





RECALSEEN project aims to analyze the structure, activity, and outcomes of the departments of endocrinology and nutrition (S-U_EyN) of the Spanish National Health System (SNHS). Based on the results obtained, the challenges for the specialty are analyzed and proposals for improvement policies are made. In this paper 2021 survey data and activity data from the 2007–2019 from the Minimum Basic Data Set (MBDS) are presented.
Material and methodsCross-sectional descriptive study of the S-U_EyN of acute general hospitals of the NHS in 2020. Data were obtained through: 1. an "ad hoc" survey answered by the S-U_EyN’ consultants; and 2. analysing the acute general hospital discharges from S-U_EyN and discharges with endocrine-metabolic comorbidities registered in the minimum basis data set (MBDS) of the SNHS.
Results112 responses from S-U_EyN were obtained from a total of 154 general acute hospitals of the NHS (73%). The 2021 S-U_EyN sample includes 24 more centers than in 2017. 54% of the S-U_EyN were endocrinology departments. The median number of endocrinologists per S-U_EyN was 7. The estimated rate of endocrinologists was 2.5 per 100,000 inhabitants. S-U_EyN showed a high level of collaboration with primary care teams and other hospital units. Use of telemedicine by S-U_EyN experienced a high increase in 2020. Notable differences in resources and activity have been found between hospitals and Autonomous Communities. There was a wide margin for improvement in quality management.
ConclusionsRECALSEEN is a useful project for the analysis of S-U_EyN. The remarkable variability found in the indicators of structure, activity and management probably indicates a wide margin for improvement.
RECALSEEN tiene por objetivo analizar la estructura, actividad y resultados de los Servicios y Unidades de Endocrinología y Nutrición (S-U_EyN) del Sistema Nacional de Salud español (SNS), así como, a partir de los resultados obtenidos, analizar los retos para la especialidad y realizar propuestas de políticas de mejora. En este artículo se presentan los datos de la encuesta de 2021 y datos de actividad procedentes del Conjunto Mínimo Básico de Datos (CMBD) de 2007–2019.
Material y métodosEstudio descriptivo transversal de los S-U_EyN en hospitales generales de agudos del SNS en 2020. Se han utilizado datos obtenidos mediante RECALSEEN 2021, una encuesta “ad hoc” y de las altas dadas por los S-U_EyN registradas en el conjunto mínimo de datos (CMBD) del SNS (2019). La encuesta ha recogido datos de actividad de 2019 y 2020.
ResultadosSe obtuvieron 112 respuestas de S-U_EyN sobre un total de 154 hospitales generales de agudos del SNS (73%). La muestra de S-U_EyN incluyó 24 centros más que en 2017. El 54% de los S-U_EyN que respondieron eran servicios o unidades de gestión clínica. La mediana de endocrinólogos por S-U_EyN fue de 7, siendo la tasa estimada de endocrinólogos por cada 100.000 habitantes de 2,5. Los S-U_EyN tienen un elevado nivel de colaboración con unidades de atención primaria y hospitalarias. En 2020 se produjo un importante desarrollo de la telemedicina. Se encontraron notables diferencias en recursos y actividad entre centros y Comunidades Autónomas. En relación con la gestión de la calidad e implantación de buenas prácticas seguía existiendo un amplio margen de mejora.
ConclusionesRECALSEEN es un proyecto que ofrece información relevante sobre los S-U_EyN. La notable variabilidad hallada en los indicadores de estructura, actividad y gestión probablemente indica un amplio margen de mejora.
RECALSEEN is a Sociedad Española de Endocrinología y Nutrición [Spanish Society of Endocrinology and Nutrition] (SEEN) project that began in 2017 in the context of envisioning significant challenges arising from the increasing prevalence of health problems typical of the specialty and the progressive technification of diagnostic and therapeutic processes,1–3 framed within the SEEN’s commitment to professionalism.4,5 The need to provide information on the resources, activity and quality of endocrinology and nutrition services and units (S-U_EyN) in order to make health policy proposals based on data has become even more evident as a result of the effects that the SARS-CoV-2 pandemic has had on the functioning of health services, including the need for their transformation and the impetus for “digitisation” of health.6,7 The RECALSEEN project, developed by the SEEN with the collaboration of the IMAS (Instituto para la mejora de la asistencia sanitaria [Institute for Health Care Improvement]) Foundation, aims to: (1) Gain information on healthcare in the S-U_EyN for endocrinology diseases and nutritional disorders; and (2) Develop proposals to improve the quality and efficiency of care for these conditions. The RECALSEEN project has two main sources of information: the RECALSEEN survey and the Spanish National Health System (SNHS) Minimum Basic Data Set (MBDS) database.
The RECALSEEN survey in 2017 received responses from 88 S-U_EyN hospitals with 600 ± 360 beds (median 500) and a population coverage of 58%. The most relevant conclusions included: predominantly outpatient activity of the S-U_EyN (consultation, interconsultation and day hospital); integration of nutrition units in the S-U_EyN, but with low staffing provision; progressive development of specialist units; greater participation of the S-U_EyN in multidisciplinary units, as well as the significant variability found in the indicators of structure, activity and management of the S-U_EyN.1
The aim of this article is to present the most relevant results obtained in 2021, as well as to analyse changes and progress since 2017. Finally, we suggest changes that the S-U_EyN should consider in order to offer an appropriate response to the challenges identified by the findings of the RECALSEEN project.3
Material and methodsThis was a descriptive, cross-sectional study conducted with the S-U_EyN of the SNHS. The universe included S-U_EyN located in general acute care hospitals with 200 or more beds, whilst, as in 2017, surveys of S-U_EyN from hospitals with fewer than 200 beds were also included. The questionnaire used for data collection is shown in Appendix B additional material (Table 1, annex). The registration data were self-managed online by those responsible for the S-U_EyN. The management and debugging of the questionnaire have been described in other publications.1,8 The data collected through the survey referred to the year 2020, except for activity for which data were requested for the years 2019 and 2020. The survey opened on 1 May and closed on 1 October 2021. The MBDS data correspond to the period 2007–2019.
Statistical analysisThe qualitative variables are described with frequency distribution (number of cases and percentages) and the quantitative variables with the mean, median, standard deviation (SD) and interquartile range (IQR). The Chi-squared test was used to compare qualitative variables, and the Student's t-test to compare quantitative variables. Trend analyses were performed using Poisson regression. All comparisons rejected the null hypothesis with an alpha error <0.05. Statistical analyses were performed with STATA version 17.0.
ResultsOut of a total of 154 general acute care hospitals of the SNHS, there were 112 responses (73%) from S-U_EyN (24 S-U_EyN more than in 2017). Nine S-U_EyN were from centres with fewer than 200 beds and one from a private hospital. One centre was exclusively paediatric. The number of beds in the hospitals where the S-U_EyN were located was 555 ± 297, not statistically different from the 2017 survey (602 ± 361; p = 0.332). All the data from the S-U_EyN that responded to the RECALSEEN survey were considered for the analyses. The distribution of responses by autonomous community is shown in Appendix B, Table 2 of the additional material (annex). The estimated population of the catchment areas of the S-U_EyN that responded to the survey represented 76% of the total Spanish population as of 1 July 2020 (INE [Instituto Nacional de Estadística (Spanish National Institute of Statistics)]). Fifty-seven (51%) of the S-U_EyN that responded were from hospitals with 500 or more beds.
Structure and resourcesIn total, 54% of the S-U_EyN that completed the survey were clinical management units or services, and 36%, sections. The Nutrition unit was integrated into the S-U_EyN in 89% of cases. The median number of affiliated endocrinologists was seven (mean: 8.1 ± 4.7). The rate of endocrinologists estimated by the survey was 2.5 per 100,000 inhabitants in the SNHS.
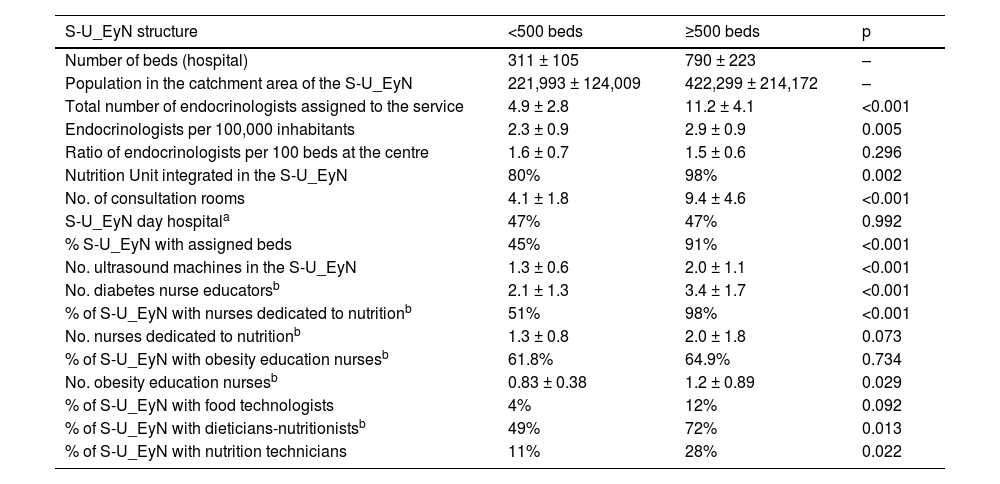
The S-U_EyN had 4.5 nurses (median; average: 5.4 ± 3.3) assigned to the service (including those assigned to functional tests and excluding hospitalisation); two nurses (median; mean: 2.8 ± 1.7) assigned to diabetes education; 73% of the S-U_EyN had nurses assigned to nutrition (median: 1.3); 63% of the S-U_EyN had nurses assigned to obesity education (median: 1) and 61%, dieticians-nutritionists (median: 2). On many occasions, educational roles are carried out by the same person, which is why the distribution between activities has been estimated in these cases. Important differences were found in relation to the structure and resources of the S-U_EyN depending on the complexity of the hospital (Table 1).
Structure of the S-U_EyN in hospitals by hospital size (2020).
| S-U_EyN structure | <500 beds | ≥500 beds | p |
|---|---|---|---|
| Number of beds (hospital) | 311 ± 105 | 790 ± 223 | – |
| Population in the catchment area of the S-U_EyN | 221,993 ± 124,009 | 422,299 ± 214,172 | – |
| Total number of endocrinologists assigned to the service | 4.9 ± 2.8 | 11.2 ± 4.1 | <0.001 |
| Endocrinologists per 100,000 inhabitants | 2.3 ± 0.9 | 2.9 ± 0.9 | 0.005 |
| Ratio of endocrinologists per 100 beds at the centre | 1.6 ± 0.7 | 1.5 ± 0.6 | 0.296 |
| Nutrition Unit integrated in the S-U_EyN | 80% | 98% | 0.002 |
| No. of consultation rooms | 4.1 ± 1.8 | 9.4 ± 4.6 | <0.001 |
| S-U_EyN day hospitala | 47% | 47% | 0.992 |
| % S-U_EyN with assigned beds | 45% | 91% | <0.001 |
| No. ultrasound machines in the S-U_EyN | 1.3 ± 0.6 | 2.0 ± 1.1 | <0.001 |
| No. diabetes nurse educatorsb | 2.1 ± 1.3 | 3.4 ± 1.7 | <0.001 |
| % of S-U_EyN with nurses dedicated to nutritionb | 51% | 98% | <0.001 |
| No. nurses dedicated to nutritionb | 1.3 ± 0.8 | 2.0 ± 1.8 | 0.073 |
| % of S-U_EyN with obesity education nursesb | 61.8% | 64.9% | 0.734 |
| No. obesity education nursesb | 0.83 ± 0.38 | 1.2 ± 0.89 | 0.029 |
| % of S-U_EyN with food technologists | 4% | 12% | 0.092 |
| % of S-U_EyN with dieticians-nutritionistsb | 49% | 72% | 0.013 |
| % of S-U_EyN with nutrition technicians | 11% | 28% | 0.022 |
S-U_EyN, endocrinology and nutrition services and units; No., number.
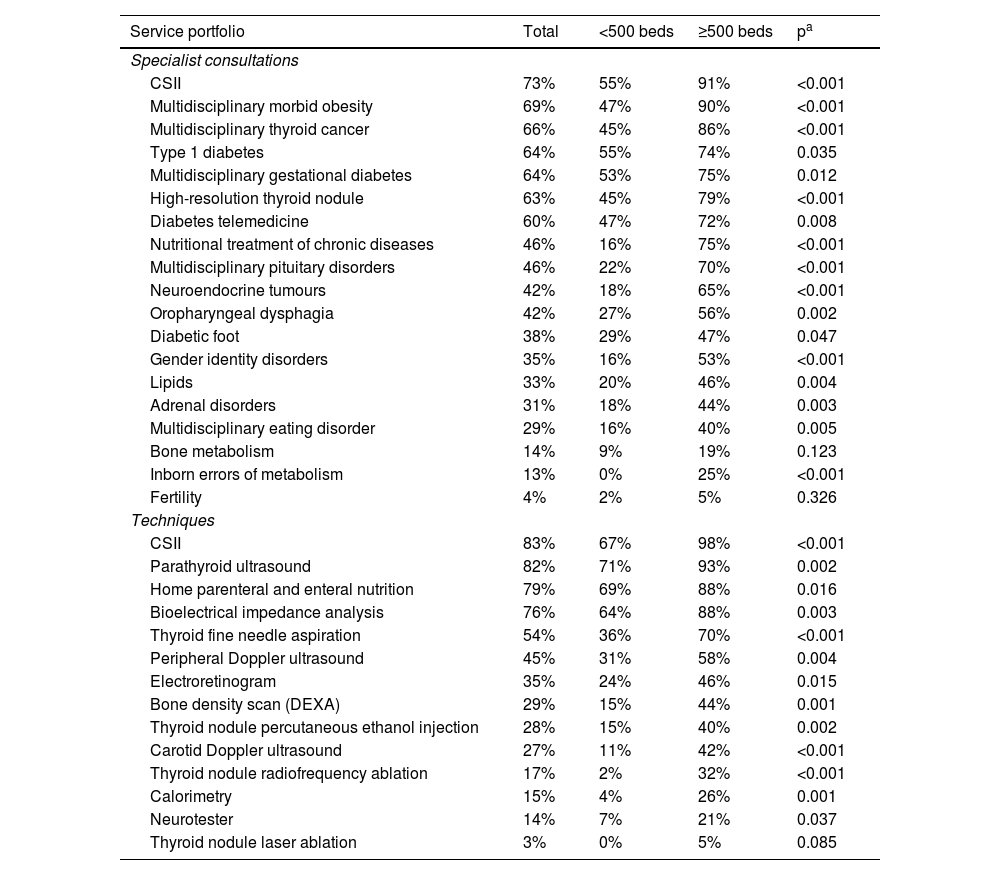
Some 97% of the S-U_EyN said that they had a structured relationship of some kind with primary care, while 70% of the S-U_EyN had developed an interconsultation service or unit with other hospital departments. Table 2 shows the service portfolio in specialist and technical units of the S-U_EyN in 2020. More than 50% of the S-U_EyN had units specifically for continuous subcutaneous insulin infusion (CSII) (73%), morbid obesity (69%), thyroid cancer (66%), type 1 diabetes (64%), diabetes and pregnancy (64%), high-resolution thyroid nodule (63%) and telemedicine in diabetes mellitus (60%). In terms of techniques, in 2020 > 50% of the S-U_EyN performed CSII insertion (83%), thyroid ultrasound (82%), home nutrition (79%), bioelectrical impedance analysis (76%) and fine needle aspiration of the thyroid (54%).
S-U_EyN service portfolio (2020).
| Service portfolio | Total | <500 beds | ≥500 beds | pa |
|---|---|---|---|---|
| Specialist consultations | ||||
| CSII | 73% | 55% | 91% | <0.001 |
| Multidisciplinary morbid obesity | 69% | 47% | 90% | <0.001 |
| Multidisciplinary thyroid cancer | 66% | 45% | 86% | <0.001 |
| Type 1 diabetes | 64% | 55% | 74% | 0.035 |
| Multidisciplinary gestational diabetes | 64% | 53% | 75% | 0.012 |
| High-resolution thyroid nodule | 63% | 45% | 79% | <0.001 |
| Diabetes telemedicine | 60% | 47% | 72% | 0.008 |
| Nutritional treatment of chronic diseases | 46% | 16% | 75% | <0.001 |
| Multidisciplinary pituitary disorders | 46% | 22% | 70% | <0.001 |
| Neuroendocrine tumours | 42% | 18% | 65% | <0.001 |
| Oropharyngeal dysphagia | 42% | 27% | 56% | 0.002 |
| Diabetic foot | 38% | 29% | 47% | 0.047 |
| Gender identity disorders | 35% | 16% | 53% | <0.001 |
| Lipids | 33% | 20% | 46% | 0.004 |
| Adrenal disorders | 31% | 18% | 44% | 0.003 |
| Multidisciplinary eating disorder | 29% | 16% | 40% | 0.005 |
| Bone metabolism | 14% | 9% | 19% | 0.123 |
| Inborn errors of metabolism | 13% | 0% | 25% | <0.001 |
| Fertility | 4% | 2% | 5% | 0.326 |
| Techniques | ||||
| CSII | 83% | 67% | 98% | <0.001 |
| Parathyroid ultrasound | 82% | 71% | 93% | 0.002 |
| Home parenteral and enteral nutrition | 79% | 69% | 88% | 0.016 |
| Bioelectrical impedance analysis | 76% | 64% | 88% | 0.003 |
| Thyroid fine needle aspiration | 54% | 36% | 70% | <0.001 |
| Peripheral Doppler ultrasound | 45% | 31% | 58% | 0.004 |
| Electroretinogram | 35% | 24% | 46% | 0.015 |
| Bone density scan (DEXA) | 29% | 15% | 44% | 0.001 |
| Thyroid nodule percutaneous ethanol injection | 28% | 15% | 40% | 0.002 |
| Carotid Doppler ultrasound | 27% | 11% | 42% | <0.001 |
| Thyroid nodule radiofrequency ablation | 17% | 2% | 32% | <0.001 |
| Calorimetry | 15% | 4% | 26% | 0.001 |
| Neurotester | 14% | 7% | 21% | 0.037 |
| Thyroid nodule laser ablation | 3% | 0% | 5% | 0.085 |
CSII, continuous subcutaneous insulin infusion; DEXA, dual X-ray absorptiometry; S-U_EyN, endocrinology and nutrition services and units.
Blank answers were considered “No”.
A progressive decrease in hospital discharges from the S-U_EyN (MBDS) was observed in the period from 2007 to 2019 (10,617 discharges in 2007 and 8,269 in 2019; IRR: 0.981; p < 0.001). Attendances (annual discharges from the S-U_EyN per 100,000 inhabitants over 17 years of age) fell from a rate of 28 in 2007 to 21 in 2019 (−25%) (IRR: 0.981; p < 0.001). The decrease in hospital attendances was accompanied by a decrease in the average length of stay in the discharges from the S-U_EyN, from 7.4 days in 2007 to 6.1 days in 2019 (IRR: 0.981; p < 0.001).
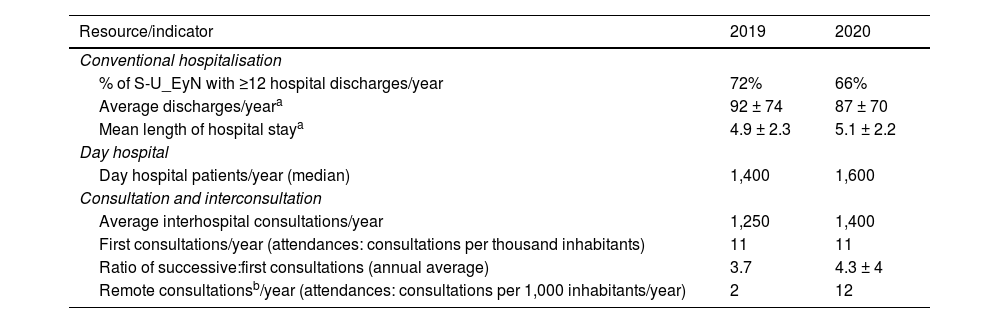
SurveyTable 3 shows the clinical activity of the S-U_EyN in 2019 and 2020 collected from the RECALSEEN survey. Overall, 66% of the S-U_EyN who responded to the survey had assigned hospitalisation beds. No clinically relevant differences were found in the activity of the S-U_EyN, with the exception of the notable increase in attendances of remote consultations, which went from two (2019) to 12 (2020) consultations of this type per 1,000 inhabitants per year. In all the activity indicators there was a wide variability between S-U_EyN. In relation to the tests/activities performed by the S-U_EyN, significant record problems were detected, which is why they are not included in this article, and can be consulted in the RECALSEEN 2021 report.9
Indicators of clinical activity by healthcare resource. RECALSEEN survey.
| Resource/indicator | 2019 | 2020 |
|---|---|---|
| Conventional hospitalisation | ||
| % of S-U_EyN with ≥12 hospital discharges/year | 72% | 66% |
| Average discharges/yeara | 92 ± 74 | 87 ± 70 |
| Mean length of hospital staya | 4.9 ± 2.3 | 5.1 ± 2.2 |
| Day hospital | ||
| Day hospital patients/year (median) | 1,400 | 1,600 |
| Consultation and interconsultation | ||
| Average interhospital consultations/year | 1,250 | 1,400 |
| First consultations/year (attendances: consultations per thousand inhabitants) | 11 | 11 |
| Ratio of successive:first consultations (annual average) | 3.7 | 4.3 ± 4 |
| Remote consultationsb/year (attendances: consultations per 1,000 inhabitants/year) | 2 | 12 |
S-U_EyN, endocrinology and nutrition services and units.
In total, 22% of the S-U_EyN had professionals dedicated to research, with a median for these units of 1.5 full-time professionals. Some 20% of the S-U_EyN that responded to the survey were integrated into a stable organisational structure (RETIC [REd Temática de Investigación Cooperativa (collaborative thematic research network)] or CIBER [Centro de Investigación Biomédica En Red (biomedical research centre network)]) promoted by the Instituto Carlos III [Carlos III Institute]. Overall, 60% of the S-U_EyN had, in 2020, active research projects from national or international, public or private competitive tenders. Fifty-one percent (51%) were involved in clinical trials, with a median of three trials for these units. In 67% of the units, at least one member of the service/unit had published in journals with an impact factor in the last two years. Some 56% of units participated in national disease registries.
Fifty-two percent (52%) of the S-U_EyN that responded to the survey were accredited for postgraduate training. Accredited units had a median of one resident in training per specialty year. In total, sixty percent of the units provided training to dieticians-nutritionists.
Thirteen percent of the S-U_EyN that responded to the survey had at least one professor, and 25%, at least one tenured professor, while 66% had at least one professor associated with the university.
Good practicesTable 4 shows the data on the implementation of good practices. In total, 45% of S-U_EyN had developed healthcare processes, with a median of three processes per unit, and 22% had quality certifications.
Good practices in the S-U_EyN (2020).
| Good practice | % |
|---|---|
| Healthcare team multidisciplinary meetings | 86% |
| Quality manager in the service/unit | 33% |
| Does the S-U_EyN hold clinical sessions? | 88% |
| Are these sessions accredited? | 40% |
| Periodic sessions with other hospital departments (neurosurgery, paediatrics, endocrine surgery, ENT, nuclear medicine, radiology, etc.) | 87% |
| Process management | |
| Does the service/unit have a process map? | 34% |
| Has process management been implemented for the unit's most relevant processes? | 39% |
| No. of processes performed by the unit | 45% units with a median of 3 processes |
| Presence of S-U_EyN quality commission professionals | 60% |
| Presence of S-U_EyN safety manager | 27% |
| Certification of the S-U_EyN (ISO, EFQM, etc.) | 22% |
S-U_EyN, endocrinology and nutrition services and units.
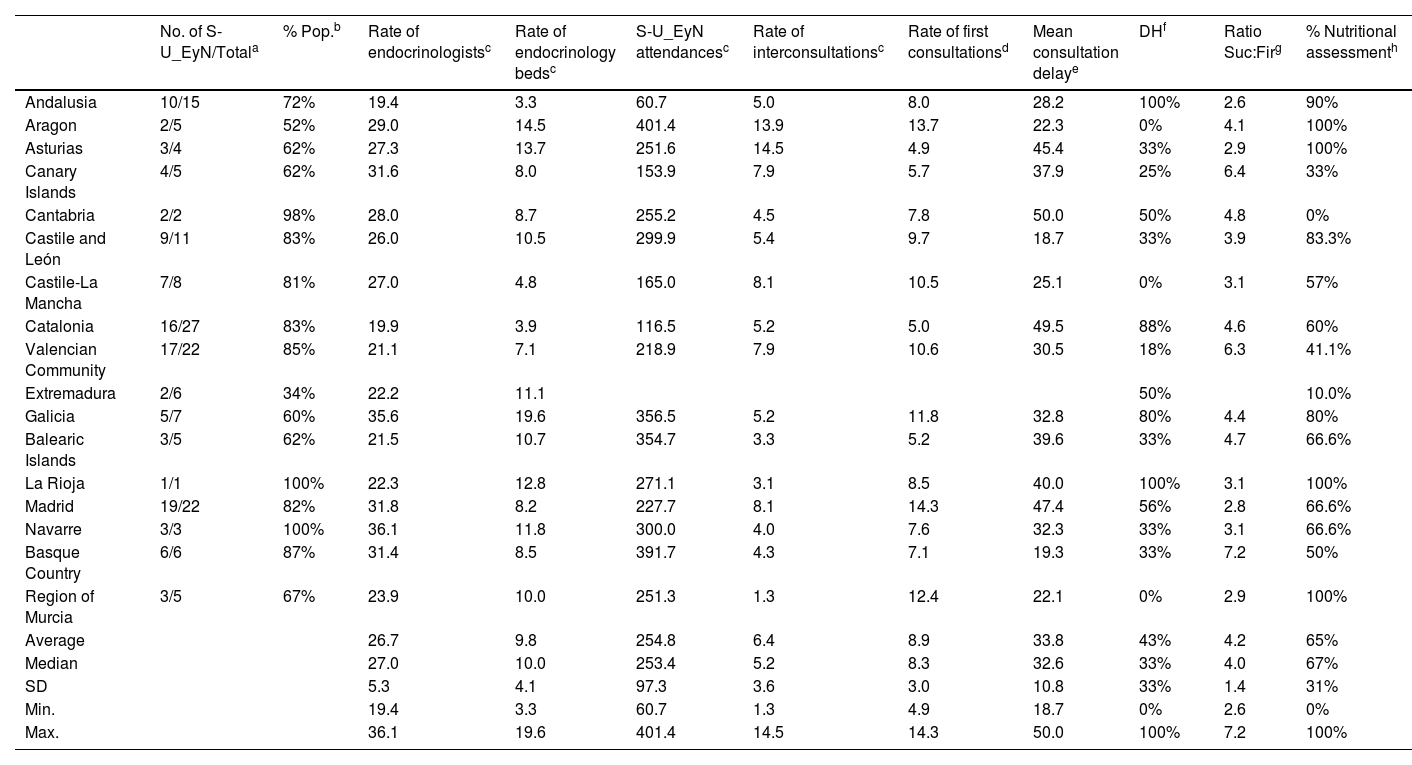
The lower the percentage of S-U_EyN that responded, as well as their population coverage, the lower the reliability of the estimates from the health services of the autonomous communities based on the RECALSEEN survey data. In this respect, the estimates for Aragon and Extremadura, which are below 50%, are not reliable, and those for Andalusia, Catalonia, the Balearic Islands and Murcia, which are below 70%, should be regarded with caution. Even with the aforementioned precaution, notable differences in endocrinology resources and activity between the health services of the autonomous communities are evident (Table 5).
Comparison of indicators between health services of the autonomous communities (2020).
| No. of S-U_EyN/Totala | % Pop.b | Rate of endocrinologistsc | Rate of endocrinology bedsc | S-U_EyN attendancesc | Rate of interconsultationsc | Rate of first consultationsd | Mean consultation delaye | DHf | Ratio Suc:Firg | % Nutritional assessmenth | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Andalusia | 10/15 | 72% | 19.4 | 3.3 | 60.7 | 5.0 | 8.0 | 28.2 | 100% | 2.6 | 90% |
| Aragon | 2/5 | 52% | 29.0 | 14.5 | 401.4 | 13.9 | 13.7 | 22.3 | 0% | 4.1 | 100% |
| Asturias | 3/4 | 62% | 27.3 | 13.7 | 251.6 | 14.5 | 4.9 | 45.4 | 33% | 2.9 | 100% |
| Canary Islands | 4/5 | 62% | 31.6 | 8.0 | 153.9 | 7.9 | 5.7 | 37.9 | 25% | 6.4 | 33% |
| Cantabria | 2/2 | 98% | 28.0 | 8.7 | 255.2 | 4.5 | 7.8 | 50.0 | 50% | 4.8 | 0% |
| Castile and León | 9/11 | 83% | 26.0 | 10.5 | 299.9 | 5.4 | 9.7 | 18.7 | 33% | 3.9 | 83.3% |
| Castile-La Mancha | 7/8 | 81% | 27.0 | 4.8 | 165.0 | 8.1 | 10.5 | 25.1 | 0% | 3.1 | 57% |
| Catalonia | 16/27 | 83% | 19.9 | 3.9 | 116.5 | 5.2 | 5.0 | 49.5 | 88% | 4.6 | 60% |
| Valencian Community | 17/22 | 85% | 21.1 | 7.1 | 218.9 | 7.9 | 10.6 | 30.5 | 18% | 6.3 | 41.1% |
| Extremadura | 2/6 | 34% | 22.2 | 11.1 | 50% | 10.0% | |||||
| Galicia | 5/7 | 60% | 35.6 | 19.6 | 356.5 | 5.2 | 11.8 | 32.8 | 80% | 4.4 | 80% |
| Balearic Islands | 3/5 | 62% | 21.5 | 10.7 | 354.7 | 3.3 | 5.2 | 39.6 | 33% | 4.7 | 66.6% |
| La Rioja | 1/1 | 100% | 22.3 | 12.8 | 271.1 | 3.1 | 8.5 | 40.0 | 100% | 3.1 | 100% |
| Madrid | 19/22 | 82% | 31.8 | 8.2 | 227.7 | 8.1 | 14.3 | 47.4 | 56% | 2.8 | 66.6% |
| Navarre | 3/3 | 100% | 36.1 | 11.8 | 300.0 | 4.0 | 7.6 | 32.3 | 33% | 3.1 | 66.6% |
| Basque Country | 6/6 | 87% | 31.4 | 8.5 | 391.7 | 4.3 | 7.1 | 19.3 | 33% | 7.2 | 50% |
| Region of Murcia | 3/5 | 67% | 23.9 | 10.0 | 251.3 | 1.3 | 12.4 | 22.1 | 0% | 2.9 | 100% |
| Average | 26.7 | 9.8 | 254.8 | 6.4 | 8.9 | 33.8 | 43% | 4.2 | 65% | ||
| Median | 27.0 | 10.0 | 253.4 | 5.2 | 8.3 | 32.6 | 33% | 4.0 | 67% | ||
| SD | 5.3 | 4.1 | 97.3 | 3.6 | 3.0 | 10.8 | 33% | 1.4 | 31% | ||
| Min. | 19.4 | 3.3 | 60.7 | 1.3 | 4.9 | 18.7 | 0% | 2.6 | 0% | ||
| Max. | 36.1 | 19.6 | 401.4 | 14.5 | 14.3 | 50.0 | 100% | 7.2 | 100% |
DH, day hospital; SD, standard deviation; S-U_EyN, endocrinology and nutrition services and units.
% of the total population of the autonomous community in the catchment area of the hospitals' S-U_EyN that responded to the survey. Both indicators should be used to get closer to the reliability of the indicators.
The RECALSEEN 2021 survey provides relevant information on several aspects of the structure, resources and activities of the S-U_EyN. The most significant findings were as follows: (1) the notable inter-regional differences in provision of resources; (2) the significant interrelationship of the S-U_EyN with other departments and units in both primary and specialised care; (3) the remarkable impetus that the S-U_EyN have experienced regarding the prospect of the "hospital of the future"10: shifting processes to the outpatient setting and telemedicine; (4) the existing gap with the standards established by the SEEN; and (5) the acknowledgement of a long journey towards the implementation of good practices in the S-U_EyN.
There are notable inter-regional differences both in resources (endocrinologists per 1,000,000 inhabitants, assigned beds) and in the use of S-U_EyN (hospital admissions, outpatient consultations) (Table 5). The extent to which these differences may be associated with inequalities in health outcomes between health services in the autonomous communities should be investigated. Regarding the rate of endocrinologists, it should be noted that the estimate calculated through the RECALSEEN survey (2.5 per 100,000 inhabitants) tallies with the estimate from the Ministry of Health (2.6), which uses a different methodology.11
The concept of multidisciplinarity seems to be incorporated into the S-U_EyN. Practically all of the S-U_EyN have structured relationship systems with primary care, and 70% of the S-U_EyN have developed an interconsultation unit with other departments. Although progress should probably be made in the implementation of more structured interrelational models with other departments and with primary care, the role of endocrinology and nutrition in the provision of patient-focussed multidisciplinary care will probably be one of the challenges of future development.
The shift of endocrinological care to the outpatient setting is a trend in the S-U_EyN that was detected in the 2017 survey. The rate of hospital admissions in the S-U_EyN has decreased significantly throughout the period from 2007 to 2019, accompanied by a progressive decrease in length of hospital stay, in a context of admissions of progressively older or very elderly patients,12 with a notable increase in comorbidities, including diabetes and malnutrition.13,14 In the scenario of the "hospital of the future", the notable impetus that the S-U_EyN have given to the use of telemedicine in all its modalities is also noteworthy. The rate of remote consultations per 1,000 inhabitants per year was slightly higher in 2020 than the rate of first consultations, representing a six-fold increase on 2019 (Table 3). This can most probably be explained by adaptation to the healthcare overburden arising from the SARS-CoV-2 pandemic, and is a trend that is likely to continue in the future. Developing quality "telemedicine", which involves the need to equip endocrinologists and the other healthcare professionals integrated in the S-U_EyN with digital skills, is probably going to be another future challenge for the specialty.15 In this sense, the development of instruments such as those created by the SEEN16 and other scientific-medical societies,17 shifting processes to the outpatient setting, multidisciplinarity and digitisation are just some of the relevant healthcare challenges for the immediate future.
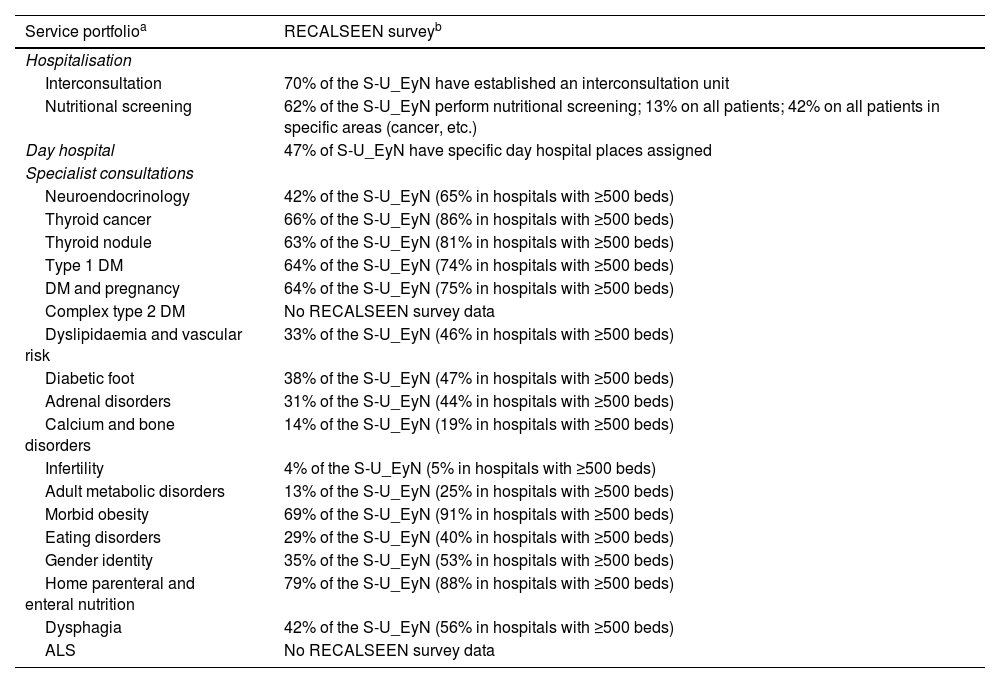
In relation to the S-U_EyN portfolio of services, the information collected in the 2021 survey shows a considerable step forward compared to 2017. There are, however, meaningful gaps compared to the proposal prepared by the SEEN16 (Table 6). Where these gaps seem most significant is in the methodical performance of nutritional screening in hospitalised patients (13% in all patients; 42% in specific areas); the assignment of day hospitals to the S-U_EyN (47%), the day hospital having special relevance for diabetes; as well as in the provision of some specialist units, especially in more complex hospitals (500 or more beds). Adequate provision of resources for the S-U_EyN of referral centres (health or regional area) and, probably, the establishment of healthcare networks that integrate the units in centres of lower volume and complexity with the S-U_EyN of their referral centres18 are possible challenges that the S-U_EyN must face in the immediate future.
Full service portfolio vs. RECALSEEN survey (2020).
| Service portfolioa | RECALSEEN surveyb |
|---|---|
| Hospitalisation | |
| Interconsultation | 70% of the S-U_EyN have established an interconsultation unit |
| Nutritional screening | 62% of the S-U_EyN perform nutritional screening; 13% on all patients; 42% on all patients in specific areas (cancer, etc.) |
| Day hospital | 47% of S-U_EyN have specific day hospital places assigned |
| Specialist consultations | |
| Neuroendocrinology | 42% of the S-U_EyN (65% in hospitals with ≥500 beds) |
| Thyroid cancer | 66% of the S-U_EyN (86% in hospitals with ≥500 beds) |
| Thyroid nodule | 63% of the S-U_EyN (81% in hospitals with ≥500 beds) |
| Type 1 DM | 64% of the S-U_EyN (74% in hospitals with ≥500 beds) |
| DM and pregnancy | 64% of the S-U_EyN (75% in hospitals with ≥500 beds) |
| Complex type 2 DM | No RECALSEEN survey data |
| Dyslipidaemia and vascular risk | 33% of the S-U_EyN (46% in hospitals with ≥500 beds) |
| Diabetic foot | 38% of the S-U_EyN (47% in hospitals with ≥500 beds) |
| Adrenal disorders | 31% of the S-U_EyN (44% in hospitals with ≥500 beds) |
| Calcium and bone disorders | 14% of the S-U_EyN (19% in hospitals with ≥500 beds) |
| Infertility | 4% of the S-U_EyN (5% in hospitals with ≥500 beds) |
| Adult metabolic disorders | 13% of the S-U_EyN (25% in hospitals with ≥500 beds) |
| Morbid obesity | 69% of the S-U_EyN (91% in hospitals with ≥500 beds) |
| Eating disorders | 29% of the S-U_EyN (40% in hospitals with ≥500 beds) |
| Gender identity | 35% of the S-U_EyN (53% in hospitals with ≥500 beds) |
| Home parenteral and enteral nutrition | 79% of the S-U_EyN (88% in hospitals with ≥500 beds) |
| Dysphagia | 42% of the S-U_EyN (56% in hospitals with ≥500 beds) |
| ALS | No RECALSEEN survey data |
S-U_EyN, endocrinology and nutrition services and units.
The 2021 survey revealed no significant improvements in the implementation of good practices in the S-U_EyN compared to the 2017 survey, with still only a low proportion (39%) of S-U_EyN that have implemented process management for their most relevant processes, with considerable room for improvement in this area (38% in 2017).
The 2021 survey confirms the notable research activity of the S-U_EyN detected in 2017. Some 22% of the S-U_EyN had professionals dedicated to research versus 24% in 2017; 60% had active research projects versus 48% in 2017; 51% were involved in clinical trials versus 63% in 2017; and 67% had published at least one article in journals with an impact factor versus 59% in 2017.
Although falling outside the scope of this article, the information available from the RECALSEEN project could be used to analyse the possible association between the structure and activity of the S-U_EyN with health outcomes, and especially if the inequalities observed in health outcomes between autonomous communities19,20 are associated with differences in resources or activity.
LimitationsAs with RECALSEEN 2017, the reliability of the estimates, which depend, among other factors, on the representativeness of the sample in each autonomous community and the types of centre and S-U_EyN, must be borne in mind. Given that the sample is large, however, it does not seem controversial to assert that the information gleaned from it is representative of the current situation of the S-U_EyN; although it cannot be defined as a statistically significant sample. As has been pointed out, the activity data from 2020 are surely influenced by the healthcare changes induced by the adaptation of hospitals to the SARS-CoV-2 pandemic. Finally, although there are no statistically significant differences in the volume of S-U_EyN hospitals that responded to the survey in 2021 compared to 2017, the percentage of units that responded differs considerably, and not all the S-U_EyN that responded in 2017 did so in 2021, so the comparison of results between the two periods is merely an indication, without statistical comparisons being established.
ConclusionsThe RECALSEEN 2021 survey provides relevant information on the resources and activity of the S-U_EyN. The data and information generated identify some of the most significant challenges for the specialty, the S-U_EyN and for the SEEN: the role of endocrinology and nutrition in providing patient-focussed multidisciplinary care; the development of quality "telemedicine"; adequate provision of resources for the S-U_EyN and the establishment of healthcare networks; the implementation of healthcare process management; and the reduction of possible inequalities in care for endocrine diseases and nutritional disorders between health centres and services.
Conflicts of interestThe authors declare that they have no conflicts of interest.
The following is Supplementary data to this article:
