and fast to apply.4,5 To use these tools it is necessary to validate them in each community so that healthcare personnel have useful instruments that allow them to be more efficient when treating patients of this type.
Although several scales are used, the oldest and one of those to have been evaluated for predictive validity is the Beck Hopelessness Scale (BHS).5 Hopelessness is defined as pessimism or negative expectations about the future, and it is associated with suicide.6 More specifically, hopelessness has been associated with suicidal ideation, a previous attempted suicide and suicidal behaviour in the adolescent community and mental health patients; it is also associated with past and future attempted suicide.7,8 The main aim of the scale is to measure hopelessness, although several studies showed that it is a good predictor of attempted and consummated suicides.9,10
This scale was selected because it was the first to be designed exclusively to evaluate hopelessness, and this has been correlated with a higher risk of suicide.
The aim of this research is to determine the validity and reliability of the BHS in patients at risk of suicide who attend a specialised surgery in the city of Bucaramanga, Colombia.
MethodsA diagnostic test was subjected to a validation study. The study was approved by the Research Ethics Committee of the Health Sciences Faculty of Bucaramanga Universidad Autónoma. All of the participants were asked to give their informed consent before commencing the study. They gave their consent after receiving an explanation and understanding the research objectives. They took part voluntarily and with the guarantee of confidentiality according to the Colombian regulations governing health research and the Helsinki Declaration.11,12 In the case of minors the adolescent and a family member or tutor both had to give their consent.
InstrumentsThe BHS was prepared by Aaron T. Beck et al. in the Cognitive Therapy Centre of the Psychiatric Department in Pennsylvania University Faculty of Medicine, to evaluate pessimism in patients at risk of suicide.6 Beck and his co-workers constructed an instrument based on pessimistic statements about the future selected from the descriptions mentioned by patients. The 20 propositions selected were known as the General Expectations Scale (GES).6 In 1974 some words in certain propositions were changed, and the definitive current version of the BHS was presented. The scale is composed of 20 propositions that can be defined as true or false, and they evaluate the scope of negative expectations about the immediate and long-term future.6 The replies are added to give a score of from 0 to 20, with a cut-off point at 9 or 10, depending on the population for which it was validated. The items that indicate hopelessness score 1 point, while those that do not indicate it score 0 points. The number of points measure the severity of hopelessness: 0–3 is minimum or normal, 4–8 is mild, 9–14 is moderate and 15–20 is severe.5 The BHS was validated with a good internal consistency that varies from .82 to .93; its test-retest reliability varies from .60 to .69; its convergent validity with the Beck Depression Inventory (BD) is 0.63. The BHS discriminates for patients with depression (M=11.3; SD=5.2) and generalised anxiety (M=7.9; SD=4.9).6,9,13,14 The main purpose of the scale is to measure hopelessness, although several studies show that it is a good predictor of attempted and consummated suicide.10,15
The Suicide Behaviour Questionnaire—Revised (SBQ-R) is an instrument composed of 4 items. It contains questions on suicidal thoughts and behaviour in the past and future. The SBQ-R is a Likert-type questionnaire, and it consists of questions about the frequency of the emergence of suicidal ideation, the communication of suicidal thoughts to others, attitudes and expectations regarding the current suicide attempt. The maximum score is 18, and the scale takes approximately 5min to complete. It has suitable internal consistency, test-retest reliability and concurrent validity.16
The Reasons for Living Inventory (RFL) is a questionnaire that contains 48 items that score on a Likert-type 6 point scale. This scale evaluates the adaptive (positive) beliefs and expectations for not committing suicide. The factors analysed are divided into dimensions and indicate the 6 main reasons for living: a) beliefs about survival and facing up to things (24 items); b) family responsibility (7 items); c) concerns in connection with children (3 items); d) fear of suicide (7 items); e) fear of social disapproval (3 items), and f) moral objections (4 items).17
Population studied and sampleThe study universe was composed of all the patients who visited either the emergency department or the outpatient surgery of the Instituto del Sistema Nervioso de Oriente (ISNOR) with suicidal tendencies. To ensure that the sample was collected, the psychiatrist marked a predetermined box in the electronic clinical history once a patient with suicidal tendencies had been detected. This sign informed the group of researchers of the presence of a patient with suicidal tendencies so that they could be included in the study.
To calculate the size of the sample the sum of the 20 items in the BHS was used. The recommendation to recruit 10 patients per item was taken into account, to make it possible to validate the construct (in this case, at least 200 patients).18 For the predictive validation an incidence of 10% of attempted or consummated suicides was taken into account, with a negative predictive value of .95 and a positive predictive value of .2; a level of significance of .05 and a power of .8 for a minimum number of 480 patients. Patients with suicidal tendencies were defined as all of those with suicidal thoughts, ideas or plans and behaviour or attempted suicides.19
ProcedureAll of the patients who voluntarily agreed to participate in the study and who had suicidal tendencies according to their doctor were included in the study. Those with psychosis were excluded, as were those with cognitive functioning that would prevent them from answering the interview or those who were incapable of understanding the questions of the scale due to their educational level.
All of the patients were interviewed by one of the researchers with previous training in evaluation of the risk of suicide. The training was carried out by the director of the group of researchers, a psychiatrist with 14 years’ experience and 3 years in research into the risk of suicide. They conducted a semi-structured interview that asked about demographic characteristics, the main risk factors such as alcohol consumption, family problems or problems with their partner, as well as protective factors such as having children and being older.20 They finally classified the severity of the risk of suicide as low, medium, high or very high and immediate, depending on the presence or absence of factors.
After the interview one of the researchers gave the patient instructions about how to answer the BHS, the RFL and the SBQ-R.
A researcher interviewed the patient 30 days later to establish whether there had been an attempted or consummated suicide, and the BHS was applied again. The reason why a 30 day follow-up was selected is that it is in the first 2 weeks that the highest number of attempts or suicides is observed in patients with suicidal tendencies.21,22 Although of course it is possible for them to make further attempts or suicide after 30 days, the probability of this is far lower. A maximum of 3 appointments were made for this follow-up, and if the patient did not keep the appointment they were declared to have abandoned the study.
Statistical analysisBased on the fact that the BHS is a dichotomic scale, internal consistency was determined using the Kuder–Richardson 20 coefficient.23 Before identifying possible factors on the scale Bartletts’ sphericity test was applied together with the Kaiser–Meyer–Olkin (KMO) sample suitability index.24,25 To test construct validity an oblique exploratory factor analysis was performed (Promax).26 For predictive validation the positive and negative predictive values were found, defining the best cut-off point according to the ROC curve.27 For converging validity Spearman's or Pearson's correlation coefficient was used, depending on the case.
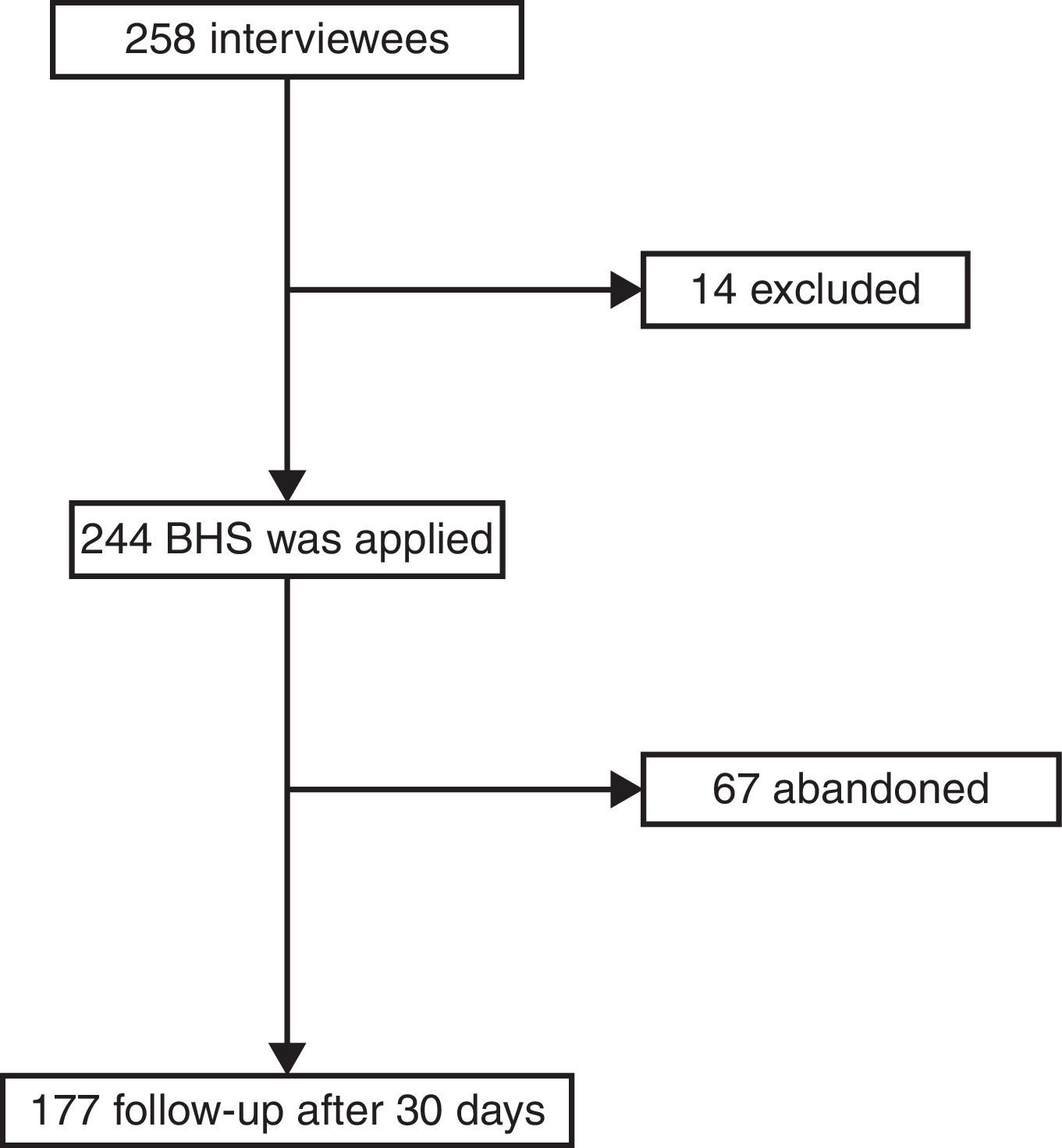
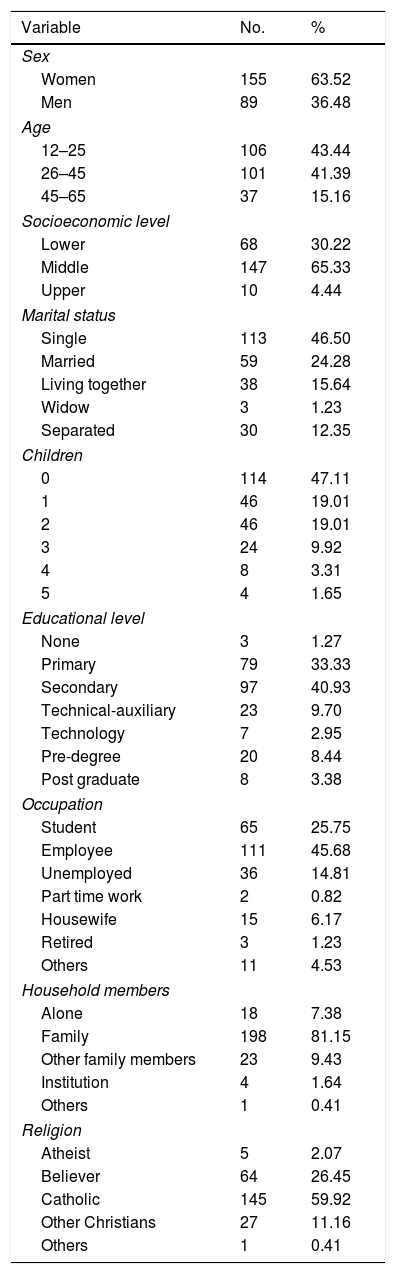
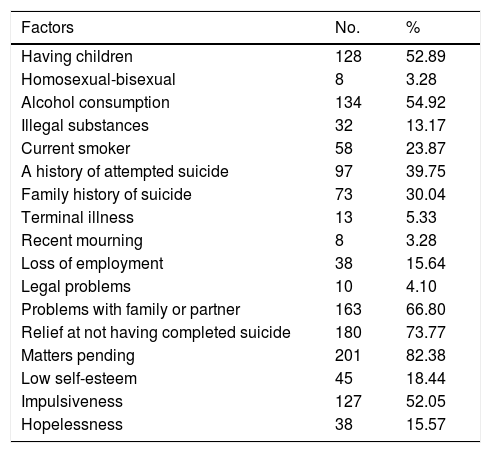
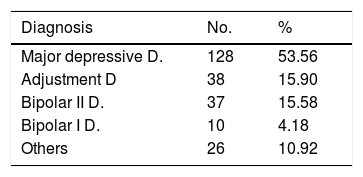
Results258 patients were interviewed, of whom 14 were excluded from the study as they fulfilled exclusion criteria; 244 agreed to take part in the study voluntarily; 67 patients did not conclude the study as it was not possible to contact them. Fig. 1 shows the pattern of the study. The majority of the patients were women, which can be expected as they are the population which consult the most; the average age was 30.65 years old±13.2, with an educational level ending at 11 years old±3.4 years. Table 1 shows the sociodemographic characteristics of the population. Table 2 shows the suicide protective or risk factors which were clinically evaluated using the semi-structured interview. Table 3 shows the main diagnoses of the population studied. No consummated suicides occurred and there were 10 attempted suicides in the 30 day follow-up.

Sociodemographic variables of the patients with suicidal tendencies.
| Variable | No. | % |
|---|---|---|
| Sex | ||
| Women | 155 | 63.52 |
| Men | 89 | 36.48 |
| Age | ||
| 12–25 | 106 | 43.44 |
| 26–45 | 101 | 41.39 |
| 45–65 | 37 | 15.16 |
| Socioeconomic level | ||
| Lower | 68 | 30.22 |
| Middle | 147 | 65.33 |
| Upper | 10 | 4.44 |
| Marital status | ||
| Single | 113 | 46.50 |
| Married | 59 | 24.28 |
| Living together | 38 | 15.64 |
| Widow | 3 | 1.23 |
| Separated | 30 | 12.35 |
| Children | ||
| 0 | 114 | 47.11 |
| 1 | 46 | 19.01 |
| 2 | 46 | 19.01 |
| 3 | 24 | 9.92 |
| 4 | 8 | 3.31 |
| 5 | 4 | 1.65 |
| Educational level | ||
| None | 3 | 1.27 |
| Primary | 79 | 33.33 |
| Secondary | 97 | 40.93 |
| Technical-auxiliary | 23 | 9.70 |
| Technology | 7 | 2.95 |
| Pre-degree | 20 | 8.44 |
| Post graduate | 8 | 3.38 |
| Occupation | ||
| Student | 65 | 25.75 |
| Employee | 111 | 45.68 |
| Unemployed | 36 | 14.81 |
| Part time work | 2 | 0.82 |
| Housewife | 15 | 6.17 |
| Retired | 3 | 1.23 |
| Others | 11 | 4.53 |
| Household members | ||
| Alone | 18 | 7.38 |
| Family | 198 | 81.15 |
| Other family members | 23 | 9.43 |
| Institution | 4 | 1.64 |
| Others | 1 | 0.41 |
| Religion | ||
| Atheist | 5 | 2.07 |
| Believer | 64 | 26.45 |
| Catholic | 145 | 59.92 |
| Other Christians | 27 | 11.16 |
| Others | 1 | 0.41 |
Risk and protective factors for patients with suicidal tendencies.
| Factors | No. | % |
|---|---|---|
| Having children | 128 | 52.89 |
| Homosexual-bisexual | 8 | 3.28 |
| Alcohol consumption | 134 | 54.92 |
| Illegal substances | 32 | 13.17 |
| Current smoker | 58 | 23.87 |
| A history of attempted suicide | 97 | 39.75 |
| Family history of suicide | 73 | 30.04 |
| Terminal illness | 13 | 5.33 |
| Recent mourning | 8 | 3.28 |
| Loss of employment | 38 | 15.64 |
| Legal problems | 10 | 4.10 |
| Problems with family or partner | 163 | 66.80 |
| Relief at not having completed suicide | 180 | 73.77 |
| Matters pending | 201 | 82.38 |
| Low self-esteem | 45 | 18.44 |
| Impulsiveness | 127 | 52.05 |
| Hopelessness | 38 | 15.57 |
The average score on the BHS was 7.8±5.3. The minimum score was 0 and the maximum score was 20. The total average for the women was 7.9±5, and for the men it was 7.8±5.8.
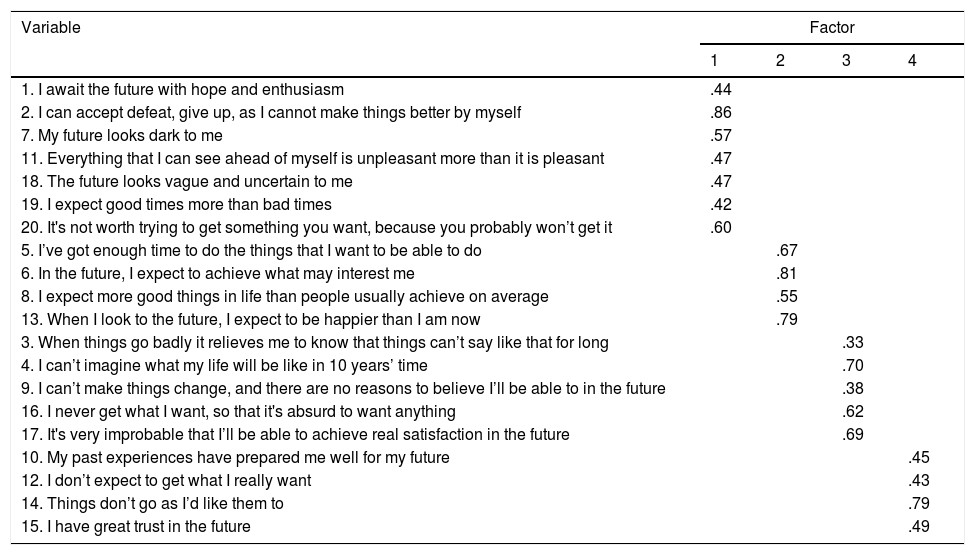
Analysis of factors. Bartlett's sphericity test was significant (χ2=1419.01, gl=190, P<.001). The KMO sample suitability test showed it to be suitable (0.90). Oblique exploratory factor analysis (Promax) found 4 dimensions that explained 50% of the variance. These dimensions were denominated: (1) expectations for the future (self-evaluated 6.34; explaining 31.7% of the variance); (2) motivation (self-evaluated 1.54; explaining 7.7% of the variance); (3) pessimism about the future (self-evaluated 1.19; explaining 6.0% of the variance), and (4) individual perception of the future (self-evaluated 1.0; explaining 5.0% of the variance) (Table 4).
Factorial analysis of the BHS.
| Variable | Factor | |||
|---|---|---|---|---|
| 1 | 2 | 3 | 4 | |
| 1. I await the future with hope and enthusiasm | .44 | |||
| 2. I can accept defeat, give up, as I cannot make things better by myself | .86 | |||
| 7. My future looks dark to me | .57 | |||
| 11. Everything that I can see ahead of myself is unpleasant more than it is pleasant | .47 | |||
| 18. The future looks vague and uncertain to me | .47 | |||
| 19. I expect good times more than bad times | .42 | |||
| 20. It's not worth trying to get something you want, because you probably won’t get it | .60 | |||
| 5. I’ve got enough time to do the things that I want to be able to do | .67 | |||
| 6. In the future, I expect to achieve what may interest me | .81 | |||
| 8. I expect more good things in life than people usually achieve on average | .55 | |||
| 13. When I look to the future, I expect to be happier than I am now | .79 | |||
| 3. When things go badly it relieves me to know that things can’t say like that for long | .33 | |||
| 4. I can’t imagine what my life will be like in 10 years’ time | .70 | |||
| 9. I can’t make things change, and there are no reasons to believe I’ll be able to in the future | .38 | |||
| 16. I never get what I want, so that it's absurd to want anything | .62 | |||
| 17. It's very improbable that I’ll be able to achieve real satisfaction in the future | .69 | |||
| 10. My past experiences have prepared me well for my future | .45 | |||
| 12. I don’t expect to get what I really want | .43 | |||
| 14. Things don’t go as I’d like them to | .79 | |||
| 15. I have great trust in the future | .49 | |||
Internal consistency. The Kuder–Richardson 20 coefficient was .88 for the total BHS. The Kuder–Richardson values for each one of the dimensions were as follows: 0.81 for the first factor; .70 for the second factor; .65 for the third el factor and .64 for the fourth factor.
Concurrent validity. A positive correlation was found with the SBQ (Spearman .48, P<.001); number of attempted suicides (Spearman .25, P<.001), and the severity of the risk of suicide classified by the researcher (Spearman .23, P<.001). The correlation with the RFL inventory was negative (Spearman −.52, P<.001).
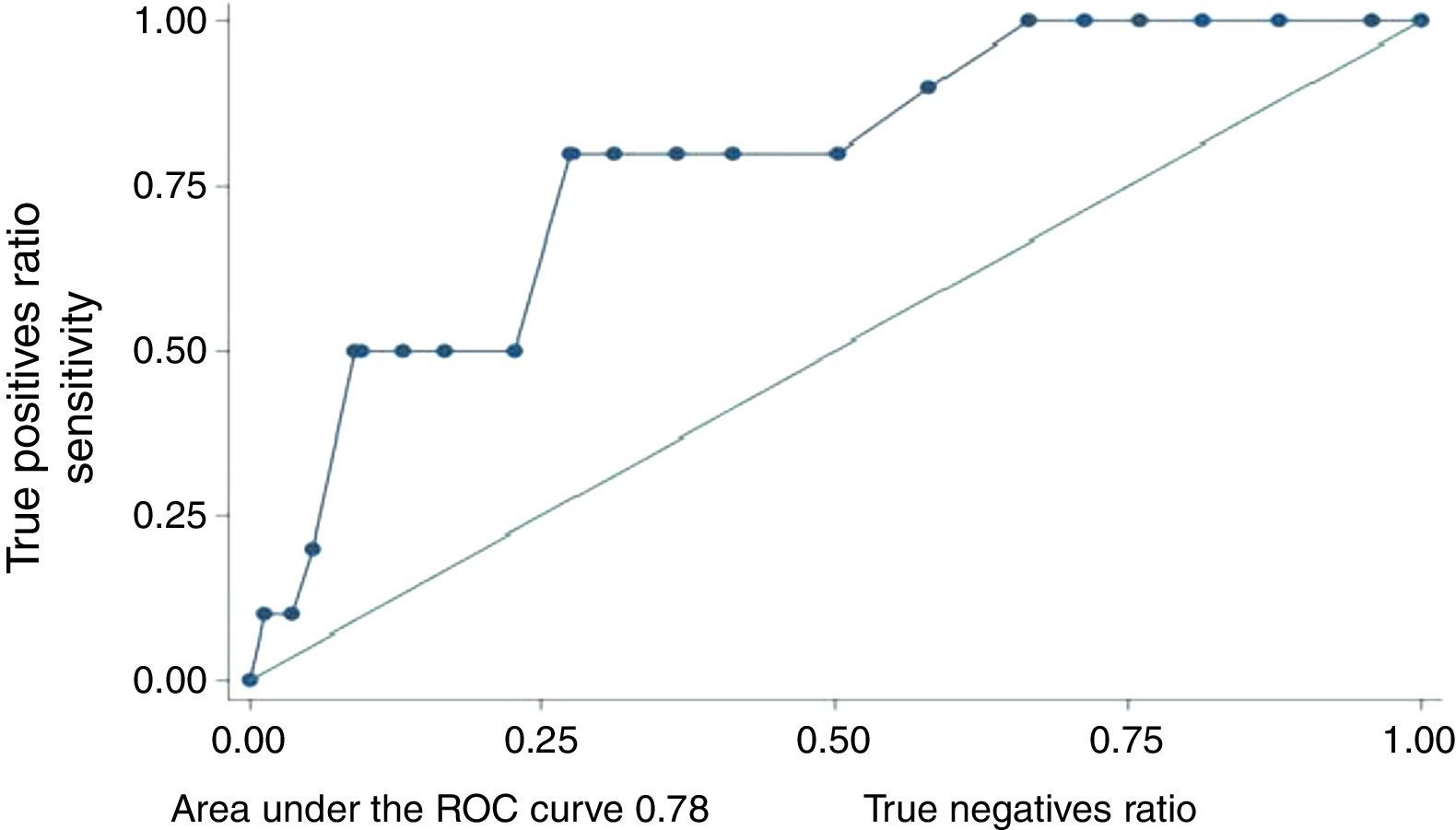
Predictive validity. The area under the ROC curve was 0.78 (CI 95%: 0.64–0.92) (Fig. 2). In this population the best cut-off point was ≥12. With this cut-off point the negative predictive value was 98.4% (CI 95%: 94.2–99.8) and the positive predictive value was 14.8% (CI 95%: 6.6–27.1). The RR of the patients with suicidal tendencies with scores ≥12 was 9.1 (CI 95%: 2–41.5).
Discussion
This study shows that in the Colombian population the BHS has similar dimensions to the original version, with suitable reliability and good concurrent validity. Nevertheless, the utility of the scale may be affected by its low positive predictive value.
Although it is similar to the original, the factorial structure of the BHS in a Colombian population has an additional factor. In the original validation by Beck et al. in 1974 3 factors were found: feelings about the future, loss of motivation and expectations for the future which is similar to a validation in Argentina.10,14 In this validation the feelings about the future factor was divided into pessimism and individual perception of the future. In a subsequent validation by Steer et al. in 199728 2 factors were found: pessimism about the future, which is similar to ours, and resignation, which would correspond to expectations for the future and in this work. Additionally, a validation carried out in 2006 in Lima, Peru, found 6 factors, although 2 of them only contained one item.9 The differences observed may be explained by the type of population in question, given that Beck included the general population and patients at risk of suicide or simply with depression.14,28 On the other hand, the differences in interpreting the questions may be due to cultural factors. These would lead the dimensions to vary with the population, although in any case they would still follow a relevant and representative intrinsic logic in connection with the concept of hopelessness.
In spite of the difference in the construct, the BHS worked correctly in our population given that the total internal consistency of the scale was excellent and each one of the factors had an internal consistency that was from good to very good. This indicates that there are no redundant questions in the scale and that nor are any items lacking in each factor.
As expected, the BHS had a diverging correlation with the RFL, given that the latter is constructed using positive statements about life, children, the family or religion. It is also logical for it to have a converging correlation with the SBQ-R and number of attempted suicides, given that hopelessness has been associated with such behaviour. The correlation with the number of suicide attempts had been determined previously.29 The positive correlation with the SBQ-R had also been documented.30 Nevertheless, this is the first time that the correlation of this scale with the severity of the risk of suicide evaluated by the researcher has been documented.
With respect to predictive validity, a high negative predictive value was found, making the scale useful in departments where swift evaluation by a psychiatrist would be difficult. This is because the scale guarantees with a low margin of error that those who score less than 12 will have a lower probability of attempted suicide. Nevertheless, its positive predictive value was very low, leading to a high percentage of false positives. The result of this characteristic of the scale is that when a score is 12 or more it is impossible to determine whether there is a real high risk of suicide. It is therefore impossible to use the scale alone as the only tool in evaluating the risk of suicide. This has to be evaluated by a psychiatrist or expert in the evaluation of this risk. These predictive values are similar to those found in previous studies, so that the APA recommended that these scales should not be used in clinical practice to estimate the risk of suicide.31 However, the APA probably ruled out the usefulness of the scale in countries where it would be hard to find the necessary specialised human resources, and that it did not take into account that a large number of false positives are inevitable for rare phenomena such as suicide.
Beck et al. performed a study in which they observed the relationship between hopelessness and suicide, analysing the outcome of each patient for death due to suicide. They took a sample of 1958 patients with affective disorders and suicidal ideas from September 1978. Each patient had to complete the BHS. The follow-up included those patients who had finished their treatment in the hospital until 1982. To document whether any of the participants committed suicide a 43 month follow-up study was carried out of death certificates registered in the local Philadelphia and national offices; 31 participants died (1.6%), of whom 17 committed suicide (0.86%). They found that the patients who committed suicide had a higher score on the scale than the patients who died from natural causes. They found a cut-off point for the BHS of 9, unlike this study, in which the cut-off point for the BHS was found at 12. The sensitivity was 94.1% and specificity was 41%. Although these values may seem to be good, they represent intrinsic properties of the scale and have no practical value in themselves. The positive predictive value in the study by Beck et al. stood at 2.28%, and the negative predictive value was 96.6%. These data were not shown in the study but can be found based on sensitivity and specificity. When seen in this light the study by Beck et al. has conclusions that are similar to those of this study.32
The chief limitation of this study is that the sample is too small to achieve predictive validity. Nevertheless, the confidence interval for negative predictive value is appropriate. This is one of the few studies to evaluate the predictive validity of the BHS, and it is the first one to do so in a Latin American population. Additionally, although the RR was significant, it has a broad confidence interval for the same reason: an insufficient sample. However, the sample was large enough to find the concurrent and reliability validity of the construct. Another weakness was the follow-up time; although in the first month after detecting the risk of suicide a higher proportion of suicides or attempted suicides was expected, this is also the time when the highest number of therapeutic alternatives are offered, and it cannot be ruled out that suicide occurred subsequently.
The findings of this study could be used by clinicians without sufficient training to evaluate patients at risk of suicide in primary care departments and in situations where rapid access to a psychiatrist is hindered by geographical factors or deficiencies in the health system. Taking into account the fact that the BHS is the best-known tool for evaluating hopelessness and that this is one of the most important risk factors in the evaluation of the risk of suicide, this work offers a valid scale for evaluating hopelessness in Latin America. Nevertheless, it is recommendable that these results be repeated in similar populations with a longer follow-up.
Conclusions- 1.
A high level of negative predictive validity was found, making this scale useful in outpatient and emergency departments, given that there is a high probability that patients who score less than 12 will not attempt suicide in the next 30 days.
- 2.
The finding of a low positive predictive validity and thus a higher probability of false positives means that expert evaluation is required before taking any measure with the patient. Nevertheless, this does not mean that the scale is not useful as an initial way to evaluate the risk of suicide.
- 3.
In Colombian patients with suicidal tendencies the BHS has similar dimensions to the original version, with a suitable level of reliability and moderate concurrent as well as predictive validity.
The authors declare that no experiments with human beings or animals took place in this research.
Data confidentialityThe authors declare that they followed the protocols of their centre of work on the publication of patient data.
Right to privacy and informed consentThe authors obtained the informed consent of the patients and/or subjects referred to in this paper. This document is held by the corresponding author.
Conflict of interestsThe authors have no conflict of interests to declare.
We would like to thank Dr. María Teresa López, Dr. Kelly Guzmán and Dr. Alexander Blanco for their help in this work.
Please cite this article as: Rueda-Jaimes GE, Castro-Rueda VA, Rangel-Martínez-Villalba AM, Moreno-Quijano C, Martinez-Salazar GA, Camacho PA. Validación de la Escala de Desesperanza de Beck en pacientes con riesgo suicida. Rev Psiquiatr Salud Ment (Barc.). 2018;11:86–93.