







Breast cancer (BC) is a heterogeneous and complex disease characterized by distinct biological subtypes and numerous risk factors. Salivary biomarkers for BC are promising indicators of both oral and systemic health. Given the role of antioxidants in the development and progression of BC, assessing patient's antioxidant capacity through saliva may be a valuable strategy.
Material and methodsThis study aimed to investigate the antioxidant capacity of saliva in 134 women with BC and its correlation with prognostic factors. Total antioxidant capacity (TRAP) was measured using the high-sensitivity chemiluminescence technique.
ResultsSignificantly reduced salivary TRAP levels were observed in women with tumors positive for estrogen and progesterone receptors (p<.05). Conversely, an increase in salivary TRAP levels was noted in patients with triple-negative tumors. No significant changes were observed in other clinical comparisons. Correlation analysis revealed negative associations between reduced salivary TRAP levels and estrogen receptors (R=−0.1881) and progesterone receptors (R=−0.1837). Positive correlations were found between TRAP levels and the ki67 proliferation index above 14% (R=0.1697), as well as the presence of the triple-negative tumor molecular subtype (R=0.2078). Additionally, the analysis showed no correspondence between TRAP levels in saliva and blood, with TRAP levels being higher in blood than in saliva.
ConclusionsThese findings suggest that salivary TRAP levels could serve as a systemic marker associated with BC, particularly in cases with a worse prognosis, such as triple-negative tumors and high proliferation indices.
El cáncer de mama (BC) es una enfermedad heterogénea y compleja que se caracteriza por diferentes subtipos biológicos y numerosos factores de riesgo. Los biomarcadores salivales para el BC son indicadores prometedores de la salud oral y sistémica. Dado el rol de los antioxidantes en el desarrollo y progresión del BC, evaluar la capacidad antioxidante del paciente a través de la saliva puede ser una estrategia valiosa.
Material y métodosEl objetivo de este estudio fue investigar la capacidad antioxidante de la saliva en 134 mujeres con BC, así como su correlación con los factores pronósticos. La capacidad antioxidante total (CAT) se midió mediante la técnica de quimioluminiscencia de alta sensitibilidad.
ResultadosSe observaron niveles salivales considerablemente reducidos de CAT en las mujeres con tumores positivos en términos de receptores de estrógenos y progesterona (p<0,05). Por contra, se detectó un incremento de los niveles salivares de CAT en las pacientes con tumores triple negativos. No se observaron cambios significativos en otras comparaciones clínicas. El análisis de correlación reveló asociaciones negativas entre los niveles reducidos de CAT salival y los receptores de estrógeno (R=−0,1881) y progesterona (R=−0,1837). Se encontraron correlaciones positivas entre los niveles de CAT y el índice de proliferación de ki67 superior al 14% (R=0,1697), así como la presencia del subtipo molecular del tumor triple negativo (R=0,2078). Además, el análisis no reflejó correspondencia entre los niveles salivales y sanguíneos de CAT, siendo mayores estos niveles en sangre que en saliva.
ConclusionesEstos hallazgos sugieren que los niveles salivales de CAT podrían servir como un marcador sistémico asociado al BC, particularmente en casos con peor pronóstico, tales como los tumores triple negativos y los índices altos de proliferación.
Breast cancer (BC) is one of the most pressing public health issues worldwide. This is one of the most frequently diagnosed malignancy among women globally and a leading cause of death.1 By 2070, an estimated 34 million new cases are projected.2 In Brazil, 704 000 new cancer cases are anticipated between 2023 and 2025, with approximately 10% attributed to female BC, making it the second most common malignant tumor in the country.3
BC is a multifaceted disease with significant genetic variability and several molecular subtypes, each presenting distinct clinicopathological characteristics.4,5 Recent decades have seen extensive research into the mechanisms and factors involved in breast carcinogenesis.6 Studies have identified oxidative stress as a key factor in carcinogenesis, contributing to genetic mutations and maintaining genomic instability.7
Oxidative stress arises from an imbalance between the production of reactive species and their neutralization by antioxidant defenses.8 Persistent oxidative damage without adequate antioxidant repair can significantly impact redox homeostasis and the etiology of BC.9 Research has highlighted the clinical significance of systemic antioxidant levels in BC, noting increased tumor antioxidant capacity,10 reduced systemic antioxidant capacity,11 and changes in plasma antioxidant levels following chemotherapy12,13 .
Despite advancements, identifying BC biomarkers faces challenges, primarily due to the difficulty in obtaining samples from small tumor masses and the invasive nature of blood and body fluid collection. In this regard, saliva has emerged as a promising source for cancer biomarker discovery. Sialochemistry, the study of saliva composition, indicates that saliva contains a wide array of biomolecules, including proteins, enzymes, antibodies, and nucleic acids, which are also present in the blood. This overlap suggests that saliva can reflect systemic physiological and pathological conditions, making it a valuable diagnostic fluid.14
The advantage of using saliva lies in its non-invasive collection method, which is simple, stress-free, and can be performed repeatedly without discomfort to the patient. This non-invasive nature makes it particularly suitable for large-scale screenings and monitoring of disease progression and treatment response. Moreover, saliva collection does not require specialized medical personnel or equipment, thus reducing costs and logistical challenges associated with blood sampling. Given these benefits, saliva offers a practical and efficient means for obtaining biochemical data on systemic diseases, providing new possibilities for complementary testing and advancing personalized medicine.15
Given the significance of antioxidants in BC and the lack of studies using saliva for this analysis, our study investigated antioxidant levels in the saliva of women with BC. We evaluated their correlation with clinical aspects that determine disease prognosis.
MethodsStudy designThe present study employs a mixed-methods, retrospective-prospective approach involving qualitative and quantitative analyses of patients treated at the Francisco Beltrão-PR Cancer Hospital (Ceonc) between 2015 and 2022 to investigate lesions suggestive of BC. Ethical approval for this research was granted by the Institutional Ethics Committee.
Inclusion criteria required a confirmed diagnosis of BC via biopsy, specifically the CDI histological type (infiltrating ductal carcinoma), and paired collection of both blood and saliva samples. Exclusion criteria encompassed samples lacking paired blood or saliva, insufficient quantities for processing, and patients currently undergoing chemotherapy. A total of 134 women participated voluntarily, providing signed informed consent forms.
To gather comprehensive clinicopathological data, a questionnaire was administered alongside consultation of medical records:
- 1)
Biopsies were categorized according to their histological grade (graded as 1 for well-differentiated, 2 for moderately differentiated, or 3 for poorly differentiated). These data were grouped as low (grades 1 and 2) and high (grade 3) degrees. Immunohistochemical analyses were conducted on CDI-positive biopsies to assess the expression of estrogen (ERs) and progesterone (PRs) receptors (cut-off value >1%), human epidermal receptor 2 (HER2) amplification (also evaluated by FISH test in 2+ HER2-positive samples), and the ki67 proliferation index status. Samples were classified as Luminal A-like (ER and/or PR positive, ki67<14%, HER2 negative), Luminal B-like (ER and/or PR positive, ki67≥14%, HER2 negative, HER2-amplified (negative ER and PR, any ki67 status, and HER2-amplified), and triple-negative (ER, PR, and HER2 negative, with any ki67 value), based on the St Gallen Consensus.16
- 2)
Determination of the patient's clinical profile was based on clinical data collected during medical consultations and from medical records, focusing on the following parameters:
- a)
Age at diagnosis: Patients were categorized as either under 50 years old or over 50 years old.
- b)
Body mass index (BMI): BMI was categorized into:
- i)
Normal BMI: BMI≤26 kg/m2.
- ii)
Overweight: BMI between 26.1 and 30 kg/m2.
- iii)
Obesity: BMI>30.1 kg/m2.
- i)
- c)
Menopausal status at diagnosis: Patients were classified as either pre-menopausal (presence of menstrual cycles) or post-menopausal (absence of menstrual cycles).
- a)
These variables provide essential clinical context for understanding the demographic and physiological characteristics of the patients studied, aiding in the comprehensive analysis of BC outcomes and treatment responses.
Sample obtentionPeripheral heparinized blood samples, averaging 10 mL per patient, were collected preoperatively and processed by centrifugation at 4000 rpm for 5 min to separate the plasma. Saliva samples were obtained in individual plastic tubes through spontaneous salivation without stimulation. All participants underwent a minimum 8-h fast prior to sample collection. The samples were collected concurrently and stored in a freezer at −20 °C until analysis.
Assessment of total antioxidant capacity by high sensitivity chemiluminescence (TRAP)The compound 2,2′-azobis (ABAP) reacts with lipids present in the sample to generate lipoperoxides, a process that emits low levels of photons not detectable by spectrophotometry. To enhance detection, luminol, which is more reactive than lipoperoxides and capable of capturing their unpaired electrons, is added. This amplifies the signal detected by the luminometer. The delay in the rise of the ABAP curve indicates the extent to which antioxidants in the sample hinder lipoperoxide formation, particularly low-molecular weight antioxidants.
The reaction mixture comprises 50 μL of saliva or plasma diluted 1:50, 850 μL of glycine buffer pH 8.6, 50 μL of luminol solution (0.0398 mg/mL), and 50 μL of ABAP solution (54.24 mg/mL). Trolox (6-hydroxy-2,5,8-tetramethylchroman-2-carboxylic acid), a water-soluble analog of α-tocopherol, serves as the reference standard antioxidant. Results were analyzed using OriginLab 7.5 software, and antioxidant levels are expressed in nM of Trolox equivalents, based on the inhibition profile of the ABAP curve compared to a Trolox standard solution.17
Data analysisFor each variable, Fisher's exact test for independence was employed to examine associations between categories and groups. In cases where expected frequencies were minimal, potentially leading to injury, the Monte Carlo method was utilized as an association test with a significance level of 5%. This method serves the same purpose as the Chi-square test for independence but is statistically more robust under conditions where assumptions may not hold.
Data were presented as means ± standard error of the mean. Normality of data distribution was assessed using the Shapiro–Wilk test. Parametric tests (such as Student's t-test) were used for variables with a normal distribution, while non-parametric tests (like Mann–Whitney U test) were applied when normality assumptions were not met. In cases involving more than 2 comparison groups, one-way ANOVA was conducted, followed by post-hoc tests (Bonferroni or Tukey) as appropriate.
Correlation analyses were performed using the Spearman rank correlation coefficient. A significance level of p<.05 was considered statistically significant for all analyses. All statistical computations were carried out using GraphPad Prism software version 9.0 (GraphPad Software, San Diego, CA, USA), and the quickcalcs online tool (http://www.graphpad.com/quickcalcs/grubbs1.cfm) was utilized for outlier detection, confirming no outliers were present in this study.
ResultsTable 1 presents the clinicopathological profile of the patients included in the study. It can be observed that 67.1% were positive for ER, with a mean of 57.6% for the Ki67 tumor proliferation index, most tumors greater than or equal to 2 cm (90%), and a predominance of the Luminal A molecular subtype (41.5%). There is also a predominance of non-menopausal patients (55.8%) aged over 50 years (67.6%) and overweight (67.3%).
Clinicopathological characteristics of patients included in the study.
| % | |
|---|---|
| Estrogen receptor | Negative: 32.9% |
| Positive: 67.1% | |
| Progesterone receptor | Negative: 55.6% |
| Positive: 44.4% | |
| ki67 proliferation index | <14%: 42.4% |
| ≥14%:57.6% | |
| Molecular subtype | Luminal A:41.5% |
| Luminal B:24.6% | |
| HER-2 amplified:6.2% | |
| Triple-negative:27.7% | |
| Tumor size (cm) | >2 cm: 90% |
| ≤2 cm:10% | |
| Histological grade | Low: 78.7% |
| High: 21.3% | |
| Body mass index (kg/m2) | Normal: 32.7% |
| Excess: 67.3% | |
| Age at diagnosis | >50 years: 67.6% |
| ≤50 years: 32.4% | |
| Menopause at diagnosis | No: 55.8% |
| Yes: 44.2% |
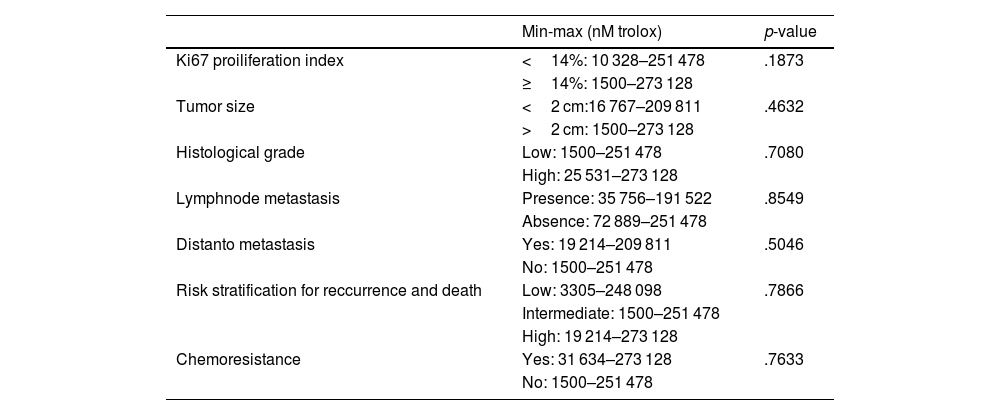
In Table 2, we observe the TRAP values according to the clinicopathological parameters of the patients evaluated. In the categorization of tumors for the ki67 index below 14%, the values varied between 10 328 and 251 478 nM of trolox, and in the group with ki67 equal to or above 14%, the values varied from 1500 to 273 128 nM of trolox. The values for the group of tumors below 2 cm ranged from 16 767 to 209 811 nM of trolox, and for the tumors equal to or above 2 cm, the values were from 1500 to 273 128 nM of trolox.
TRAP levels according to clinicopathological characteristics of patients.
| Min-max (nM trolox) | p-value | |
|---|---|---|
| Ki67 proiliferation index | <14%: 10 328–251 478 | .1873 |
| ≥14%: 1500–273 128 | ||
| Tumor size | <2 cm:16 767–209 811 | .4632 |
| >2 cm: 1500–273 128 | ||
| Histological grade | Low: 1500–251 478 | .7080 |
| High: 25 531–273 128 | ||
| Lymphnode metastasis | Presence: 35 756–191 522 | .8549 |
| Absence: 72 889–251 478 | ||
| Distanto metastasis | Yes: 19 214–209 811 | .5046 |
| No: 1500–251 478 | ||
| Risk stratification for reccurrence and death | Low: 3305–248 098 | .7866 |
| Intermediate: 1500–251 478 | ||
| High: 19 214–273 128 | ||
| Chemoresistance | Yes: 31 634–273 128 | .7633 |
| No: 1500–251 478 |
For patients with histological grade 1 and 2 tumors, TRAP levels ranged from 1500 to 251 478 nM, and those with grade 3 tumors ranged from 25 531 to 273 128 nM trolox. The TRAP values considering the presence of lymph node metastasis were 35 756–191 522 nM of trolox, and for the group without lymph node metastasis, the values ranged from 72 889 to 251 478 nM of trolox. Patients with distant metastasis presented values between 19 214 and 209 811 nM of trolox. The values for the group without distant metastasis were 1500 to 251 478 nM of trolox. Patients with a low-risk stratification of death and recurrence had values ranging from 3305 to 248 098 nM of trolox. Intermediate-risk patients presented values of 1500 to 251 478 nM of trolox, and high-risk patients values between 19 214 and 273 128 nM of trolox. Finally, patients responsive to treatment presented values between 31 634 and 273 128 nM of trolox, while chemoresistant patients presented values between 1500 and 251 478 nM of trolox. No comparison showed statistical significance between the variables in this table (p>.05, Fisher's test).
Fig. 1A shows the comparison between the salivary TRAP levels of patients with BC according to the tumor estrogen receptor expression. It was observed that samples with positive expression for the estrogen receptor had a lower TRAP compared to samples with negative status. The ranges varied between 1 and 480 nM of Trolox for ER+ and from 50 to 500 nM for ER− (p=.049).
. * indicates p<.05.")
TRPA levels according to hormonal receptors status and molecular subtyping of breast tumors. A: estrogen receptor status, B: progesterone receptor status, C: molecular subtypes of BC. ER=estrogen receptors, PR=progesterone receptors, −=negative, +=positive, LumA=Luminal A, LumB=Luminal B, HER2=HER2-amplified, and TN=triple-negative. The data are represented in box plots (min–max). * indicates p<.05.
In Fig. 1B, a salivary TRAP profile for patients is observed according to the expression of progesterone receptors in the tumor tissue, where those with breast tumors with positive PR expression showed lower TRAP than those with negative tumor expression. ER+’s minimum and maximum ranges for ER+ were 1–480 nM and 50–500 nM trolox for ER−, (p=.044).
In Fig. 1C, salivary TRAP increases in patients with tumors of the triple-negative molecular subtype compared to those with the Luminal A, Luminal B, and HER2 subtypes. The minimum and maximum values found for triple-negative ranged from 30 to 480 nM; for Luminal B, they ranged from 50 to 420, and Luminal A values ranged from 1 to 500 nM (p=.041).
Correlations were identified between salivary TRAP values and some parameters associated with a worse prognosis of BC (Table 3), such as the absence of estrogen receptors (R=−0.1881), absence of progesterone receptors (R=−0.1837), increased ki67 proliferation index (R=0.1697), occurrence of the triple negative molecular subtype (R=0.2078), and occurrence of distant metastasis (R=0.1080). The p-values of all correlations were >.05.
Spearman's correlations.
| TRAP vs. ER | TRAP vs. PR | TRAP vs. KI67 | TRAP vs. Molecular subtype | TRAP vs. Tumor size | TRAP vs. Grade | TRAP vs. Lymphnode metastasis | TRAP vs. distant metastasis | TRAP vs. risk stratification | TRAP vs. chemoresistance | |
|---|---|---|---|---|---|---|---|---|---|---|
| Spearman R | −0.1881 | −0.1837 | 0.1697 | 0.2078 | −0.01705 | 0.04187 | −0.001655 | 0.1080 | 0.02520 | −0.07179 |
| IC 95% | −0.4341 to 0.08401 | −0.4304 to 0.08858 | −0.1055 to 0.4207 | −0.06883 to 0.4548 | −0.2837 to 0.2520 | −0.2310 to 0.3087 | −0.2967 to 0.2936 | −0.2155 to 0.4101 | −0.2443 to 0.2911 | −0.3564 to 0.2250 |
| p-value | .1611 | .1714 | .2112 | .1279 | .8998 | .7593 | .9912 | .5015 | .8524 | .6278 |
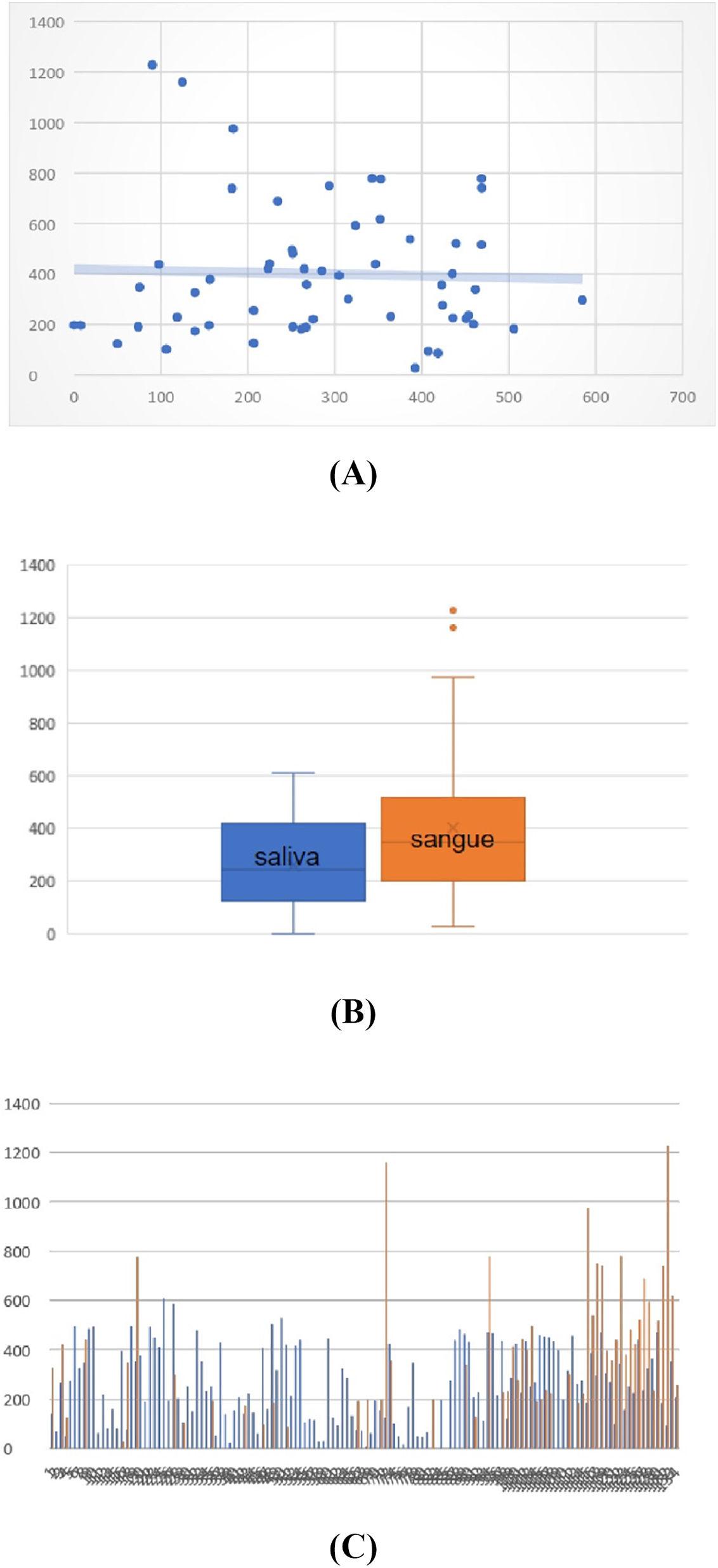
Regarding the correlation analysis between TRAP levels in saliva and blood, we observed in Fig. 2A that there is no significant correlation (R=0.0013). In Fig. 2B, we also observed that the numerical values of TRAP in blood are higher than those found in saliva, but this difference was not significant. The minimum and maximum values of the saliva samples maintained an average of 400 nM trolox, while the values of the blood samples varied from 10 to 1200 nM trolox. Furthermore, analyzing paired samples between blood and saliva individually, the values do not have any correspondence (Fig. 2C).
. In B, mean saliva and blood range. In C, individual levels of TRAP in saliva (blue lines) and blood (orange lines). (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)")
Correlation between TRAP levels in saliva and blood. In A, regression analysis shows no correlation between TRAP levels in blood and saliva (R=0.0013). In B, mean saliva and blood range. In C, individual levels of TRAP in saliva (blue lines) and blood (orange lines). (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
Our study demonstrates significant variations in the antioxidant profile of saliva depending on the clinical, morphological, and immunohistochemical profile of BC. Using the TRAP technique, we observed changes in salivary antioxidant levels that correlated with key parameters influencing BC prognosis, particularly the hormone receptor profile and tumor molecular subtypes. This novel information contributes significantly to the search for BC biomarkers with clinical applications.
The TRAP technique is highly sensitive, capable of detecting minimal variations in low-molecular weight antioxidants present in the sample. Although not specific to a particular antioxidant type, TRAP provides a comprehensive assessment of oxidative stress balance by measuring the consumption of non-enzymatic antioxidants like uric acid, carotenoids, glutathione, and tocopherols, in response to lipoperoxides generated from oxidative stress.18,19
While systemic variations in TRAP have been documented in BC patients, particularly in plasma studies showing elevated oxidative stress levels and depleted TRAP capacities in advanced stages and recurrence,20 our study explored the meaning of salivary TRAP levels. Herrera et al.20 found higher TRAP levels in tumor tissues compared to adjacent non-tumorous breast tissue, indicating that BC cells may increase antioxidant production to counteract inflammatory changes induced by the immune response against the tumor.10
BC comprises distinct molecular subtypes, each with different clinical prognoses. Our findings revealed that patients with estrogen and progesterone receptor-positive tumors exhibited lower salivary TRAP levels compared to those with receptor-negative tumors. Conversely, patients with triple-negative BC showed increased salivary TRAP levels compared to hormone-positive subtypes (Luminal A and B) and HER-2 amplified subtypes.
Inflammation plays a pivotal role in BC, influencing oxidative stress markers differently across molecular subtypes. Luminal tumors exhibit high oxidative stress and inflammatory cytokine levels, whereas triple-negative tumors demonstrate reduced tumor necrosis factor-alpha and elevated oxidative and nitrosative stress levels.20 This disparity likely contributes to the observed differences in salivary antioxidant levels among BC subtypes.
Saliva, traditionally studied for specific cancer biomarkers, also serves a critical role in modulating oxidative damage in the oral cavity.21 Salivary antioxidants mitigate lipid peroxidation induced by ingested food and counteract reactive species, thereby influencing saliva composition directly affected by oxidative stress.22 Studies in oral cancer have identified salivary antioxidants like glutathione as significant biomarkers for disease detection,23 underscoring the relevance of our findings in aggressive BC, especially in patients with mutations in the BRCA1 gene.24
Our study did not find significant correlations between saliva and blood antioxidant levels in BC patients, indicating that saliva composition does not mirror blood composition. Blood TRAP levels were consistently higher than saliva levels, likely due to greater oxidative challenges in the bloodstream compared to the oral cavity.25
Limitations of our study include a modest sample size, which restricted pairing of saliva and blood samples across clinicopathological subgroups. Additionally, saliva volume limited assessment to TRAP alone, omitting other crucial redox balance molecules like hydroperoxides and nitric oxide metabolites. Future research should validate our findings in larger patient cohorts and explore additional oxidative stress markers to enhance understanding and clinical utility. Therefore, our study provides initial evidence of a correlation between BC clinical presentation and saliva antioxidant levels, particularly in aggressive molecular subtypes like triple-negative BC. Further investigation is warranted to validate these findings and explore new oxidative stress markers that could enhance BC diagnosis and treatment monitoring.
ConclusionSaliva plays a crucial role in maintaining health. Our study revealed that while no direct correlations were observed between antioxidant levels in blood and saliva samples, salivary TRAP levels were notably elevated in women with triple-negative BC compared to those with estrogen and progesterone receptor-positive tumors. These findings underscore significant variations in clinical and pathological parameters associated with poor prognosis, including the triple-negative molecular subtype, high Ki67 expression, and the presence of distant metastasis. This suggests that salivary TRAP could serve as a potential biomarker for hormone-negative BC.
These results highlight the potential of saliva as a non-invasive source for monitoring oxidative stress and assessing disease progression in BC, particularly in aggressive subtypes where conventional biomarkers may be limited. Further research is needed to validate these findings in larger patient cohorts and explore the broader utility of salivary biomarkers in personalized cancer care.
FundingCarolina Panis is supported by Fundação Araucária (Call number 048/2021-PRPPG/Unioeste and 02/2022), Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES, Call number 01/2019), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq grants number 402364/2021–0, 441017/2023–1, and 305335/2021–9).
Ethics approval and consent to participateCAAE 35524814.4.0000.0107, ethics opinion number 6.129.064.
Patients consentThe authors declare that they obtained the patient's consent for publication of the article.
Authors' contributionAll authors equally contributed to the study conception and design, material preparation, data collection and analysis, and manuscript writing and revision.
Authors' contribution: All authors contributed to the study conception and design, material preparation, data collection and analysis. The first draft of the manuscript was written by Mariane Fontana Mezoni and Carolina Panis, and all authors read and approved the final manuscript.
The authors would like to thank all patients who agreed to participate in this work and Francisco Beltrão Cancer Hospital (CEONC) for collaborating with the study.

