



Circumstances under lockdown increase the risk factors for gender-based violence (GBV) at the individual and social level due to isolation and barriers to victims in seeking help and reporting their situation. This has the direct consequence of an increase in this violence. Initially, due to the reduced number of reports and homicides, it could be mistakenly understood that there has been a decrease in GBV. The medico-legal study of GBV under lockdown must be an evolving process that contemplates its consequences in two phases: during lockdown, with the increase in all its forms (physical, psychological and sexual), and after lockdown, focusing on fatality risk assessment, which increases due to perceived loss of control on the part of the perpetrator.
Las circunstancias del confinamiento potencian los factores de riesgo de violencia de género (VG) a nivel individual y social, al aumentar el aislamiento y las barreras que dificultan la solicitud de ayuda y la denuncia. Esta situación tiene como consecuencia directa el aumento de esta violencia. Sin embargo, una primera aproximación puede llevar al error al entender que la VG disminuye debido al descenso de las denuncias y del número de homicidios. El estudio médico-legal de la VG bajo el confinamiento debe tener un sentido evolutivo que contemple las consecuencias en sus dos fases: Durante el confinamiento, con el aumento en todas sus formas (física, psicológica y sexual), y tras el confinamiento, centrándose en la valoración del riesgo de letalidad, el cual se incrementa debido la percepción de pérdida de control por parte del agresor.
The General Director of the World Health Organisation (WHO), Margaret Chan, in the presentation of the report Global and regional estimates of violence against women (2013), stated that “violence against women is a global health problem of epidemic proportions”.1 Taking the most conservative references to the size of this violence in terms of the percentage of women who suffer it, and limiting its expression to the context of couples, every year approximately 770 million women are attacked by their partners or ex-partners in the planet. This number and presence do not arouse a response that is proportional to the problem they represent.
One of the key factors in understanding the different ways health problems are perceived consists of the risk construct. The main factor that that leads a problem to be seen as a threat arises from the combination of its magnitude with how long it has been evolving in a specific geographical context, these being references that are used to refer to an epidemic or pandemic. When gender-based violence is analysed, this perception is defined by 2 elements: it is an historical problem and it consists of forms of behaviour that are intrinsic to certain contexts. It is not a social problem, which is expressed differently depending on the circumstances, an idea constructed on the basis of the myths and stereotypes which surround it.
The data on the magnitude of this problem speak volumes. The said WHO1 report states that the worldwide prevalence of gender-based violence in couples amounts to 30%, while in Europe it stands at 22.3%. The report by the EU Fundamental Rights Agency (FRA), Violence against women: An EU-wide survey,2 indicates that 20% of the women in the EU older than 18 years old suffer physical violence in the context of their relationship with their partner, while 43% suffer psychological violence and 7% suffer sexual violence at the hands of their partners or ex-partners. Likewise, the report Global study on homicide. Gender-related killing of women and girls by the United Nations3 shows that every year 50,000 women are killed in the context of gender-based violence and family relationships. In Spain, the Macrosurvey of gender-based violence in 20114 directly quantified the number of women maltreated per year at 593,038, and the annual average of homicides, according to official data shown in the statistics of the Ministry of Equality, is higher than 60.5
Gender-based violence and lockdownStudy of the characteristics of these two elements, gender-based violence on the one hand and lockdown on the other, helps to understand the impact they cause on women and society as a result of their interaction.
Elements that characterise gender-based violenceGender-based violence is often presented as just another type of interpersonal violence, in the understanding that it is characterised by its results (physical or psychological lesions, or death). This traditional approach considers it to be a part of domestic or family violence. But the differences between different types of violence lie basically in their origin and most especially in what motivates them and the goals they aim to obtain. Additionally, gender-based violence has 3 basic elements that differentiate it from other forms of violence, determining how it presents and the response to it. These elements are its structural component, the goal of control and the isolation which it involves.
The structural component of gender-based violenceThe classic works by Johan Galtung at the start of the 1970s underlined what was defined as “structural violence”, violence that arises as the result of elements in culture and social organisation that are used to prevent the satisfaction of needs.6,7 Gender-based violence is included within this structural violence, among other types, because it takes place under the construction of gender roles and sexual stereotypes, which function as risk factors and are determinant causes of the same.8 This structural component is one of the elements used by the WHO when analysing factors associated with different types of violence.9
The goal of controlThe main aim of gender-based violence is not to harm, but rather to control and subject women to the dictates and references imposed by the aggressor based on structural elements of society and culture.10 This violence therefore continues over time, during which physical, psychological and sexual attacks occur. This is why its impact on health surpasses the effect that the sum of isolated but more or less repeated attacks may have.
IsolationWithin the strategy of control, the aggressor uses structural elements at a social level as well as individual control11–13 to isolate the women from her sources of external support, fundamentally her family, friends and circles, with the dual aim of increasing control and achieving impunity for the violence used.
The interaction of these 3 elements in gender-based violence has the result that, in spite of its great prevalence, proximity and severity, the majority of cases remain invisible. Only 25–28% of cases are reported, as is shown by the comparison of data in the reports by the General Board of Judicial Power on reports with those of the macrosurveys.4 It also means that it is justified in different ways, an example of which is shown in the special Eurobarometer on domestic violence against women in 2010.14 In this 3% of the EU population stated that “there are circumstances that justify gender-based violence”, showing a passive attitude to the problem and a distance that is reflected in the barometers of the Centro de Investigaciones Sociológicas,15 as they show that, in spite of the 600,000 cases per year and an average of 60 homicides, only 1-4% include gender-based violence among the most serious problems. This passivity and distance also give rise to a lack of involvement by families and circles to help women escape from violence, as may be seen in the percentage of reports lodged by family members, amounting to 0.57%, and in the responses by professionals (for example, in medicine, reports of injuries represent only 9.6% of all reports),16 although maltreated women often visit medical services due to the health problems caused by gender-based violence.
Lockdown circumstances and their impact on gender-based violenceThe lockdown, for its part, created ideal conditions for the growth of the elements involved in gender-based violence: it isolated women even more, increasing control by formal confinement in the home, facilitating impunity by making it harder for women to escape from violence, and creating a context that facilitated the use of any of its forms if faced with the slightest stimulation.
Studies reveal that this is a habitual situation after a catastrophe or disaster, and that aggressors take advantage of the circumstances in which movement is restricted, to increase the use of violence against women.17–19 In scenarios of this type, as studies after different disasters show, (the Haiti earthquake, fires in Australia and the tsunami in Japan), there is an increase in gender-based violence with 2 components: an increase in the level of violence prior to the disaster, and the appearance of gender-based violence in relationships where it had not existed beforehand. And all of this occurs without a rise in the number of reports.20
The data shown in different newspaper reports on the evolution of gender-based violence during the lockdown confirm the situation, with a 37% increase in the number of calls to 01621 and a fall in the number of reports. All in a scenario in which the elements that increase the risk of violence against women have increased, such as alcohol consumption, with a rise in sales of 84.4%, and pornography, which rose by 61.3%.
It can therefore be stated that the lockdown trapped women in violence and freed their attackers to use it.
The consequences of the lockdown due to the pandemic for gender-based violenceConfining maltreated women to the home where they suffer violence together with the person who uses it has the direct result of increasing the level of violence and the impunity of the aggressor. This is due to the amplification of the 3 elements which characterise it: the structural component, which places the figure of the man at the centre of decision-making and the need to maintain order based on his own criterion; isolation, as the result of the material barrier against escaping from it and freely communicating, and the direct control which violence exerts over women.
In-depth analysis of the situation makes it necessary to take into account how it evolved, and therefore also to consider the potential impact of the changing situation after the end of the lockdown. The first thing that has to be evaluated is therefore the starting point, i.e., the situation of violence prior to the lockdown. The previous situation was characterised by increasing violence against women, as is also shown by a rise in the number of homicides. In 2019 there was a rise of 4 homicides (7.8%), from 51 in 2018 to 55 in 2019.5 In the first 2 months of 2020, just before the lockdown, homicides in both months were above average. More specifically, there were 7 in January, when the average number of gender-based violence homicides in this month stands at 5.6, and there were 6 in February (average 4.7, X Informe Anual del Observatorio Violencia sobre la Mujer, 2016).22
The lockdown therefore occurred in a context characterised by an increase in gender-based violence which continued during the same, as can be deduced from the first data published and as is usual in such situations, such as those which coincide with disasters and catastrophes.
In this context, analysis of the consequences of the lockdown for gender-based violence must take the medical-legal dimension into account, as well as the clinical dimension. The impact on children living in the homes in question must also be included in the results.
Clinical consequences of the lockdown in terms of gender-based violenceThe rise in gender-based violence and the elements which define its characteristics during this time, above all in terms of continuity and threat, as well as the increase in sexual violence in many cases, will have a profound impact on women’s health. This impact will depend on the time during which they are exposed to the said violence and their state of health prior to the lockdown. This refers to their health problems caused by the violence itself, as well as the existence of any other process or disease that would be aggravated by violence.
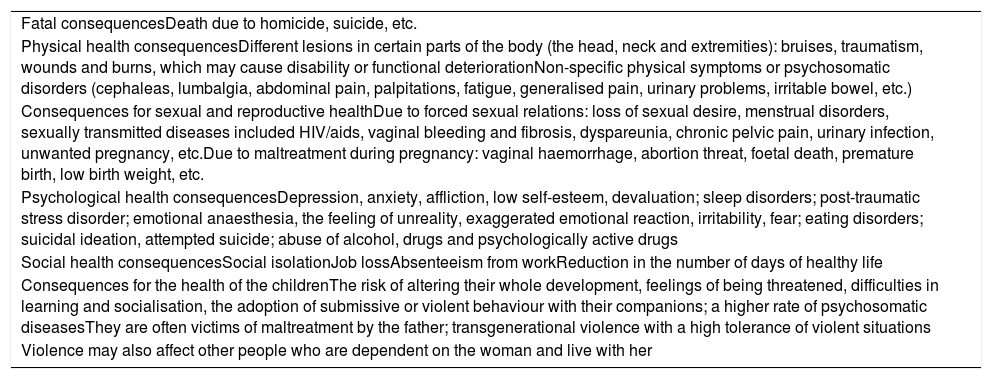
The clinical manifestations that define gender-based violence are shown in 3 planes: general physical condition, physical condition centring on the genital-urinary plane due to sexual violence, and the psychological plane. The main alterations defining these symptoms are shown in Table 1, taken from the work by Sans and Sellarés.23
Health consequences of gender-based violence.
| Fatal consequencesDeath due to homicide, suicide, etc. |
| Physical health consequencesDifferent lesions in certain parts of the body (the head, neck and extremities): bruises, traumatism, wounds and burns, which may cause disability or functional deteriorationNon-specific physical symptoms or psychosomatic disorders (cephaleas, lumbalgia, abdominal pain, palpitations, fatigue, generalised pain, urinary problems, irritable bowel, etc.) |
| Consequences for sexual and reproductive healthDue to forced sexual relations: loss of sexual desire, menstrual disorders, sexually transmitted diseases included HIV/aids, vaginal bleeding and fibrosis, dyspareunia, chronic pelvic pain, urinary infection, unwanted pregnancy, etc.Due to maltreatment during pregnancy: vaginal haemorrhage, abortion threat, foetal death, premature birth, low birth weight, etc. |
| Psychological health consequencesDepression, anxiety, affliction, low self-esteem, devaluation; sleep disorders; post-traumatic stress disorder; emotional anaesthesia, the feeling of unreality, exaggerated emotional reaction, irritability, fear; eating disorders; suicidal ideation, attempted suicide; abuse of alcohol, drugs and psychologically active drugs |
| Social health consequencesSocial isolationJob lossAbsenteeism from workReduction in the number of days of healthy life |
| Consequences for the health of the childrenThe risk of altering their whole development, feelings of being threatened, difficulties in learning and socialisation, the adoption of submissive or violent behaviour with their companions; a higher rate of psychosomatic diseasesThey are often victims of maltreatment by the father; transgenerational violence with a high tolerance of violent situations |
| Violence may also affect other people who are dependent on the woman and live with her |
Taken from Sans y Sellarés.23
The rise in violence due to the perception of impunity has 2 direct results for medical-legal questions.
InjuriesPhysical injuries may be affected by the conditions due to lockdown in two ways: on the one hand, the rise in the frequency and intensity of violence, and on the other hand, the feeling of impunity, which may lead aggressors to attack less habitual parts of the body, instead of the trunk and head where lesions usually go unnoticed as they are covered by clothing or hair. Although medical-forensic examination has to include the most usual anatomical regions, it has to be expanded to include other areas, to identify one of the characteristic features of lesions caused by gender-based violence: the different phase of lesion evolution caused by the repetition of attacks on different days.24
In the genital-urinary plane it is important to examine the consequences of sexual attacks as parts of gender-based violence. Such attacks are made under a situation of intimidation rather than the use of physical force. Examination should be completed by interviewing the woman in a structured way to discover the characteristics of the sexual attacks and certain practices that may leave injuries and signs during these days, some of which are associated with the consumption of pornography.
Psychological symptoms will depend on how long the woman has been subjected to violence. Anxiety predominates in the initial phases, while as the process evolves the reaction tends towards depression. The circumstances of the lockdown give rise to a feeling of impotence and that there is no escape, facilitating this evolution towards depressive symptoms, and these will saturate all of the other psychological manifestations.
Medical evaluation, in the clinical as well as in the medical-legal plane, must include the risk of suicide.
Increased risk of new aggressions and homicideThe other factor that must be covered by the medical-legal approach is the evaluation of the risk of new aggressions and homicide, given that the circumstances of lockdown directly affect this risk and how it evolves.
The rise in violence during lockdown is the result of the appearance of risk factors with three component parts: the risk of victimisation, the risk of new aggressions and the risk of lethality.25 The study has to distinguish between 2 temporal contexts with different consequences for risk: coexistence during the lockdown on the one hand, and on the other the period following the lockdown.
Evaluation of risk in gender-based violence during the lockdownAs we pointed out above, the main aim of gender-based violence is to control a woman. The aggressor considers this to have been achieved in this phase as women are unable to leave the home freely, and as they believe she will have very little possibility of renewing her life after a possible break-up due to the social and economic circumstances caused by the pandemic.
Risk in this phase will largely be determined by individual risk factors26 and the history of previous violence, before the lockdown as well as how it evolved during the same. These elements mean that risk factors have a greater effect on all forms of violence and the repetition of aggressions.
Risk evaluation in gender-based violence after lockdownThe end of lockdown modified how aggressors perceived the main aim of their violence: control of the woman. This, together with other factors, substantially changed the risk of further aggressions and lethality.
The most important risk factor influencing the severity of aggression and lethality is perception of loss of control over the woman who is the victim of the aggressor’s violence.25 The general risk will increase due to the presence of individual risk factors (explicit death threats, the consumption of alcohol and toxic substances, and a low level of self-esteem …). These are added to permanent risk factors (previous violence that was sustained over time, isolation – amplified in this case by lockdown -, violence against the children, a pattern of domination and control over the woman, communication problems and the objectification of women, which may have been increased by the consumption of pornography during lockdown …).8,25,26
All of these factors have to be analysed in terms of how they evolve over time, and separation from the woman must be taken into account as the most important risk factor, as it affects the perception of loss of control. Thus any initiative towards separation, by fully breaking off and separating or warning that this will occur increases the risk of new aggressions and most especially the risk of lethality.
Studies which analysed the increase in gender-based violence and homicides after disasters confirm the increase in risk following situations that facilitate control of the victim. They show that risk rises dramatically when control is perceived to be lost due to changing circumstances, especially when the woman separates or states that she intends to do so.17–20
Consequences of gender-based violence during the lockdown for childrenThe third affect of lockdown on gender-based violence arises due to the context and climate of violence created by the aggressor, using threats, control and intimidation …, all of which create an atmosphere that affects the children who live in the same home.
The 2011 macrosurvey directly quantified the number of children exposed to gender-based violence, and it concluded that there are 840,000 of them in Spain. This figure means that 10.1% of children live in conditions of gender-based violence and of these, 517,000 (6.2%) suffer direct violence by the aggressor.
The impact of gender-based violence on children who are exposed to it must also be evaluated in terms of the physical and psychological alterations it causes, as well as the risk of suffering new aggressions, with their component of lethality.
Response to gender-based violence after the lockdownTo analyse the impact of the circumstances created by the lockdown on gender-based violence, it is of key importance to commence with the meaning of this violence in terms of its motivations and goals. It also has to be taken into account that the lockdown reinforced the essential features of this violence (the structural component in its origin, the isolation that it causes and the control it imposes). Otherwise, a first approximation may lead to confusion and the error of believing that the data which show a fall in the number of reports and homicides means that gender-based violence fell too.
It has been explained that gender-based violence increased during lockdown (as deduced from the indirect data we evaluated) and that it did so from the starting-point of a context characterised by a high level of violence, which functions as a risk factor for the future.
Medical-legal action against gender-based violence during lockdown will depend on the cases approached from a medical-forensic viewpoint after a report is lodged. However, it is always necessary to insist on the importance of detection, especially within the medical context, given that the impact of this violence on women’s health means they often visit for medical attention and care. Nevertheless, this requisite prior to detection and the lodging of a report restricts the forensic medicine response.
The major challenge lies in the response at the end of lockdown. This response centred on 3 major actions, which were located (as we did when presenting the consequences) in the contexts of clinical and legal medicine.
The response of clinical medicine to gender-based violence after the lockdownThe deterioration in health caused by the violence suffered during the lockdown and the resulting worsening of the symptoms associated with other pathologies increased the demand for medical attention even when lesions were not the characteristic symptoms. This means that a strategy for active detection is required for cases of gender-based violence, with the dual aim of properly treating the pathologies presented by women and helping to adopt measures to manage the risk of further attacks or homicide.
The response of legal and forensic medicine to gender-based violence after the lockdownLegal and forensic medicine have to act towards 2 basic goals:
Evaluation of the gender-based violence sufferedThe circumstances of the lockdown meant that violence was more continuous and repeated, and that attacks could be directed at anatomical regions other than the usual ones. Above all they led to increased psychological and sexual violence, and the impact intensely affected any children living at home. Medical-forensic study therefore has to take all of these elements into account when evaluating a case as a whole.
Risk evaluation after the lockdownMedical-forensic action should have the main aim of evaluating the risk factors which indicate the existence of a more or less high probability of new aggression occurring, as well as determining the lethal risk for the woman and her children.
The elements we have collected will be taken into account for the above-mentioned purpose, and this must be done in a way which shows how they have evolved over time. The factor which most raises the risk of homicide is when an aggressor perceives that he has “lost control” of the victim, and the clearer this loss of control, the higher the risk (if the woman announces she is leaving or does so, with a formal separation, or divorce …). The scientific literature describes how homicide in cases of gender-based violence is 3 times higher in women who have separated than it is for those who still live with their aggressor.27 Such homicide tends to occur in the first 12 months after separation,28 and beforehand the aggressor usually behaves by harassing the woman.29,30 Studies show that this risk rises objectively, but also that a margin exists in which it can be evaluated, before acting on the basis of findings.
Risk evaluation must be performed using the available instruments, including the Medical-forensic protocol for the urgent evaluation of risk in gender-based violence,31 and any other protocol that has been included by the Comprehensive Evaluation Forensic Units, but always taking the particular circumstances of each case into account together with the elements associated with homicide: perception of loss of control over the victim, changes in aggressor behaviour (increased violence, harassment after separation, increased consumption of toxic substances, tighter control of the woman, jealousy as an argument …), as well as the personal situation of the aggressor.25 All of these elements and factors create a situation of risk that is liable to be precipitated by a factor leading to homicide or a severe attack.
The key factor is to understand that knowledge of gender-based violence and the circumstances used by the aggressor to carry out further attacks mean that there is time and a margin for the identification of the situation and develop preventive and protective measures. It is therefore extremely important to adopt a proactive strategy and define protocols and strategies to apply it.
We now know that lockdown produces an increase in gender-based violence and risk, although we also know how to deal with the situation to add to women’s safety and allow them to escape from the violence that locks them into more than 4 walls. And in all of this, legal and forensic medicine plays an essential role.
Please cite this article as: Lorente Acosta M. Violencia de género en tiempos de pandemia y confinamiento. Rev Esp Med Legal. 2020;46:139–145.