



The outbreak rapidly spread to more than 200 countries and led to millions of confirmed cases as well as thousands of deaths worldwide. This makes a serious threat to the world in terms of public health. The present study aimed to compare the COVID-19 epidemic parameters in Turkey with the top ten countries that reported the highest number of confirmed cases worldwide on April 25, 2020. Plus, it might provide better insight into the efficacy of national interventions on the course of the disease by measuring the case-fatality rate.
MethodsA detailed search of the Johns Hopkins University Center for Systems Science and Engineering official websites, and announcements were conducted between January 22 and April 25, 2020. COVID-19 related datasets for the distribution of the infection on each reported day were obtained.
ResultsAlthough the growth rate sharply increased by more than 1.2% in the late January 2020, the cumulative number of cases remained below 1500 around the world. The epidemic growth curve in Turkey was very similar to the US and Italy during the period. The case-fatality rate in Turkey was 2.51%, which below the countries with the most cases, except Russia, and the recovery–death ratio appeared to be at a moderate level among these countries.
ConclusionsSince there are no standard treatments for the disease, it is important to avoid infection or further spreading. Decision-makers should adopt a series of measures to mitigate the impact of the pandemic, using national surveillance systems.
El brote se extendió rápidamente a más de 200 países y provocó millones de casos confirmados y miles de muertes en todo el mundo. Esto representa una seria amenaza para el mundo en términos de salud pública. El presente estudio tuvo como objetivo comparar los parámetros de la epidemia de COVID-19 en Turquía con los diez principales países que informaron el mayor número de casos confirmados en todo el mundo el 25 de abril de 2020. Además, podría proporcionar una mejor comprensión del papel de las medidas nacionales en el curso de la enfermedad mediante el cálculo de la tasa de letalidad.
MétodosSe realizó una búsqueda detallada de los sitios web oficiales del Centro de Ciencias e Ingeniería de Sistemas de la Universidad Johns Hopkins, y se realizaron anuncios entre el 22 de enero y el 25 de abril de 2020. Se obtuvieron los datos relevantes de la distribución de la infección en cada día informado.
ResultadosAunque la tasa de crecimiento aumentó bruscamente en más del 1,2% a fines de enero de 2020, el número acumulado de casos se mantuvo por debajo de los 1.500 en todo el mundo. La curva de crecimiento epidémico en Turquía fue muy similar a la de Estados Unidos e Italia durante el período. La tasa de letalidad en Turquía fue del 2,51%, que está por debajo de los países con la mayoría de los casos, excepto Rusia, y la tasa de recuperación y mortalidad parecía estar en un nivel moderado entre estos países.
ConclusionesDebido a que no existen tratamientos estándar para la enfermedad, es importante evitar la infección o una mayor propagación. Los tomadores de decisiones deben adoptar una serie de medidas para mitigar el impacto de la pandemia, utilizando sistemas de vigilancia nacionales.
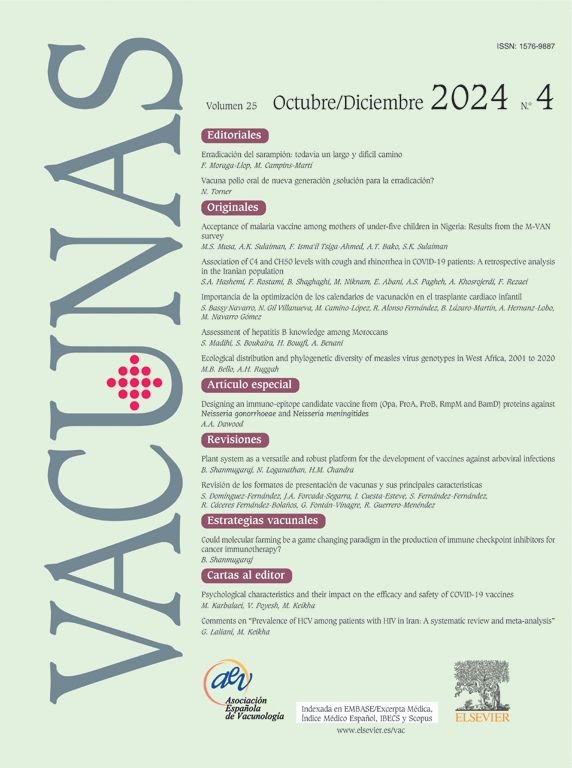
The outbreak of coronavirus disease (COVID-19), which was first reported in Wuhan, China, in late 2019, quickly spread to more than 200 countries as the number of cases rises daily, as of April 25, 2020 (Fig. 1).1 Besides mainland China, multiple countries are now facing the COVID-19 pandemic, which is a significant threat to public health. Moreover, since the last of February 2020, the rate of increase in confirmed cases has become higher in the rest of the world than inside the Mainland of China.2,3 As of April 25, 2020, a total of 2,719,897 confirmed cases and 187,705 deaths due to the COVID-19 disease were reported worldwide, of which 84,325 cases and 4642 deaths were in the Mainland of China.4 In response to the outbreak, national governments have introduced different interventions and these approaches have affected the severity of the disease in different ways, with various implications. China, for example, has reached a plateau level with strict measures, such as building an emergency hospital in days5 and rapid testing protocols.6 However, the rate of the confirmed cases in the United States has continued to increase, with almost ten times more deaths than in the Mainland of China.4

In order to measure the severity of the disease that causes death, several studies have discussed the case-fatality rate (CFR) during a specified time period by country.7–9 A widely used definition of the CFR is “a measure of disease severity and is defined as the proportion of patients with a specified disease or condition who die within a specified time.”10 This definition acknowledges that the CFR is dependent of time of observation for a disease. In other words, the time periods for the numerator and the denominator do not need to be the same.11 For example, the denominator could be cases of COVID-19 diagnosed on April 2020, whereas the numerator, deaths diagnosed with COVID-19 in the same time period, could be from April 2020 to the present. Therefore, in the study, the data on case-fatality is based on defining COVID-19 related deaths that confirmed positive test results, independently from pre-existing diseases that may have caused death. In fact, this measurement can give insight into the prognosis of the outbreak and the efficacy of public health-related interventions.12 The CFR has a crucial role in managing strategies at national and international levels in terms of public health.9 High the CFR states not only a limitation to access to proper health care for the most vulnerable people but also insufficiencies in healthcare systems, including the limited capacity of the surveillance system to trigger a timely response.13 In this regard, to examine the CFR for countries with the most confirmed COVID-19 cases, such as Turkey and Italy, may provide a viewpoint on the potential influence of the disease on public health.
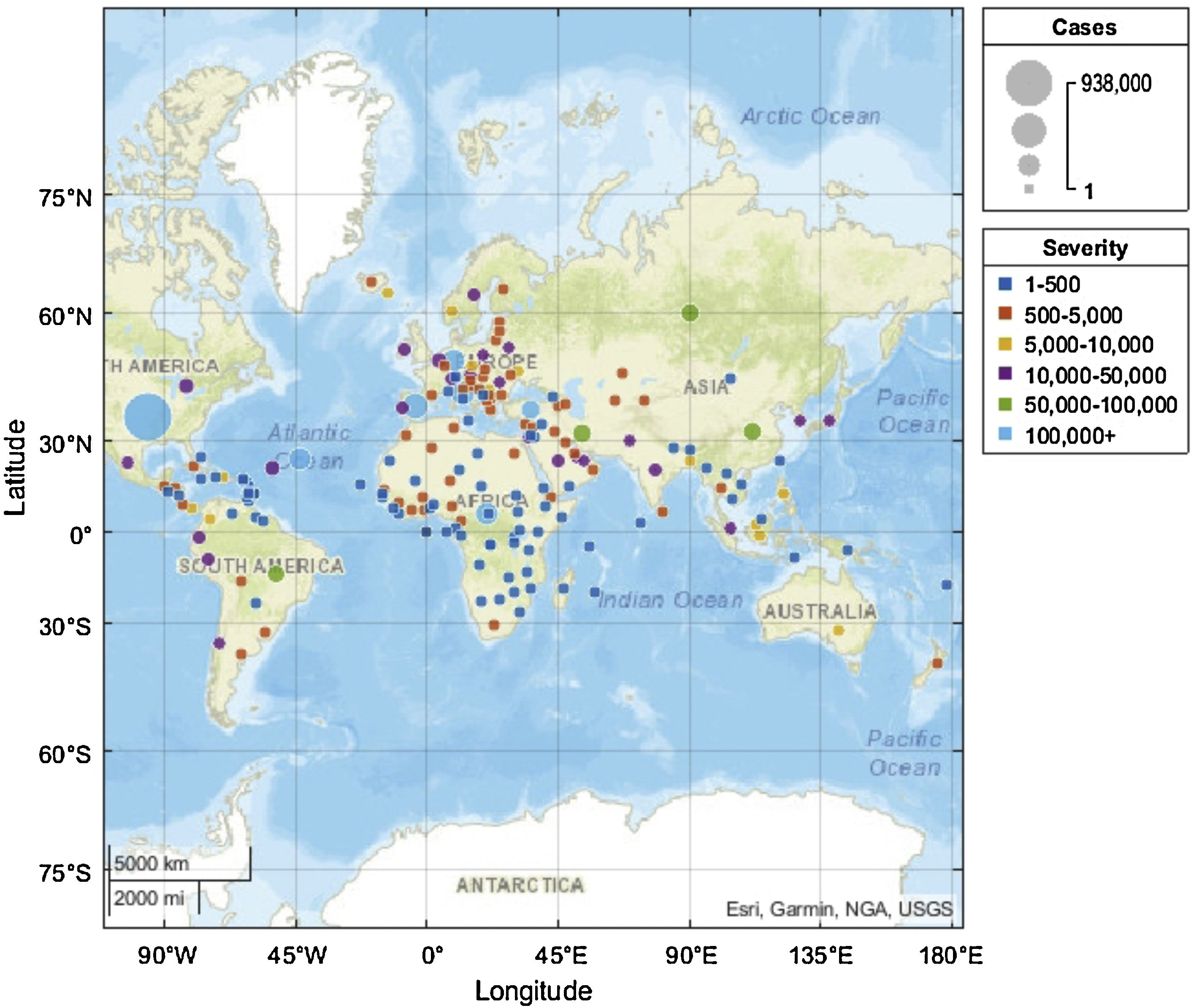
Since the beginning of February 2020, various public health interventions have been implemented across Turkey to control the spread of the COVID-19 disease (Fig. 2). However, the first confirmed case was reported on March 11, 2020.14 After a month of the first reported case, Turkey placed in the top 10 countries with the most confirmed cases. The progression of the COVID-19 epidemic reached the point of more than 100,000 cases and 2600 deaths, as of April 25, 2020. Assessing the epidemic features of the COVID-19 in Turkey and other countries is crucial to determine the changes during the outbreak progression and to enable strategic planning for decision-makers need as epidemics unfold. Therefore, this study, firstly, aimed to compare the COVID-19 epidemic trends in Turkey with the top ten countries that reported the highest number of confirmed cases around the world on April 25, 2020.4 Secondly, it might provide better insight into the role of national measures on the course of the disease by measuring the CFR.
Material and methodsStudy design and data collection
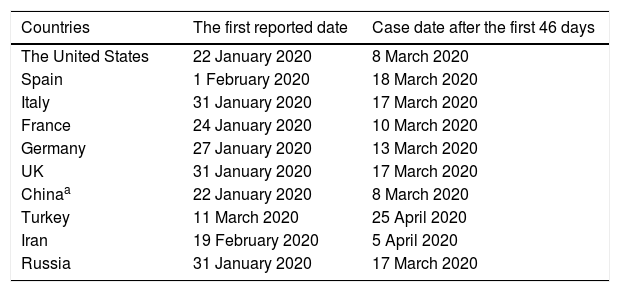
As of April 25, 2020, the top 10 countries with the most reported COVID-19 cases were the United States (US), Spain, Italy, France, Germany, the United Kingdom (UK), Turkey, Iran, China, and Russia, respectively. The relevant data on the distribution of disease for all these countries were included. In order to build a reliable comparison during the same period, firstly, the date of the first reported confirmed case of the COVID-19 was identified for these countries. Finally, the first 46-day disease-related data set for each country were included in the study. The 46-day period was selected because the first confirmed case was reported on March 11, 2020, in Turkey (Table 1).
Reported confirmed case date for the study.15
| Countries | The first reported date | Case date after the first 46 days |
|---|---|---|
| The United States | 22 January 2020 | 8 March 2020 |
| Spain | 1 February 2020 | 18 March 2020 |
| Italy | 31 January 2020 | 17 March 2020 |
| France | 24 January 2020 | 10 March 2020 |
| Germany | 27 January 2020 | 13 March 2020 |
| UK | 31 January 2020 | 17 March 2020 |
| Chinaa | 22 January 2020 | 8 March 2020 |
| Turkey | 11 March 2020 | 25 April 2020 |
| Iran | 19 February 2020 | 5 April 2020 |
| Russia | 31 January 2020 | 17 March 2020 |
Although a new coronavirus was identified by the Chinese Center for Disease Control and Prevention on January 7, 2020,30 the first cumulative data on confirmed cases for China in the dataset processed on January 22, 2020.
The data from this study were collected from open access COVID-19 epidemiological data source is compiled by the Johns Hopkins University Center for Systems Science and Engineering (JHU CCSE) from multiple sources including the World Health Organization (WHO) and the China Center for Disease Control and Prevention (CCDC).15,16
The case-fatality rate was measured in a specific time period according to the standard formula:

The growth rate formula was used as follow:

In the growth rate formula, it is subtracted the prior value, which is the number of reported cases yesterday, from the current value, which is the number of reported cases today. Then, it is divided that number by the prior value.
Data analysisCollected data were performed with the Statistical Package for Social Sciences version 26.0 (SPSS 26.0; SPSS Inc., Chicago, IL, USA) and the Prism statistical software package version 8.4 (Graphpad Software Inc. La Jolla, CA, USA). To visualize the data on the COVID-19 (Figs. 1 and 3), MATLAB v.R2020a (Natick, Massachusetts: The MathWorks Inc., USA) was used. For statistical analysis, continuous variables consisted of daily reported new confirmed cases, total confirmed cases, accumulated deaths, and recovered cases. With these data set, descriptive data analyses were performed in the study. Descriptive statistics were defined and compared. Measurement data were described as a percentage.
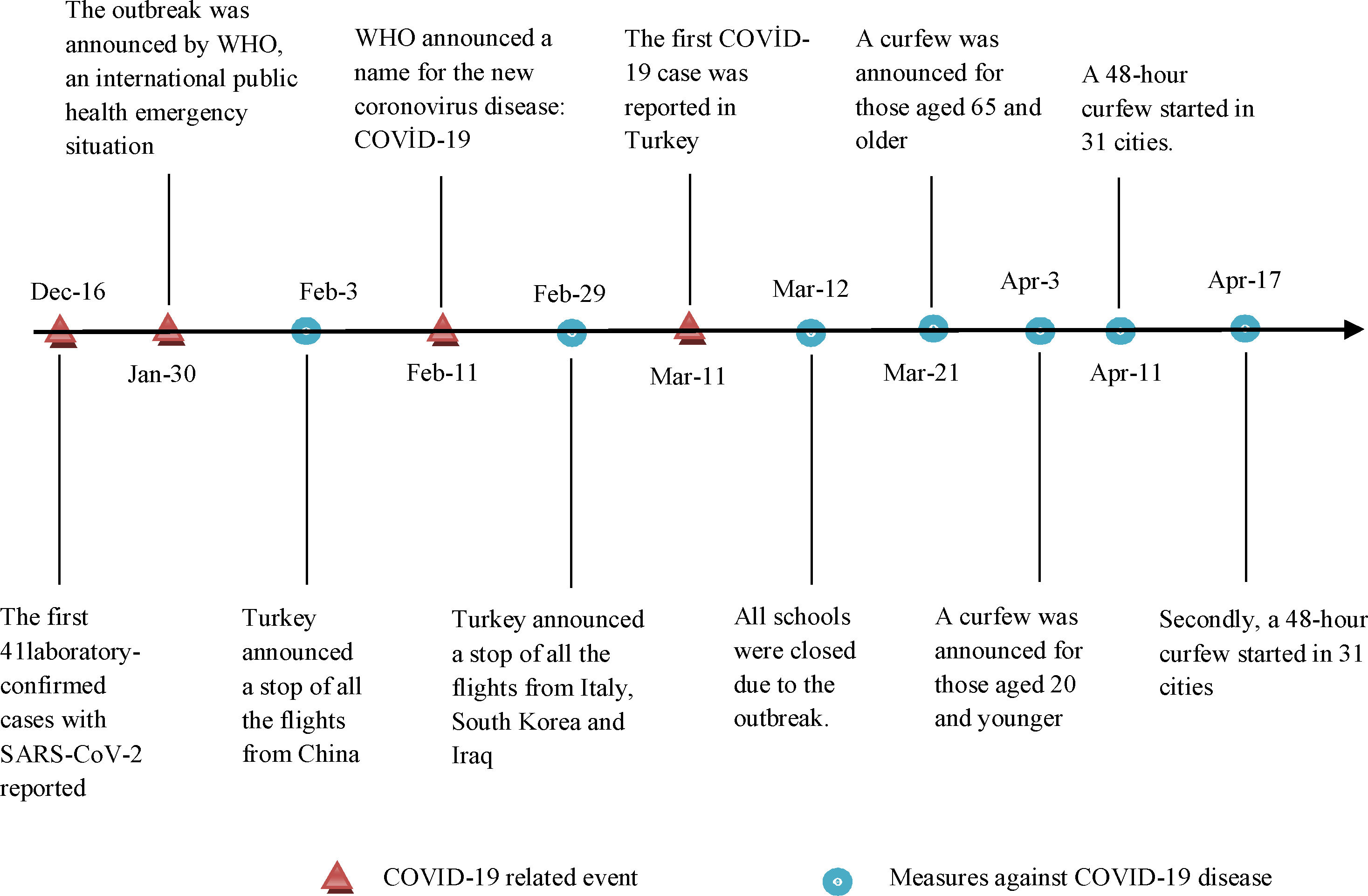
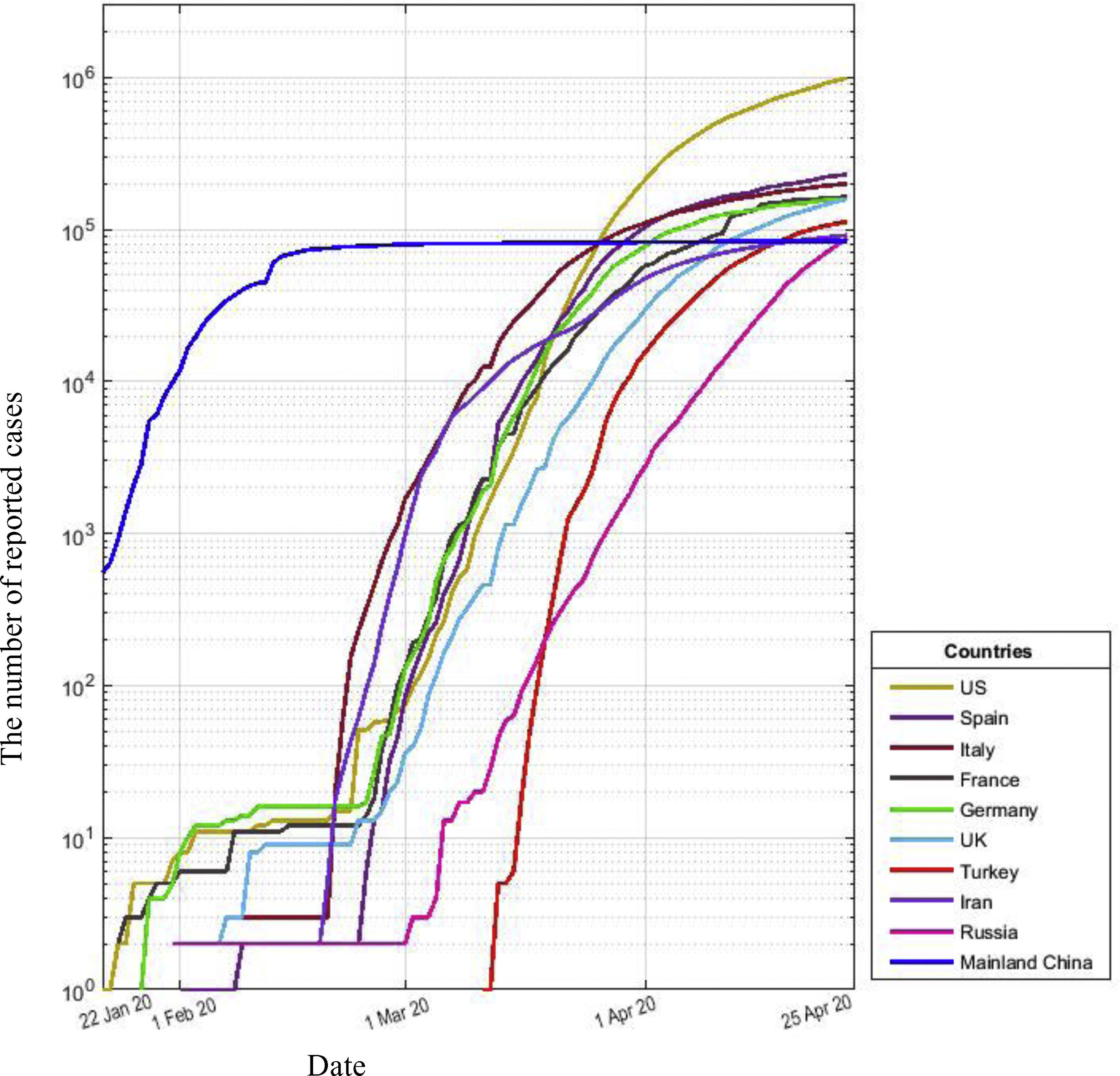
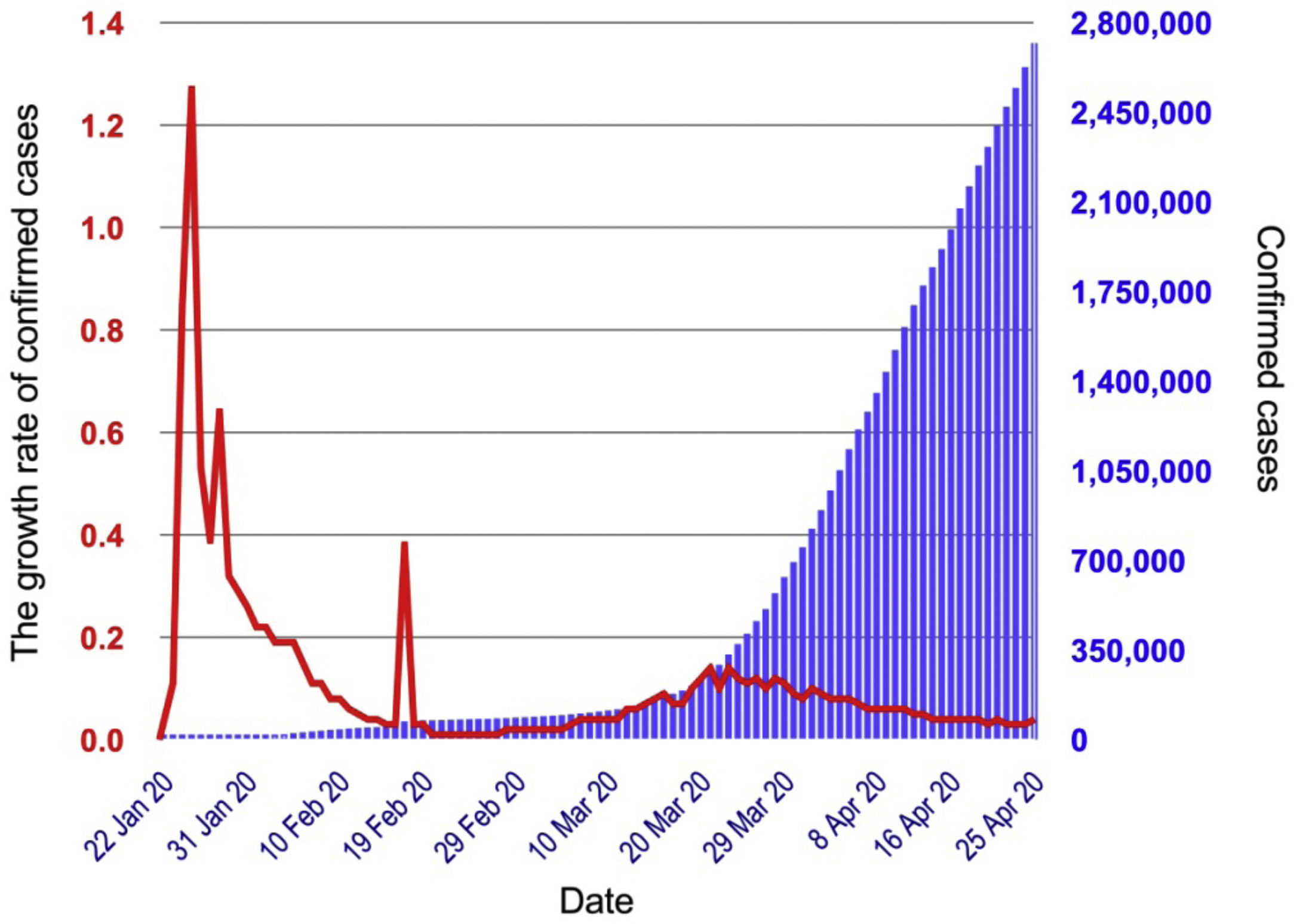
ResultsSince the outbreak of the coronavirus disease in December 2019, in the Mainland of China, it has quickly spread around the world. Although WHO declared the outbreak a Public Health Emergency of International Concern on January 30, 2020,17 the number of confirmed cases have already been reported in many countries, such as the United States, France, and Germany. By April 25, 2020, the total number of confirmed cases in the United States had reached almost 1 million, with the most reported cases worldwide (Fig. 3). As can be seen in Fig. 4, the growth rate sharply increased by more than 1.2% in the late of January 2020, whereas the cumulative number of cases remained below 1500 around the world (Fig. 4). Moreover, this rate continued to decline significantly until about the middle of February, and then sharply rose to 0.4% (nearly) in the same period. The most striking aspect of Fig. 4 is that the growth rate decreases as the number of confirmed cases increase between January, 22 and April 25, 2020.

Fig. 3 compared the course of confirmed cases by the top ten countries between January 22, 2020 and April 25, 2020 during the outbreak. The number of these cases, for the first time, started to plateau in the middle of February, though countries continued to report thousands of infections every day. Closer inspection of Fig. 3 showed an exponential increase did not take a long time in Turkey until the end of April 2020 compared to the other countries. Moreover, the epidemic growth curve in Turkey was very similar to the US and Italy; however, the national number of cases was different. Almost all countries in Fig. 3, except China and Turkey, growth curves followed a steep staircase with many confirmed cases until the beginning of March 2020.

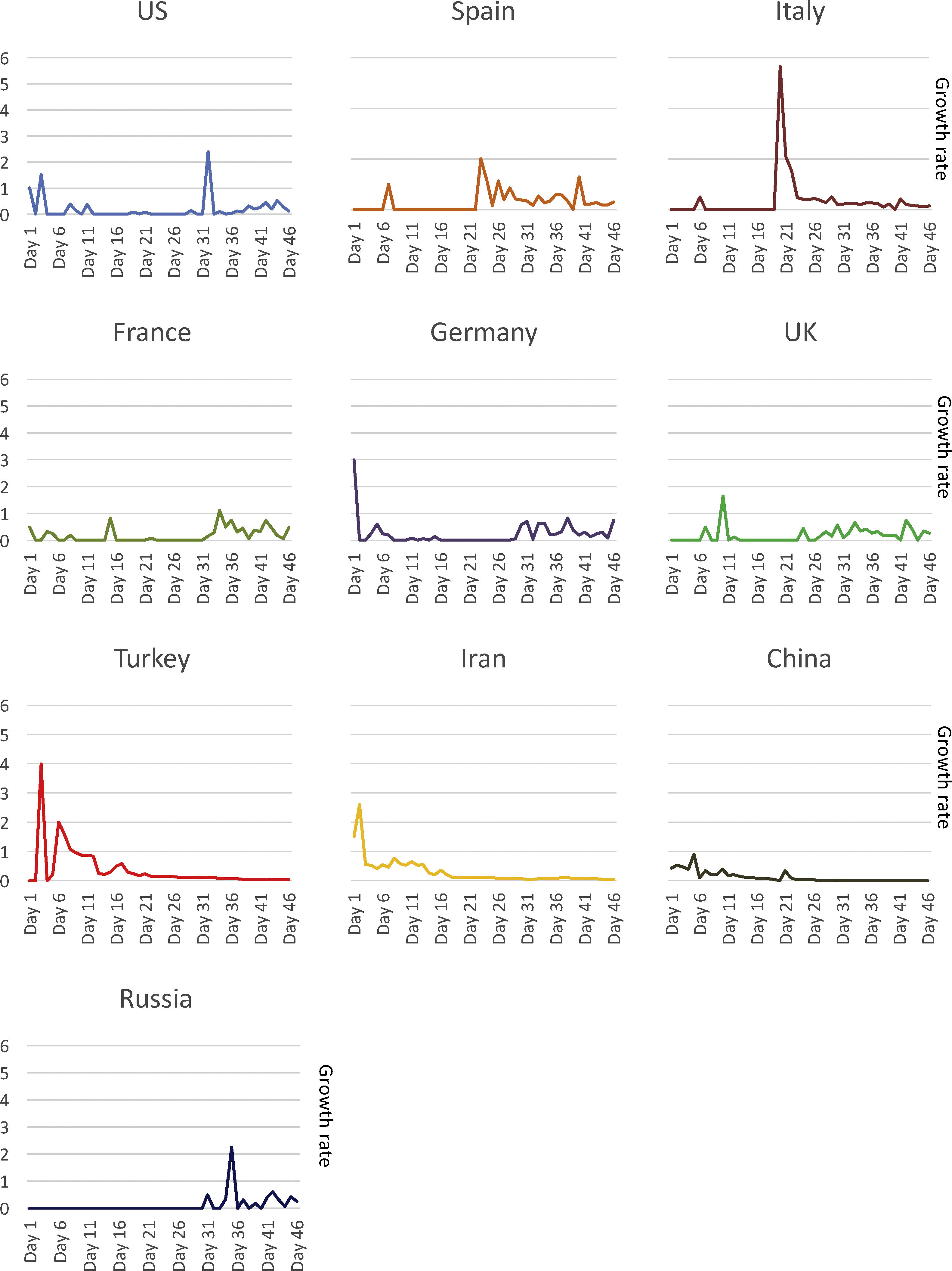
A comparison of the growth rate of confirmed cases for the first 46-day period in Turkey and other countries with the most cases around the world was presented in Fig. 5. Compared to other countries, the growth rate of the confirmed cases in Turkey suddenly increased to 4% at the beginning of the first 46-day period and then gradually decreased to below 1% by the middle of the period. In Italy, on the other hand, this rate jumped to close to 6% in the middle of the first 46-day period. Germany showed a rate of more than 3% at the beginning of the period and followed the line below 1% in the rest of the 46-day period. Among these ten countries with the most confirmed cases, the growth rate in China remained below 1% with the lowest level during the same time period.

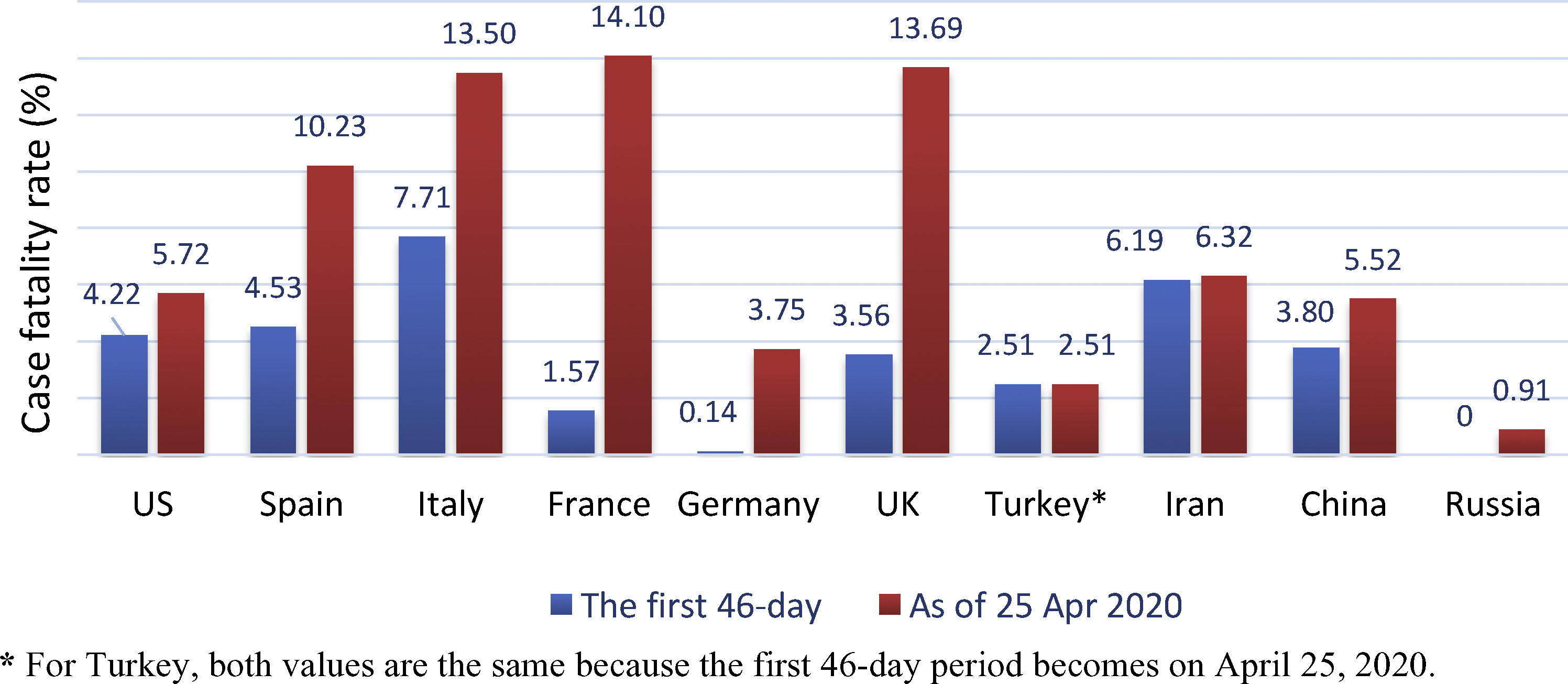
Fig. 6 showed the results of the CFR comparison by country between two different time points, first 46-day and April 25, 2020. It was apparent from this figure that almost all countries had a higher CFR than the first 46-day period. It was striking that Italy, France, and the United Kingdom had nearly the same rate. Although there were significant differences between the two time periods (the first 46-day and April 25, 2020) for many countries, case-fatality rates of Iran were slightly different, with 6.19% and 6.32%, respectively. The overall case-fatality rate in the United States (5.72%), having the most cases worldwide (Fig. 3), was substantially lower than in France (14.10%).

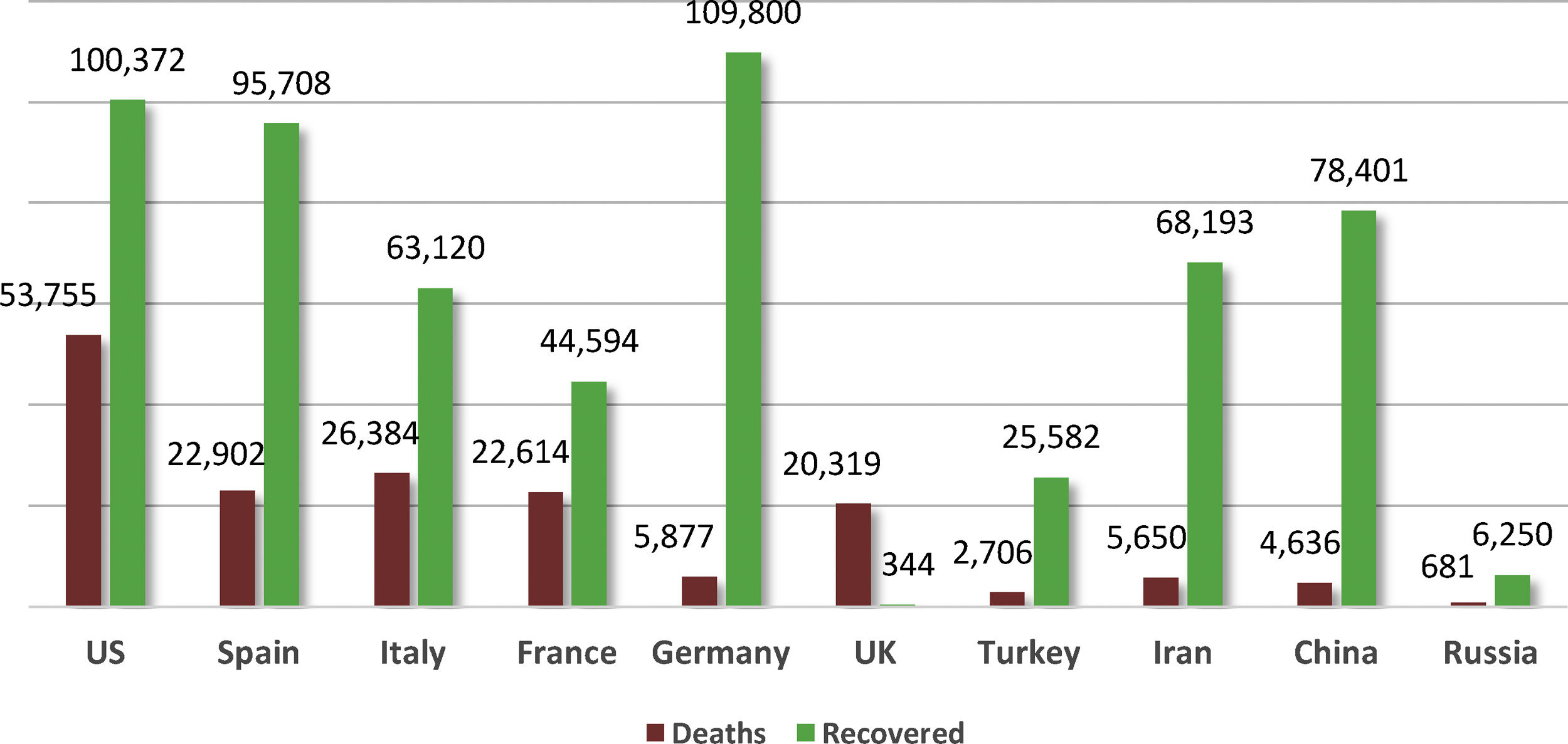
As shown in Figs. 7 and 3, the United States had not only the most confirmed cases but also total death numbers worldwide. What was striking about the data in Fig. 7 was that the number of recovered cases in Germany was higher than any in other country, whereas the number of confirmed deaths was higher than in Iran, China, Russia, and Turkey. Interestingly, the number of recovered patients in the UK was quite low compared to other countries on April 25, 2020.
Discussion.")
In late 2019, the outbreak emerged in Wuhan, China and then quickly spread to many countries. In response to the global spread of the novel coronavirus disease, many preventive measures have been implemented around the world. In order to assess the progression of the outbreak and the effect of public health measures under various facts, it could be useful to examine the infection parameters globally. This study set out with the aim of examining the epidemic variables in ten countries with infection disease compared with Turkey.
The COVID-19 outbreak is characterized as a pandemic because of spreading easily from person-to-person.18 In this case, public health officials rely on indicators of the epidemic growth rate to assess the risk of observing a major outbreak.19 The growth dynamics in the early period of the epidemic could vary substantially. However, during the first period, especially on January 2020, the cumulative number of COVID-19 cases globally followed a sharp increase, likely as a result of the outbreak management policy of the government. These dynamics should be taken into account when making inferences on the epidemic growth rate. In Turkey, for example, the possible reason why the growth rate of the outbreak in the first several weeks was a higher percentage could be the inadequate effective preventive measures against the coronavirus epidemic. Because as physical distancing measures, including school closures and strict social interventions, were implemented, the growth rate decreased gradually.
Although fluctuations in the growth rate in Turkey continued to the middle of the period, other countries like the US, France, the UK, and Spain showed a dramatic fluctuation during the first 46-day period. Moreover, the number of confirmed cases in these countries was higher than in other countries on April 25, 2020. Based on these trends, it is possible to assume that the specific measures adopted by the governments to reduce and mitigate the spread of the outbreak are inadequate or ineffective. Because some of those strict measures against the outbreak help to decline the number of confirmed cases and the growth rate of confirmed cases during the period.20
According to the data from Fig. 6, the overall case-fatality rate for countries, except Turkey, was lower and ranged from 0% (Russia) to 7.71% (Italy) in the first 46-day period compared to on April 25, 2020, ranging from 0.91% (Russia) to 14.10% (France). This may be because of the following factors. (1) The lack of disease awareness and inappropriate prevention and control may lead to a higher epidemic of infections on April 2020. This fact was experienced in the Mainland of China and its regions.21 (2) A significant number of asymptomatic or mild individuals cannot be identified.22 (3) Because of the lack of available laboratory testing, patients with the disease cannot be determined, particularly in the first period of the infection.23 (4) Because of the possible risk factors, including age and comorbidity, affecting the progression of disease in COVID-19 patients, delayed treatment and inadequate medical supplies can lead to higher mortality rates in the early days of the epidemic.24 According to the report from WHO, although the scale of asymptomatic or subclinical infections is unclear, they seem to be relatively rare. Furthermore, they do not appear to be the main factor of transmission.25
Even though there were more than 107,000 cases in Turkey, the CFR was 2.51% on April 25, 2020, which below the countries with the most cases, except Russia. Initially, with no more data on the number of cases and deaths, the CFR emerged as a ratio between 1% and 2.40% in the first week of fatalities from the outbreak in Turkey. In the same period, the rate reported outside of China on March 23, 2020 was even higher (4.45%). In the last week of April, the CFR increased to 2.52% and 7.04% in Turkey and outside of China, respectively.26 This pattern of increasing CFRs is not surprising because as the number of cases ascended around the world, the possibility of death in cases with COVID-19 intensified during the outbreak. It is worth noting that the CFR is likely increased in some countries in case of a surge of patients infected with the coronavirus, which adds to the burden on the health system and strain its sustainable medical resources. Despite highly transmissible, the infection mostly affected older adults and people having severe underlying medical conditions like diabetes.27 Hence, further research could be helpful to understand more precisely what the relationship is between the CFR and age groups in countries.
Since the first confirmed case in China on December 2019, nearly 3 million cumulative confirmed cases and more than 187 thousand deaths from the outbreak have been reported worldwide. However, the overall number of recovered cases has significantly begun to exceed the number of deaths worldwide since the beginning of February 2020.26 This trend emerged with 214 deaths and 243 recovered in Turkey, for the first time, on the 20th day after the first reported case. However, the United States, Spain, and Italy caught this trend at different times during the outbreak, with on 68th day, 36th day, and 28th day, respectively. It is important to stress that Germany has significantly higher the recovery–death ratio compared to other countries, including Turkey. This ratio in Turkey seems to be at a moderate level among these countries. On the other hand, for the UK, this fact appears dramatically low. Overall, it can be partly concluded from this trend that a high level of testing capacity for a broad sample of the population, early public health measures for the outbreak and a strong health care system to care for people with COVID-19 at high risk can be a crucial factor for underlying the results.
Finally, these results need to be interpreted with caution because of some possible reasons. First, the number of confirmed cases of infection is just based on data with laboratory confirmation for many countries, including Turkey. Especially, asymptomatic cases or patients called asymptomatic carrier or transmitter with very mild symptoms might not be identified.28 While some cases might be fully asymptomatic, not showing any symptoms yet, others can be presymptomatic, people become infectious before feeling sick. Some studies have estimated that people without symptoms (whether truly asymptomatic or presymptomatic) could be responsible for up to half of the spread.24,28 This might be the disease so difficult to contain. A study recently reported that more than 40% of secondary cases were infected during the presymptomatic stage.29 Hence, there are likely to have unreported cases in countries. Second, patients have typical signs and symptoms COVID-19 (fever, dry cough, fatigue, sputum production, shortness of breath, sore throat, headache, nasal congestion, and myalgia or arthralgia),25 although they have a negative result of COVID-19 nucleic acid testing. Such misdiagnosed cases, therefore, cannot be included in the cumulative case rates, since actual cases pertain to positive nucleic acid test (PCR) result, not the chest computed tomography (CT) imaging and other clinical symptoms of COVID-19. Finally, different surveillance and response systems in countries for monitoring risk factors might also be a potential impact on the number of cases being reported.
ConclusionsThe purpose of the present study was to examine the epidemic characteristics of COVID-19 in the countries with the most cases and to compare the epidemiological features with Turkey in the specific time period between January 22 and April 25, 2020. The findings indicate that the epidemic outbreak of COVID-19 was rapidly spread worldwide and the growth rate of confirmed cases in these ten countries rose to nearly 6% during this period. It is likely that the risk of healthcare system capacity and protecting the most vulnerable population groups may be considered high if the number of cases continued to increase in countries. In this regard, since there is no definitive treatment for COVID-19, it is essential to avoid infection or further spreading. In particular, decision-makers should adopt a series of measures to mitigate the impact of the pandemic, using national surveillance systems.
Ethical issuesNot necessary.
Conflict of interestI declare that I have no competing interests in this study.