



Given the inclusion of the Complex Post-Traumatic Stress Disorder (C-PTSD) in the International Classification of Diseases (ICD-11), this article analyses the C-PTSD as a possible new diagnosis in women victims of gender-based violence to explain a wide range of symptoms resulting from interpersonal, persistent, continuous, severe, and uncontrollable traumas that may occur in this context. Thus, it describes the psychological impact and the psychopathological consequences it produces on the victims, which are most serious when the violence suffered has occurred repeatedly and over time. In addition, it delves into the differential diagnosis of C-PTSD with other psychopathologies. Finally, a protocol for forensic psychological assessment is proposed based on C-PTSD as a clinical disorder, which explains the serious psychological impact on the evaluation of women victims of gender-based violence, considering this disorder as an alternative diagnostic hypothesis in the forensic psychological assessment of the psychological injury.
Dada la inclusión del Trastorno de Estrés Postraumático Complejo (TEPT-C) en la Clasificación Internacional de Enfermedades (CIE-11), en el presente artículo se analiza el TEPT-C como un nuevo diagnóstico posible en mujeres víctimas de violencia de género que explica una amplia gama de síntomas resultantes de traumas interpersonales, persistentes, continuados, graves e incontrolables que pueden darse en este contexto. Se describen las consecuencias psicopatológicas que sufren las víctimas, que son de mayor gravedad cuando la violencia sufrida se ha dado de forma repetida y prolongada en el tiempo. Asimismo, se profundiza en el diagnóstico diferencial del TEPT-C con otras psicopatologías. Finalmente, se propone un protocolo de evaluación psicológica forense atendiendo al TEPT-C como un cuadro clínico en el caso del impacto psíquico grave en la valoración de mujeres víctimas de violencia de género, considerando este trastorno como una hipótesis diagnóstica en la valoración psicológica forense de la huella psíquica.
Female victims of gender violence usually develop psychological sequelae. These are more severe when the violence suffered has occurred repeatedly and for a prolonged period of time, and may even lead to the development of complex traumas. The definition1 of gender violence also includes the threat of violent behaviour, coercion, and/or deprivation of the victim's freedom.
The high prevalence of mental health-related symptoms and disorders among these women in Europe coincides with reported data on symptoms of post-traumatic stress disorder (PTSD) and other psychopathologies reported by different studies.2–4 A relevant fact is the likelihood that the great suffering of these female victims of gender violence impacts their mental health as a consequence of a pattern of repeated victimisation within the intimate partner context.5
Victimisation in these cases is notably associated with a greater risk of mental disorders. In fact, the most common psychopathological consequences of female victims of gender violence are depression and PTSD, with frequent comorbidity between both clinical conditions.6–8
Of note is the fact that the number of gender violence reports in Spain is increasing. Thus, the General Council of the Judiciary (2022)9 reports that “the number of gender violence reports increased by 12.33%.” For this reason, carrying out forensic psychological evaluations on women who report gender violence is essential to highlight the psychological damage they may suffer.
Having contextualised the topic, the inclusion of a new disorder in the 11th edition of the International Classification of Diseases (ICD-11), written by the World Health Organisation (WHO) is salient: complex PTSD (C-PTSD), which can develop after exposure to one or more truly threatening or awful events, which are usually prolonged or repetitive and when escape from them is highly complex or totally impossible.10
It is important to bear in mind that with the inclusion of C-PTSD female victims of gender violence, who have been violated in a serious, prolonged, and repeated manner over time, can be correctly diagnosed and receive specific medical–psychological care to address the problems caused by the said phenomenon and their cases can be brought to trial and properly assessed.11
Currently, little scientific literature exists on C-PTSD in gender violence.12 This paper aims to provide a scientific answer and expand knowledge about this new disorder in order to provide a precise and contrasted response from the field of forensic psychology to those cases of particularly serious gender violence, i.e., those that present the characteristics of persistence, uncontrollability, and continuity.
The main objective of this article is to provide a specific forensic psychology assessment protocol for female victims of gender violence with symptoms compatible with C-PTSD. Specifically, it aims to establish the most appropriate quantitative and qualitative measurement tools to make an appropriate differential assessment and forensic discussion and consequently correctly assess the impact of gender violence as a situation of criminal victimisation.
Complex post-traumatic stress disorderWhen traumatic psychopathology is assessed in relation to the impact of a situation of criminal victimisation, the most representative diagnostic disorder is PTSD.7 This is so in cases of female victims of gender violence, where PTSD shows a high prevalence along with other clinical conditions.2
The high comorbidity that women with this diagnosis present may imply complicated assessment. Due to these and other limitations, a new nosological entity was proposed, C-PTSD,13 that includes serious alterations in the psychological functioning of the victims that do not completely match with the symptomatology of simple PTSD.
C-PTSD included in ICD-11 is a new disorder that describes the more complex reactions typical of people exposed to a chronic traumatic situation. This disorder, unlike PTSD, provides greater precision in the diagnosis of traumatised populations, as well as a more personalised and effective assessment and intervention.12
Of particular mention is a meta-analysis conducted by Redican et al. (2021),14 in which they concluded that numerous studies demonstrated support for the factorial and discriminating validity of PTSD and C-PTSD, when analysed together with other variables. Each of the diagnostic clinical conditions appears to describe a population with previously unrecognised clinically distinctive characteristics, as well as specific needs for intervention and treatment. Research has generally supported its validity and usefulness.15
In 1992, psychiatrist Judith Herman introduced the concepts Complex Trauma and C-PTSD in her book called Trauma And Recovery and her article titled Complex PTSD: A syndrome in survivors of prolonged and repeated trauma.16 According to Herman, the diagnostic criteria for C-PTSD included exposure to “totalitarian control,” which may last from months to years. It also generally includes physical and/or sexual abuse, from which are derived the symptoms consisting of alterations in the following areas:
- •
Emotion regulation (permanent dysphoria or suicidal impulses or self-harm, explosive anger or inhibition, compulsive or excessively inhibited sexuality, or an alternation between them).
- •
Consciousness (amnesia of traumatic events, dissociative episodes, reliving experiences in the form of intrusive PTSD symptoms, or worries).
- •
Self-perception (feeling of helplessness, shame or guilt, or of stigma and being different from others).
- •
Perceptions of the perpetrator (concern for the perpetrator or for getting revenge on him, or idealisation or paradoxical gratitude or acceptance of the value system, and rationalisations of the perpetrator, etc.).
- •
Relationships with others (isolation and distancing and/or constant search for a rescuer and/or constant failures in self-protection).
- •
System of meaning (feeling of helplessness, despair, etc.).
Other prominent authors who studied C-PTSD,17 concluded that victims of prolonged interpersonal trauma have a high incidence of problems regarding regulation of emotions and impulses; memory and attention, self-perception; interpersonal relations; somatisation and with systems of meaning, and they proposed the need for further research. After years of research, the WHO finally decided to include this disorder in its ICD-11 diagnostic manual, which was published in 2018 and officially came into force in February 2022.17 It was called “Complex Post-Traumatic Stress Disorder”, which is composed of the following criteria.18
As a precondition, the diagnostic criteria for PTSD must be met. In addition, the following aspects must be met, which can occur at different levels of severity and cause significant overall impairment at, among other areas, a personal, family, social, educational, occupational level:
- •
Problems in regulating emotions.
- •
Beliefs about feeling diminished, defeated, or worthless, as well as feelings of shame, guilt, or failure related to the threatening event.
- •
Difficulties maintaining interpersonal relationships and feeling close to other people.
The psychological situation, symptoms and indicators of the disorder that, in many cases, victims of violence within the intimate partner context present, may constitute C-PTSD. The impact of trauma produces multidimensional effects and encompasses the entire psychological functioning of the person. It is therefore far more than a mere list of symptoms. This clinical condition may be explained by a pattern of interacting behaviours, variables, and factors that lead to psychological damage in women subjected to continuous, random, and unpredictable abuse.19
In the study conducted by Dokkedahl et al. (2021),20 aimed at establishing the prevalence of PTSD and C-PTSD among women victims of intimate partner violence, it was found that a relatively significant subgroup of women had symptoms of C-PTSD. It was also found that psychological violence is the highest risk factor. It is therefore important to understand and recognises the severity of this new subtype of post-traumatic stress, in addition to considering it as a working hypothesis in the assessment of female victims of gender violence.
Regarding the chronicity of trauma, a distinction should be made between specific traumatic incidents and the traumatic context. This issue of differentiating between traumatic incidents and other stress factors is especially important, given the diagnostic criteria for PTSD.21 Therefore, in C-PTSD, the importance of the traumatic context is highlighted: perceptions of chronic danger, instead of focusing on incidents. This implies considering the interpretations that women attribute to violence and daily living in chronic anticipation of danger.
Very little research on C-PTSD in female survivors has been conducted in the field of gender violence, despite the fact that many of these women are being subjected to a type of violence which in all probability leads to the manifestation of C-PTSD.22
Until the entry into force of ICD-11,10 in situations of serious and continuous gender violence, the usual diagnosis has been PTSD. However, those cases that presented symptoms not included in the disorder and that could not be explained in any other way could be misdiagnosed with other psychopathologies, such as borderline personality disorder or delusional disorder.23 This led to inadequate treatment and attention to the needs and problems of the victims.
The inclusion of C-PTSD in the ICD-11 means that, in many cases of victimisation in matters of gender violence, female victims can be correctly diagnosed and treated based on their characteristics and different problems.
Complex post-traumatic stress disorder as a psychological imprintForensic psychological assessment consists of the exploration of all relevant aspects of a subject or subjects and is aimed at responding to the legal demands, thereby contributing to decision-making regarding criminal behaviour and its implications.23
The verification of psychological damage carries a probative value of victimisation in criminal cases, where in many cases the crime occurs in private circumstances and without witnesses. Hence, the importance of considering all possible diagnostic hypotheses when facing the assessment of female victims of partner violence. It should be noted that there is a high probability of suffering psychological damage as a consequence of being a victim of violence (injury or sequelae).24
According to the authors, “the damage or psychological imprint is obtained through measuring the effects of a criminal act on mental health, that has been linked to both internalised and externalised symptoms or behavioural problems.”24 It is, however, true that in forensic practice mostly internalised symptoms are assessed, and specifically those referring to PTSD in traumatic situations.
Regarding C-PTSD assessment in cases of gender violence victims, the usual forensic psychological assessment methodology will be taken into account: interviews, observation, self-reports, psychometric tests, and ad hoc questionnaires.23
There are specific tools to evaluate C-PTSD, such as the International Trauma Questionnaire (ITQ) 25 and the Complex Trauma Inventory (CTI), 26 that are able to discriminate between PTSD and C-PTSD.
However, to date, no validated protocol has yet been proposed to assess this psychopathology in victims of gender violence, controlling for the bias of the forensic context. Therefore, this article aims to provide a specific forensic expert assessment protocol for victims of gender violence, who present symptoms consistent with C-PTSD.
Forensic assessment protocol proposalThe methodology required by an expert psychological report generally implies that the assessment method used meets validity criteria and, therefore complies with the knowledge accepted by the scientific community.27 The assessment protocol must also meet the standard of proof and the minimum required characteristics in order to ratify the hypothesis that was concluded in the opinión.28
When conducting an expert assessment of psychological trauma, the diagnostic nosology is essential, since it is addresses both an experience and different sets of persistent symptoms, which are required to meet the criteria and make the diagnoses that are most commonly associated with exposure to adverse and/or traumatic events.29 Since C-PTSD has recently been introduced in the ICD-11,18 this implies considering an assessment protocol that validates its diagnostic assessment, emphasising exposure to multiple and/or inevitable traumas and taking into account the complexity to assess poorly accessible psychological aspects, that are characteristic of this clinical condition.
Regarding the assessment procedure for C-PTSD, valid protocols for forensic psychological assessment of psychological damage in victims will be taken into account, in order to avoid expert errors and guarantee the admissibility of expert evidence in the judicial context.13,23,24
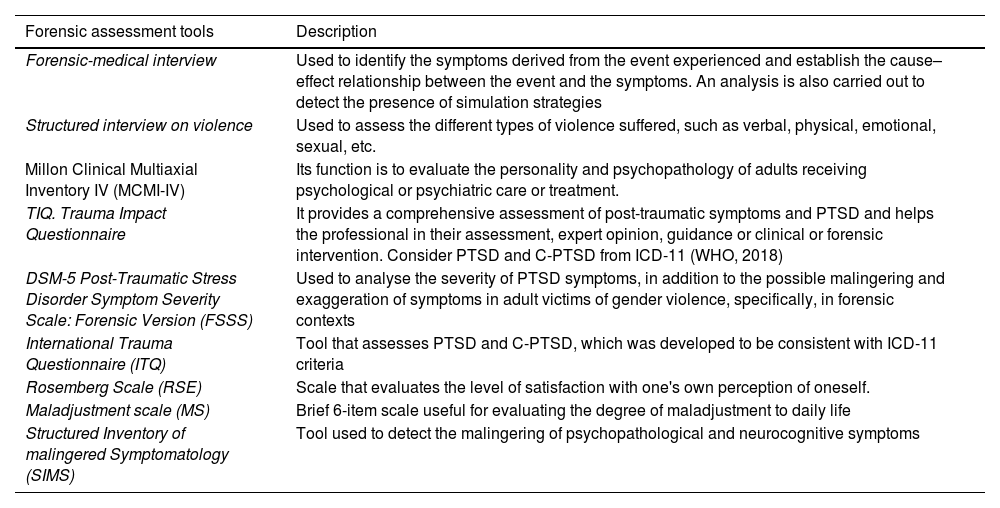
Important to bear in mind is the fact that a forensic psychological assessment protocol proposal in matters of gender violence, integrating the C-PTSD hypothesis, firstly involves conducting a forensic–psychological interview and then a structured interview on violence. Through these interviews’ data would be collected to identify the victim's symptomatology, the relationship between the event suffered and the symptoms, and the detection of the presence of simulation strategies, together with assessment of the different types of violence suffered. Subsequently, psychometric tests would be administered aimed at evaluating different aspects. Table 1 describes each test.
Forensic assessment tools.
| Forensic assessment tools | Description |
|---|---|
| Forensic-medical interview | Used to identify the symptoms derived from the event experienced and establish the cause–effect relationship between the event and the symptoms. An analysis is also carried out to detect the presence of simulation strategies |
| Structured interview on violence | Used to assess the different types of violence suffered, such as verbal, physical, emotional, sexual, etc. |
| Millon Clinical Multiaxial Inventory IV (MCMI-IV) | Its function is to evaluate the personality and psychopathology of adults receiving psychological or psychiatric care or treatment. |
| TIQ. Trauma Impact Questionnaire | It provides a comprehensive assessment of post-traumatic symptoms and PTSD and helps the professional in their assessment, expert opinion, guidance or clinical or forensic intervention. Consider PTSD and C-PTSD from ICD-11 (WHO, 2018) |
| DSM-5 Post-Traumatic Stress Disorder Symptom Severity Scale: Forensic Version (FSSS) | Used to analyse the severity of PTSD symptoms, in addition to the possible malingering and exaggeration of symptoms in adult victims of gender violence, specifically, in forensic contexts |
| International Trauma Questionnaire (ITQ) | Tool that assesses PTSD and C-PTSD, which was developed to be consistent with ICD-11 criteria |
| Rosemberg Scale (RSE) | Scale that evaluates the level of satisfaction with one's own perception of oneself. |
| Maladjustment scale (MS) | Brief 6-item scale useful for evaluating the degree of maladjustment to daily life |
| Structured Inventory of malingered Symptomatology (SIMS) | Tool used to detect the malingering of psychopathological and neurocognitive symptoms |
Source: Own elaboration. ICD-11: International Classification of Diseases 11th edition; PTSD: Post-Traumatic Stress Disorder; C-PTSD: Complex Post-Traumatic Stress Disorder.
It has been observed that C-PTSD can be applied to those victims who have suffered repeated and prolonged traumatic events, such as women who have suffered gender violence.11
Regarding forensic psychological assessment, it has been shown that the use of appropriate and specific tools for assessment symptoms derived from the experience of traumatic events leads to a clear diagnosis of cases, resulting in provision of correct assessment of the victims, in addition to the designing of personalised interventions for each of them.13
We believe C-PTSD more completely and appropriately describes the psychopathology resulting from exposure to complex traumas, and it also includes a set of symptoms that reflect serious alterations in people who suffer from it. Its consideration in the preparation of a forensic psychological expert report would therefore enable a more precise differential diagnosis to be made. Diagnostic errors or concluding with other comorbid diagnoses that do not fully match the psychopathological condition of the victim would therefore be avoided. Application of the proposed protocol would control this assessment error and an appropriate practice would be conducted for this type of particularly serious cases.
Although our study has its limitations, such as the lack of references on the topic under discussion, it has been possible to verify that the inclusion and appropriate expert assessment of C-PTSD has resulted in an accurate and contrasted response in the forensic and judicial field for female victims of gender violence who have suffered complex traumatic events.11
Furthermore, using a specific forensic psychological assessment protocol will induce a clear and well-founded response to expert enquiries in cases of violence against women in the intimate partner context, highlighting the importance of psychological expert evidence in these matters.29,30
Finally, these expert reports must be carried out in an exhaustive, rigorous, and scientific manner, to provide an accurate and reasoned response to the problem assessed within the legal context.23 In so doing, the scientific admissibility control of the evidence will be addressed.
FundingThis study did not receive specific support from public sector agencies, commercial sectors or non-profit entities.
Please cite this article as: Asensi Pérez LF, Flores Fernández E, Nevado Duarte K. Psychological–forensic expert assessment of complex post traumatic stress disorder in victims of gender-based violence. Revista Española de Medicina Legal. 2024. https://doi.org/10.1016/j.remle.2023.09.001.