




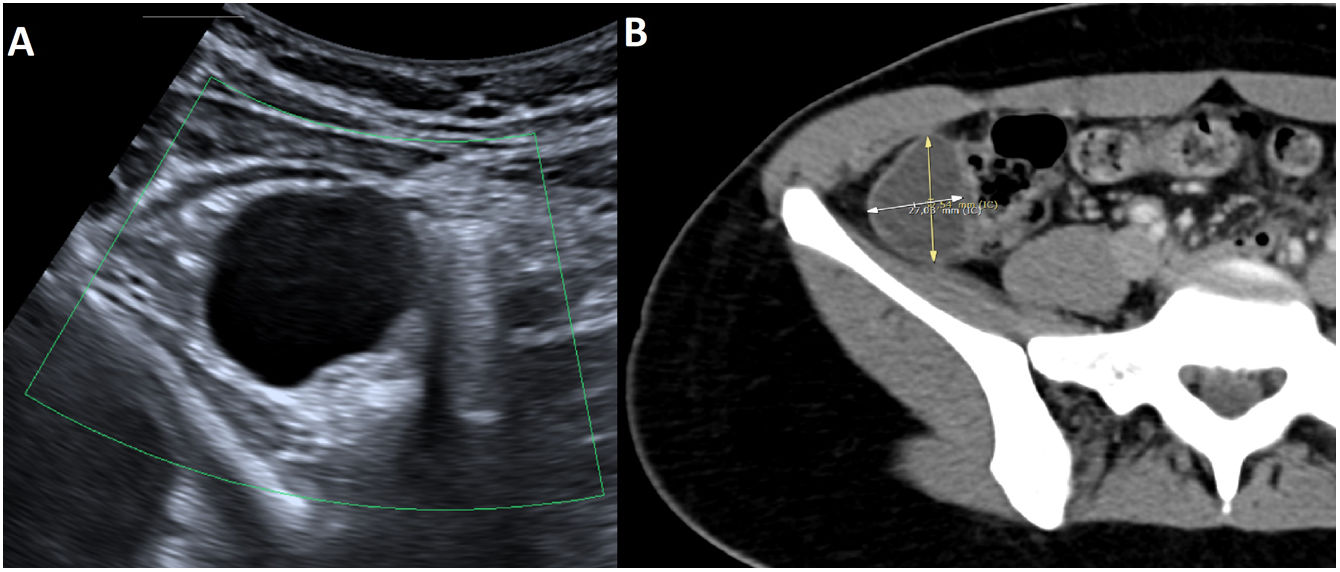
This was a 24-year-old woman, who attended Accident and Emergency for right iliac fossa (RIF) pain and nausea. On physical examination, the patient showed guarding in RIF, with no analytical abnormalities. Abdominal ultrasound showed a 27 mm peri-caecal cystic lesion1 which was confirmed by computed tomography (CT). The CT scan showed the lesion to be located alongside the caecum, not attached to the vermiform appendix, having thin, well-defined walls, with no signs of inflammation (Fig. 1). Diagnostic imaging suggested enteric duplication cyst (EDC) as a first choice, with appendiceal mucocele or endometrioma being less likely.

Image A: abdominal ultrasound showing a well-defined, anechogenic lesion lateral to the caecum, with thin walls and no vascularisation on colour Doppler study. Image B: Contrast-enhanced CT scan showing a lesion located in the RIF, adjacent to the caecum and independent of the vermiform appendix, with well-defined walls.
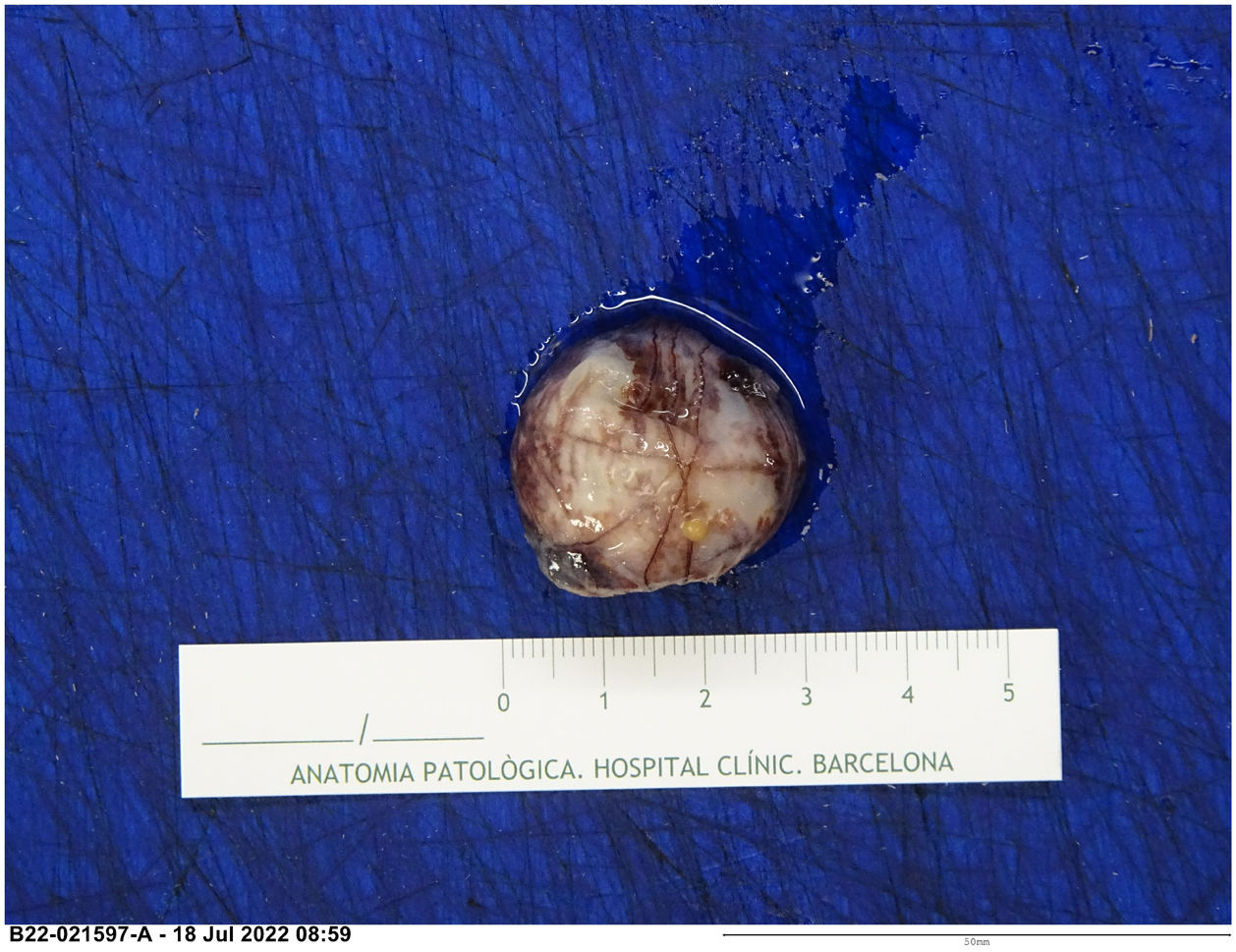
Laparoscopy identified a cystic lesion sharing serous membrane with the caecum and excision was performed. Pathology described a cystic lesion with fibrous walls lined by an epithelium of mesothelial cells without atypia, compatible with EDC (Fig. 2).

EDC is a rare congenital lesion diagnosed in the paediatric age group.2 It is often asymptomatic or presents with very non-specific symptoms, including abdominal pain, obstruction or intussusception.3 It can be found anywhere in the gastrointestinal tract, the ileum being the most common location and the colon the least.4 Given its low incidence in adults, it is important to be aware of this condition as a rare cause of acute abdomen due to its difficult diagnosis.
