





Deaths by suicide (DBS) are the leading cause of death from external causes in Spain.1 Suicide prevention programmes should be evaluated periodically. The WHO highlights that improving the recording of data on DBS and self-harm attempts in the intervention population is decisive. There are tools available to learn about the characteristics of self-harm attempts in the clinical setting.2 However, there is currently no single official source of DBS in Spain; there are two alternatives; 1) consultation of the National Statistics Institute (INE), and 2) direct consultation of forensic sources in the Institutes of Legal Medicine and Forensic Sciences (IMLCF).
Several investigations detected underreporting or misclassification of DBS that could affect INE statistics and were corrected from forensic sources.3 Since 2012, the Public Health Agency of Barcelona has been reviewing the data recorded from forensic sources in all cases of death with judicial intervention in the province of Barcelona, analysing the quality of the data on the cause of death and determining improvements in mortality statistics.4
To compare the thoroughness of the registration of DBS reported by the INE before and after implementing the consultation of forensic sources in the province of Barcelona, a retrospective observational study was designed comparing the cases registered in the INE and IMLCF, before and after access to forensic sources, in the province of Barcelona, from 01.01.2005 to 31.12.2017. The annual incidence was compared over the period and the annual difference in DBS reported through both sources was calculated as rates per 100000 population for each year of the period studied. The confidence interval for mortality rates was calculated using the exact Clopper-Pearson method. The trend over time of the rates was calculated separately according to the origin of the data, using a negative binomial regression model taking time as the main variable and assessing a joinpoint in 2012. For each year, the percentage difference in rates was calculated according to the source used. The pre- and post-2012 median of these differences were calculated and compared using the non-parametric Mann-Whitney test (STATA 15.1).
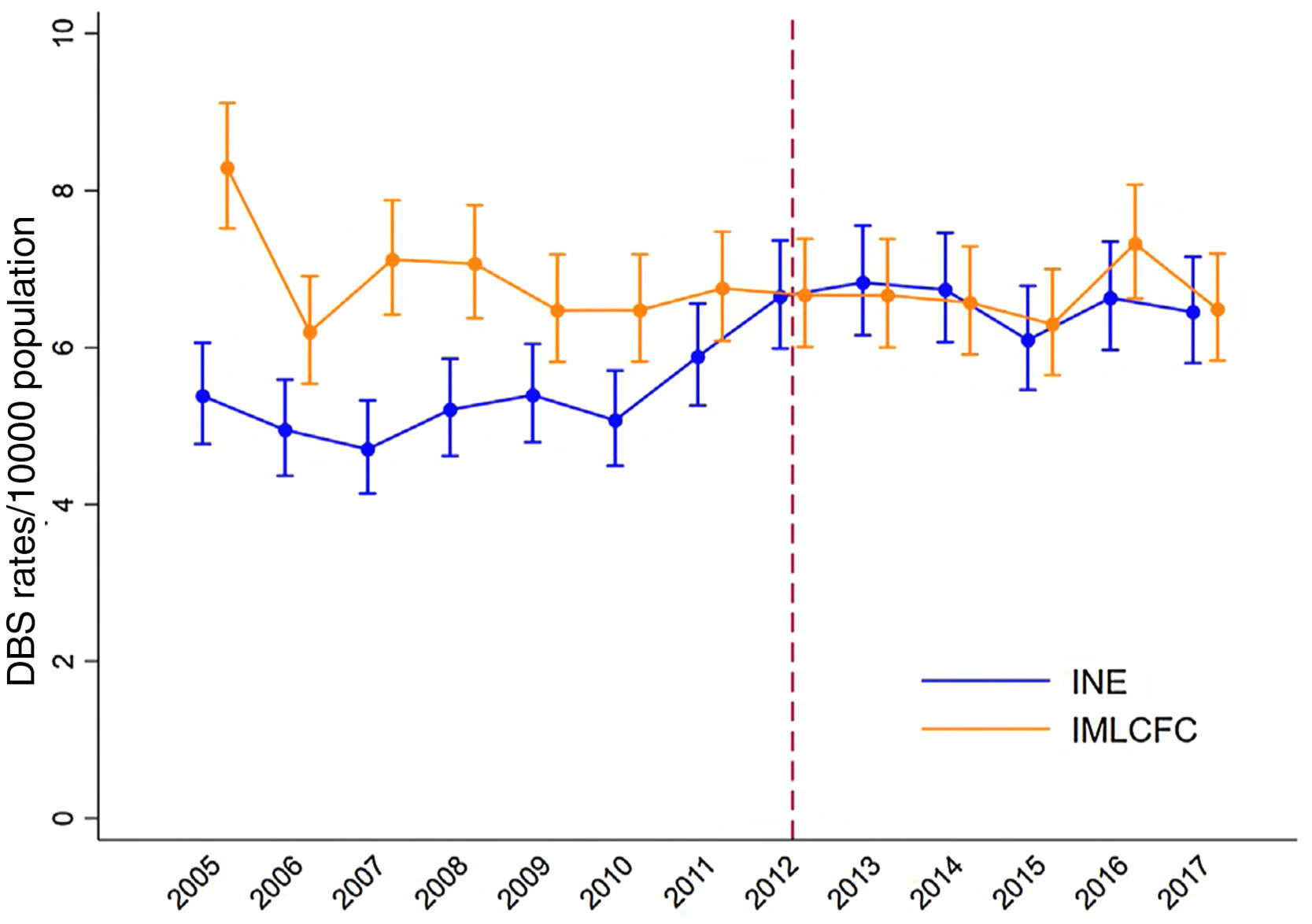
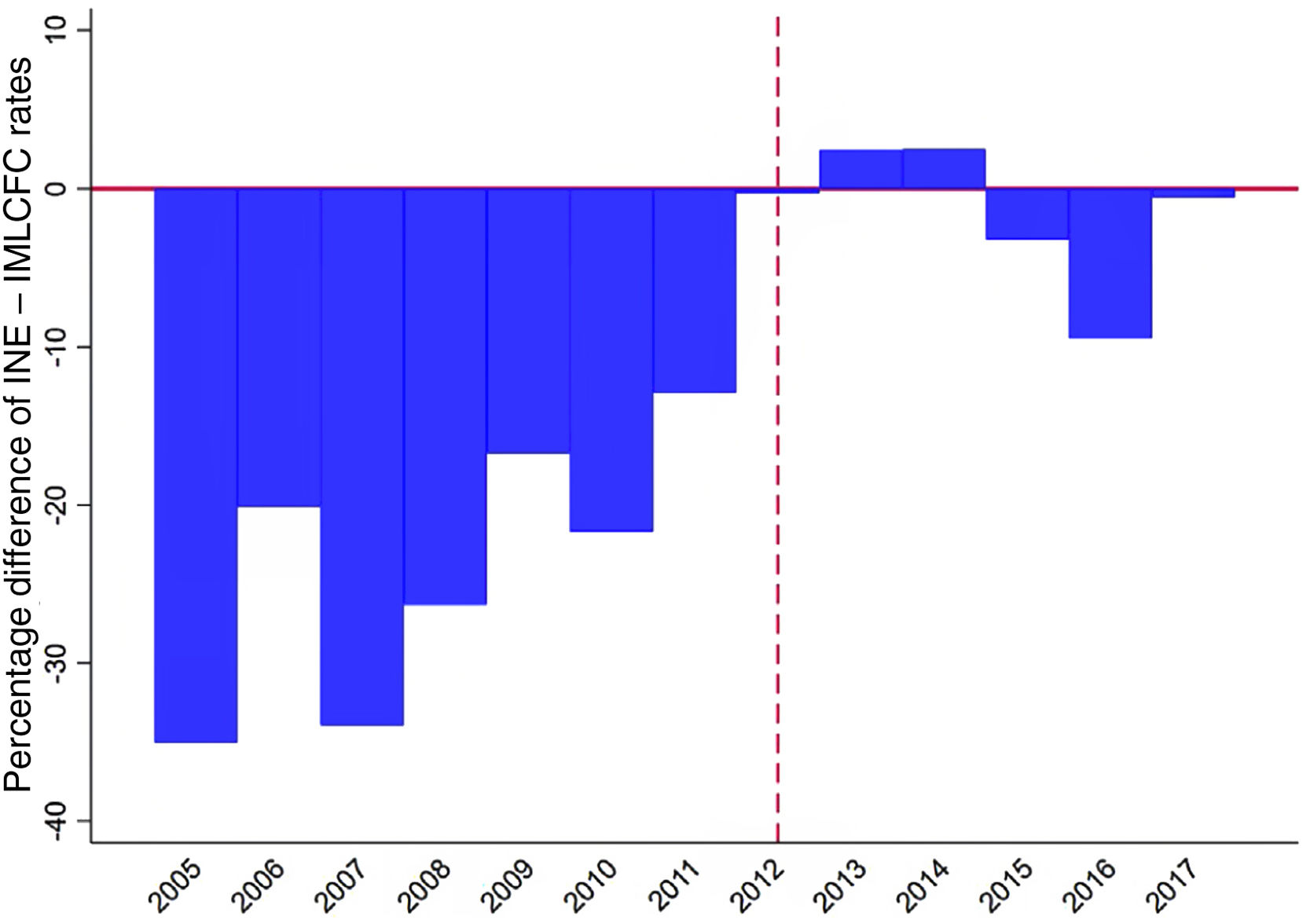
4122 MPS were identified in the INE vs. 4783 in the IMLCF. Figure 1 shows the evolution of the rates, depending on the source. For the INE, the time trend analysis of the incidence rates shows a statistically significant joinpoint (p=.002) in 2012, that is, a slightly increasing trend from the beginning of the series that ceases from 2012 onwards. In the IMLCF, no change in time trend was observed (p=.498) and the rates remained homogeneous. The median (interquartile range) of the percentage differences in the rates was -21.9 (-33.9; -16.7) before 2012 and -0.4 (-3.2; 2.4) from 2012 onwards; these differences between periods were statistically significant (p=.003) (Fig. 2).
 over the period 2005-2017, according to INE and IMLCFC data. p-value associated with the term joinpoint (change point in 2012): 0,002. DBS: deaths by suicide; IMLCFC: Institute of Legal Medicine and Forensic Sciences of Catalonia; INE: Spanish National Statistics Institute.")
Evolution of rates per 100000 population (and corresponding 95% confidence intervals) over the period 2005-2017, according to INE and IMLCFC data.
p-value associated with the term joinpoint (change point in 2012): 0,002.
DBS: deaths by suicide; IMLCFC: Institute of Legal Medicine and Forensic Sciences of Catalonia; INE: Spanish National Statistics Institute.
. Median (IQR) period 2005-2011: -21.9 (-33.9; -16.7). Median (IQR) period 2012-2017: -0.4 (-3.2; 2.4). p-value comparison of both periods: .003. DBS: deaths by suicide; IMLCFC: Institute of Legal Medicine and Forensic Sciences of Catalonia; INE: Spanish National Statistics Institute; IQR: interquartile range.")
Evolution of DBS rates in the province of Barcelona during the years 2005-2017 according to the source of registration of the data (INE or IMLCFC).
Median (IQR) period 2005-2011: -21.9 (-33.9; -16.7). Median (IQR) period 2012-2017: -0.4 (-3.2; 2.4). p-value comparison of both periods: .003.
DBS: deaths by suicide; IMLCFC: Institute of Legal Medicine and Forensic Sciences of Catalonia; INE: Spanish National Statistics Institute; IQR: interquartile range.
In line with previous research5–7 we confirm significant under-reporting of DBS through INE figures, suggesting the benefit of directly incorporating forensic data into mortality statistics from 2012 onwards. From cross-checking data with forensic sources, changes in overall DBS rates do not exceed .5% per 100000 population.
Access to forensic sources avoids underreporting of DBS and confirms the greater thoroughness of the current collection system since 2012 in Catalonia, and therefore it is worth considering extrapolating this methodology to the rest of Spain, enabling rapid access to information. The obligatory judicial autopsy on DBS, performed entirely in IMLCF, and the homogeneity in their practice8 support this access from IMLCF as an official reference register. The need for reliable real-time data on different causes of death,9 especially DBS, requires progress in direct reporting from IMLCF.10 Suicide prevention programmes, as well as any research involving the use of MPS data, should be conducted from forensic sources because they are more reliable.
