







Attention deficit hyperactivity disorder (ADHD) is the most common childhood neurodevelopmental disorder, with an estimated prevalence in adulthood of 2.5–3.4%. The Attention Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) is an 18-item self-administered scale that assesses attention deficit and hyperactivity/impulsivity symptoms of ADHD in adults. This study aims to validate the ADHD-RS in Spanish according to the diagnostic criteria established by the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5).
Materials and methodsA sample of 441 adult patients (mean age 33.34±11.37 years) was included, 396 subjects were diagnosed with ADHD (mean age 33.17±11.18 years), and 45 were controls (mean age 35.40±12.33 years). The clinical diagnosis of ADHD was established according to the DSM-5 criteria. The ADHD-RS was subsequently administered to all participants.
A logistic regression study evaluated the model in terms of sensitivity, specificity, positive predictive value, and negative predictive value. The Kaiser-Meyer-Olkin (KMO) measure was performed to assess the adequacy of the data set, and to determine whether factor analysis was applicable, Bartlett's sphericity test was performed.
Principal component analysis was used, using the Varimax orthogonal rotation method, which minimizes the number of variables with high loads on each factor, obtaining two factors and thus, simplifying their interpretation.
ResultsThe cut-off point that best discriminates the combined presentation of ADHD was 24 points, with a sensitivity of 94.78%, a specificity of 84.79%, a PPV (positive predictive value) of 93.74%, and an NPV (negative predictive value) of 78.33, with an area under the curve (AUC) of 0.85, and a kappa coefficient of 0.86.
Regarding inattentive ADHD, the cut-off point that best discriminates was 21 points, with a sensitivity of 92.56%, a specificity of 76.26%, a PPV of 92.01%, an NPV of 78.33%, an AUC of 0.90, and a kappa coefficient of 0.87.
Different cut-off values in the two subgroups suggests that a differentiated cut-off point for the inattentive and combined presentations may be an adequate assessment strategy for ADHD in adulthood.
ConclusionsThe Spanish version of the ADHD-RS is a valid instrument to evaluate ADHD in adults according to the diagnostic criteria established by the DSM-5.
Differentiated cut-off points for the inattentive and combined presentations discriminate more accurately than a single cut-off point.
Attention deficit hyperactivity disorder (ADHD) is the most common childhood neurodevelopmental disorder,1,2 characterized by a persistent pattern of inattention and/or hyperactivity–impulsivity that interferes with the subject's normal functionality or development.1,3 Its approximate prevalence is 6.5% in children, with persistence in adulthood of between 2.5 and 3.4%.4
Adult ADHD has been associated with greater psychiatric5 and medical6 comorbidity, poorer academic adjustment,7 work instability, and higher unemployment.8 At the social level, untreated patients with ADHD present poor performance, with higher rates of divorce,8 frequent changes of address,9 economic difficulties,9 and early parenthood.9 They are also associated with a higher mortality rate, especially due to accidents.2,6,10
The publication of the 5th edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)11 established some changes in both the categorization and diagnostic criteria of ADHD compared to the DSM-IV-TR. Thus, ADHD disappears from the specific chapter of “child and adolescent disorders” and is included in the chapter of neurodevelopmental disorders,11 establishing the conceptualization of ADHD as a lifelong disorder. Likewise, the diagnostic criteria required in adulthood were reduced from 6 to 5, the age range for identifying symptoms in childhood was extended from 7 to 12 years, and the exclusion criteria were modified.3
The Attention Deficit/Hyperactivity Disorder Rating Scale (ADHD-RS) is a self-administered assessment scale used to measure symptoms of inattention, hyperactivity, and impulsivity. Originally developed for children and adolescents, it has subsequently been validated in adults. The ADHD-RS examines the 18 symptoms defined by the DSM-5 (nine criteria for inattention and nine criteria for hyperactivity/impulsivity). It has good psychometric properties, with a cut-off score of 24 points in its original version12 and 17 points in a subsequent validation study in Spanish population.13
A previous validation study in Spanish of the ADHD-RS according to DSM-IV criteria suggested that different cut-off points for inattentive and combined presentations discriminated better than a single cut-off value,14 establishing 24 as the cut-off point that best discriminates the diagnosis of ADHD. A new proposal for a score of 21 points has been suggested in the case of the presentation with a predominance of attention deficit.14
The main objective of this study was to validate the ADHD-RS in Spanish adult population, according to the update of the diagnostic criteria established by the DSM-5.11 A secondary objective was to validate the proposal of differentiated cut-off points according to the different clinical presentations of ADHD.
Materials and methodsDesign of the study and patientsThis study was conducted in the adult ADHD Program of the Psychiatry Department of the Vall d’Hebron University Hospital in Barcelona. This is a suprasectoral program that receives patients with a suspected diagnosis of ADHD, referred from primary care and mental health centers. This study was approved by the Clinical Research Ethics Committee of the Vall d’Hebron University Hospital with number PR(AG)103/2019.
The sample comprised 441 patients, 396 diagnosed with ADHD, and 45 controls. The mean age of the sample (patients and controls) was 33.34±11.37 years, and 62.82% were male. Participants were recruited consecutively from July 2013 to November 2018.
The following inclusion criteria were established: to be over 18 years of age, to sign the informed consent, and in the subgroup of cases, to meet the diagnostic criteria for ADHD according to the DSM-5.
All participants voluntarily agreed to participate in the study and did not receive any financial compensation.
Instruments and proceduresThe clinical diagnosis of ADHD was made by psychiatrists and psychologists from the adult ADHD Program of the Psychiatry Department of the Vall d’Hebron University Hospital. The clinical diagnosis of ADHD was made according to the criteria established by the DSM-5.
Complementarily, and to perform a systematic and standardized assessment of psychiatric comorbidity, the Structured Clinical Interview for DMS IV (SCID-I and II) adapted to the DSM-5 was administered to all patients.15,16
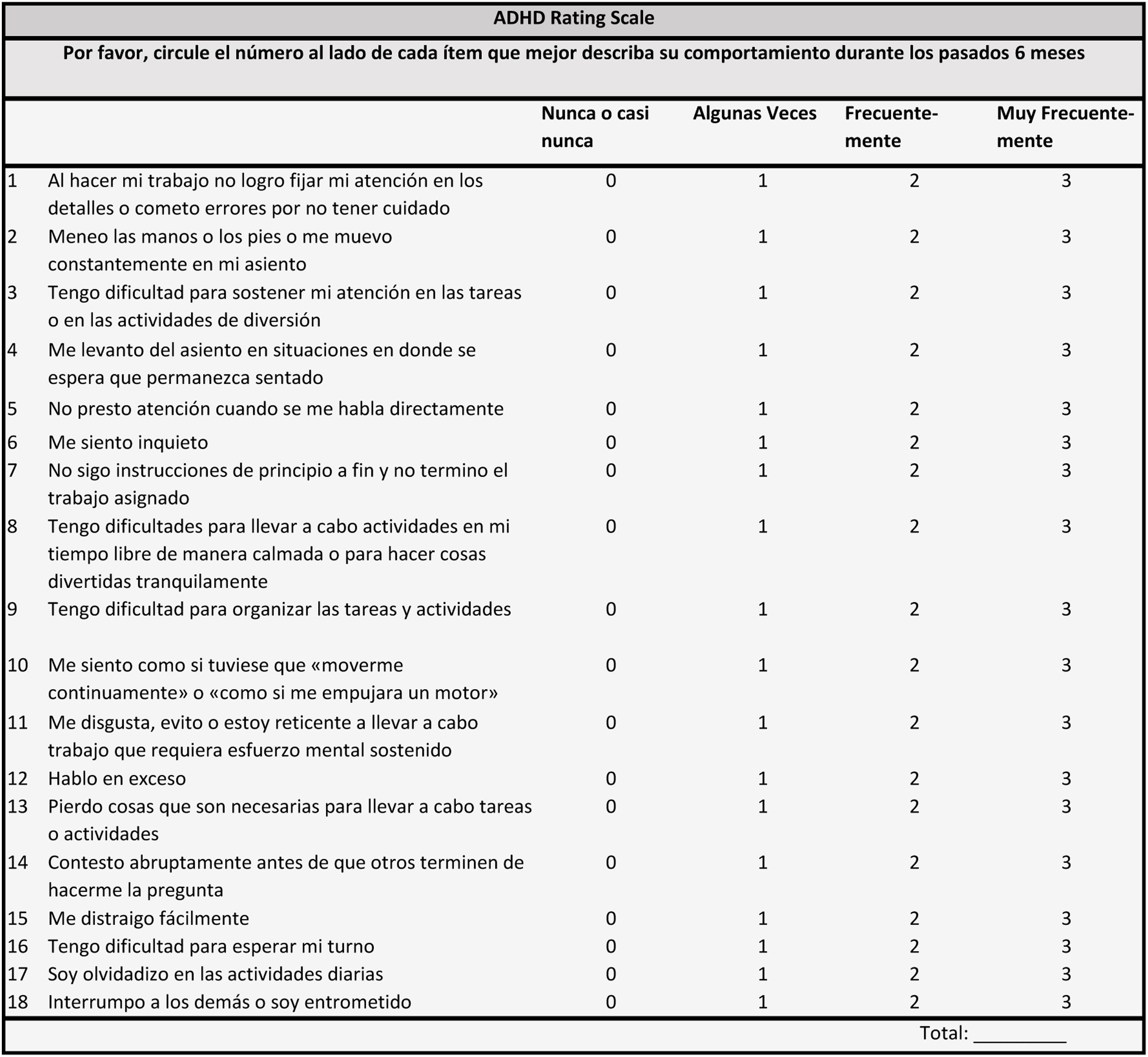
The ADHD-RS includes 18 items that explore the criteria established by the DSM-5 for ADHD. It consists of two subscales of 9 items, one related to inattentive symptomatology and the other to hyperactive and impulsive symptomatology.17 The items can present a minimum value of 0 and a maximum value of 3 points. The final result is the algebraic sum of the scores of each item, with 0 points being the lowest total score that can be obtained and 54 points the maximum. Initially, the scale was designed to be administered to children and was validated.18 However, it was subsequently adapted for adults. This scale can be self-administered or completed by an expert clinician (Annex 1).
.")
In its original version, a score equal to or greater than 24 points was considered significant.12 A subsequent validation study of the scale suggested that a differentiated cut-off point for inattentive and combined presentations would discriminate better than a single cut-off point.14
All participants completed the ADHD-RS in its Spanish version, based on DSM-5 criteria. The instrument was self-administered, as the participants were adults (in children and adolescents, it is usually completed by their parents).
Statistical analysisThe statistical analysis was conducted using IBM SPSS Statistics version 28.0.0.0. First, a descriptive study of all the target variables was carried out, and then, the chi-square test was used to perform the comparative analysis.
A logistic regression analysis was performed to determine the cut-off point that best discriminated between cases and controls in terms of sensitivity (probability that a participant diagnosed with ADHD will obtain a positive test result), specificity (probability that a healthy participant will obtain a negative result in the test), positive predictive value [PPV] (probability that a test-positive participant will receive an ADHD diagnosis), negative predictive value [NPV] (probability that a participant with a negative test result will not receive an ADHD diagnosis), and area under the curve [AUC] (where values close to 1 indicate higher agreement between the predicted and the actual diagnosis).
To assess the adequacy of the data set, the of Kaiser-Meyer-Olkin (KMO) measurement, which can take values between 0 and 1, was performed. A value close to 1 indicates a good fit for factor analysis, while a value close to 0 indicates a poor fit. To evaluate whether factor analysis was applicable, Bartlett's sphericity test was performed. A principal components analysis was performed using the Varimax orthogonal rotation method, which minimizes the number of variables that achieve high loads on each factor, obtaining two factors and simplifying their interpretation.
ResultsThe total sample was 441 adults: 396 with ADHD diagnosis and 45 controls. The mean age of the participants with ADHD was 33.17 years, with a standard deviation of 11.18 years. The mean age of the controls was 35.40 years, with a standard deviation of 12.33 years. Concerning sex, 62.80% of the patients and controls included were male. Regarding comorbidity, 53.88% had psychiatric comorbidity, the most frequent was nicotine use disorder (38.23%) and anxiety disorder (31.88%). After data analysis, no significant group differences were observed in age and sex, nor were any significant differences found in comorbidity between the group of participants diagnosed with ADHD and the control group.
Using a strategy with a single cut-off value of 24 points for all presentations, we observed a sensitivity of 92.14%, a specificity of 60.24%, a PPV of 90.42%, an NPV of 78.01%, an AUC of 0.81, and a kappa coefficient of 0.81 (Table 1).
Using the strategy of differentiated cut-off points for inattentive and combined presentations, we observed a better discrimination power between cases and controls.
The cut-off point that best discriminated for the combined presentation corresponded to 24 points, with a sensitivity of 94.78%, a specificity of 84.79%, a PPV of 93.74%, an NPV of 78.33%, an AUC of 0.85, and a kappa coefficient of 0.86 (see Table 1).
Regarding the inattentive presentation, the cut-off point that best discriminated corresponded to 21 points, with a sensitivity of 92.56%, a specificity of 76.26%, a PPV of 92.01%, an NPV of 76.60%, an AUC of 0.90, and a kappa coefficient of 0.87 (see Table 1).
To evaluate the adequacy of the data set, we performed the Kaiser-Meyer-Olkin (KMO) measurement, obtaining a notable value of 0.846. The Bartlett sphericity test was also applied to assess whether factor analysis was applicable to the data set, (2) 153=2178.58, P<0.0005. Both results indicated that factor analysis was appropriate. A principal components analysis was used with the orthogonal rotation method, obtaining two factors that explain 33.44% of the variance (see Table 2).
Result of principal component analysis with two factors obtained by orthogonal Varimax rotation.
| Matrix of rotated components | |||
|---|---|---|---|
| Hyperactivity/impulsivity factor | Inattention factor | Common items | |
| Item 1 | 0.376 | 0.605 | 0.393 |
| Item 2 | 0.616 | 0.228 | 0.328 |
| Item 3 | 0.359 | 0.448 | 0.264 |
| Item 4 | 0.651 | 0.195 | 0.465 |
| Item 5 | 0.505 | 0.317 | 0.310 |
| Item 6 | 0.646 | 0.328 | 0.423 |
| Item 7 | 0.316 | 0.613 | 0.383 |
| Item 8 | 0.566 | 0.456 | 0.446 |
| Item 9 | 0.288 | 0.570 | 0.287 |
| Item 10 | 0.682 | 0.226 | 0.511 |
| Item 11 | 0.477 | 0.462 | 0.164 |
| Item 12 | 0.610 | 0.309 | 0.474 |
| Item 13 | 0.523 | 0.654 | 0.417 |
| Item 14 | 0.669 | 0.440 | 0.518 |
| Item 15 | 0.403 | 0.589 | 0.226 |
| Item 16 | 0.655 | 0.381 | 0.498 |
| Item 17 | 0.581 | 0.661 | 0.502 |
| Item 18 | 0.627 | 0.376 | 0.479 |
| % cumulative variance | 33.44 | ||
Extraction method: principle components analysis.
Rotation method: Varimax with Kaiser normalization.
The rotation converged at 5 iterations.
This study is the first to validate the ADHD Rating Scale in Spanish in the adult population, taking into account the diagnostic criteria established by the DSM-5 for ADHD. The scale had previously been validated according to DSM-IV criteria both in children18 and adults.13
Considering that the ADHD diagnosis is eminently clinical, these results provide greater precision and reliability for clinical evaluation. As this instrument is frequently used in clinical practice to determine the presence and severity of each of the symptoms of ADHD, its psychometric properties must be evaluated according to the current diagnostic criteria established by the DSM-5.
Thus, the results of this study show that the Spanish validation of ADHD-RS according to the DSM-5 has adequate psychometric properties that allow the detection of ADHD cases in the adult population.
The differentiation in the cut-off points of the scale according to the clinical presentation of ADHD allows us to detect more precisely those patients who present ADHD with a predominance of attention deficit. As these patients have a lower score on the hyperactivity/impulsivity subscales, they might not be detected if only the original cut-off point of 21 is considered.
Thus, this scale provides valuable information for clinical practice, allowing us to adequately differentiate healthy patients from those with ADHD. This also permits a timely diagnosis and proper treatment, thus avoiding the various negative consequences that an untreated diagnosis could have in adulthood.
This study presents some limitations that should be noted. The control subjects included in this study were referred to the adult ADHD Program of the Vall d’Hebron University Hospital for suspected ADHD. Therefore, the probability of presenting a higher score on this scale may be overrepresented. Secondly, for this same reason, the number of controls is lower than that of participants with ADHD. And finally, taking into account the high percentage of psychiatric comorbidity presented by adult patients with ADHD and despite finding no group differences in the present study between participants with ADHD and the control group, it would be pertinent to analyze the properties of the instrument in the different subgroups depending on the presence of comorbid disorders.
ConclusionsThis is the first validation study of the ADHD Rating Scale from English to Spanish according to the new criteria established in the DSM-5 for the diagnosis of ADHD for the adult population.
The results indicate that the cut-off point of 24 best discriminates the combined presentation and that the cut-off point of 21 best discriminates the inattentive presentation, as in the previous validation of the ADHD-RS according to the DSM-IV criteria.
Although the diagnosis of ADHD is eminently clinical, the presence of validated psychometric instruments provides higher reliability for the diagnosis of the disorder. Such instruments are very valuable at the level of clinical practice and research. The Spanish version of the ADHD Rating Scale is a valid instrument for evaluating ADHD in adults according to the diagnostic criteria established in the DSM-5.
Ethical responsibilitiesEthics statementThe study was approved by the Ethics Committee of Clinical Research of the University Hospital Ramón y Cajal. The study participants have provided written informed consent for their participation in the study.
Protection of people and animalsThe authors state that no experiments were conducted on humans or animals for this research.
Data confidentialityAll the protocols of our center were followed to maintain the confidentiality of the data. No patient data appear in this article.
Conflicts of interestDr. Aldo Pereira declares no conflicts of interest. Dr. Vanesa Richarte declares that she has given lectures or received help to attend conferences from Rubió and Shire/Takeda. Dr. Christian Fadeuilhe declares that he has given lectures or received help to attend conferences from Rubió and Shire/Takeda. Dr. Montse Corrales declares that she has received help to attend conferences from Shire/Takeda. Estela García declares no conflicts of interest. Professor Josep Antoni Ramos-Quiroga was part of the speakers’ bureau and/or acted as a consultant for Eli-Lilly, Janssen-Cilag, Novartis, Shire, Takeda, Bial, Shionogui, Lundbeck, Almirall, Braingaze, Sincrolab, Medice and Rubió in the last 5 years. He has also received help to attend conferences from Janssen-Cilag, Rubió, Shire, Takeda, Shionogui, Bial, Medice and Eli-Lilly. The Psychiatry Service that he directs has received unrestricted educational and research support from the following companies in the last 5 years: Eli-Lilly, Lundbeck, Janssen-Cilag, Actelion, Shire, Ferrer, Oryzon, Roche, Psious and Rubió.
