




Article information
Full Text
Bibliography
Download PDF
Statistics
Figures (3)
Show moreShow less
Tables (5)
Table 1. Classification of angioedema without wheals.
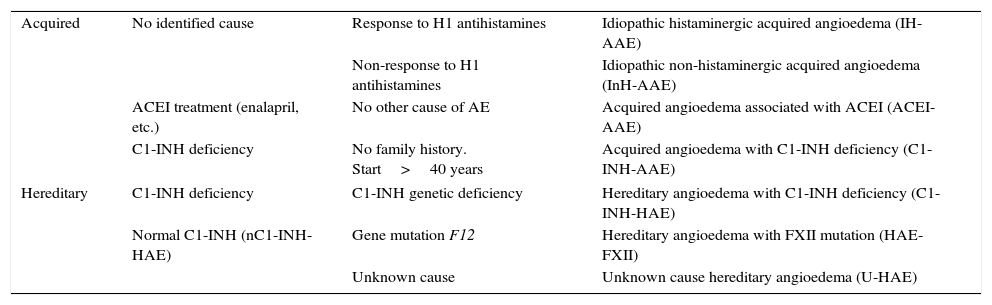
Table 2. Precipitating factors, typical prodromes and symptoms of hereditary angioedema.
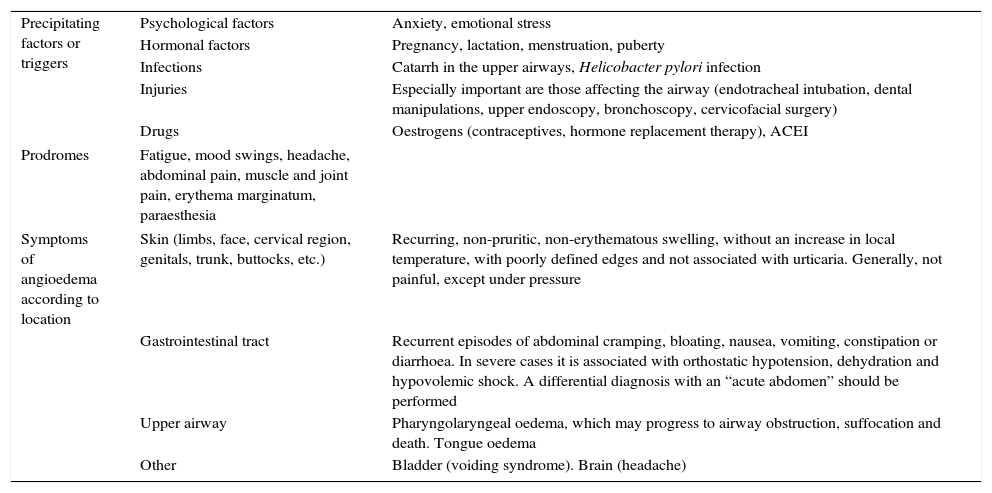
Table 3. Complement values in the different types of bradykinergic angioedema.
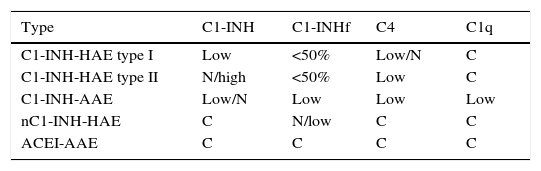
Table 4. Drugs for the treatment of hereditary angioedema and their availability in Spain.
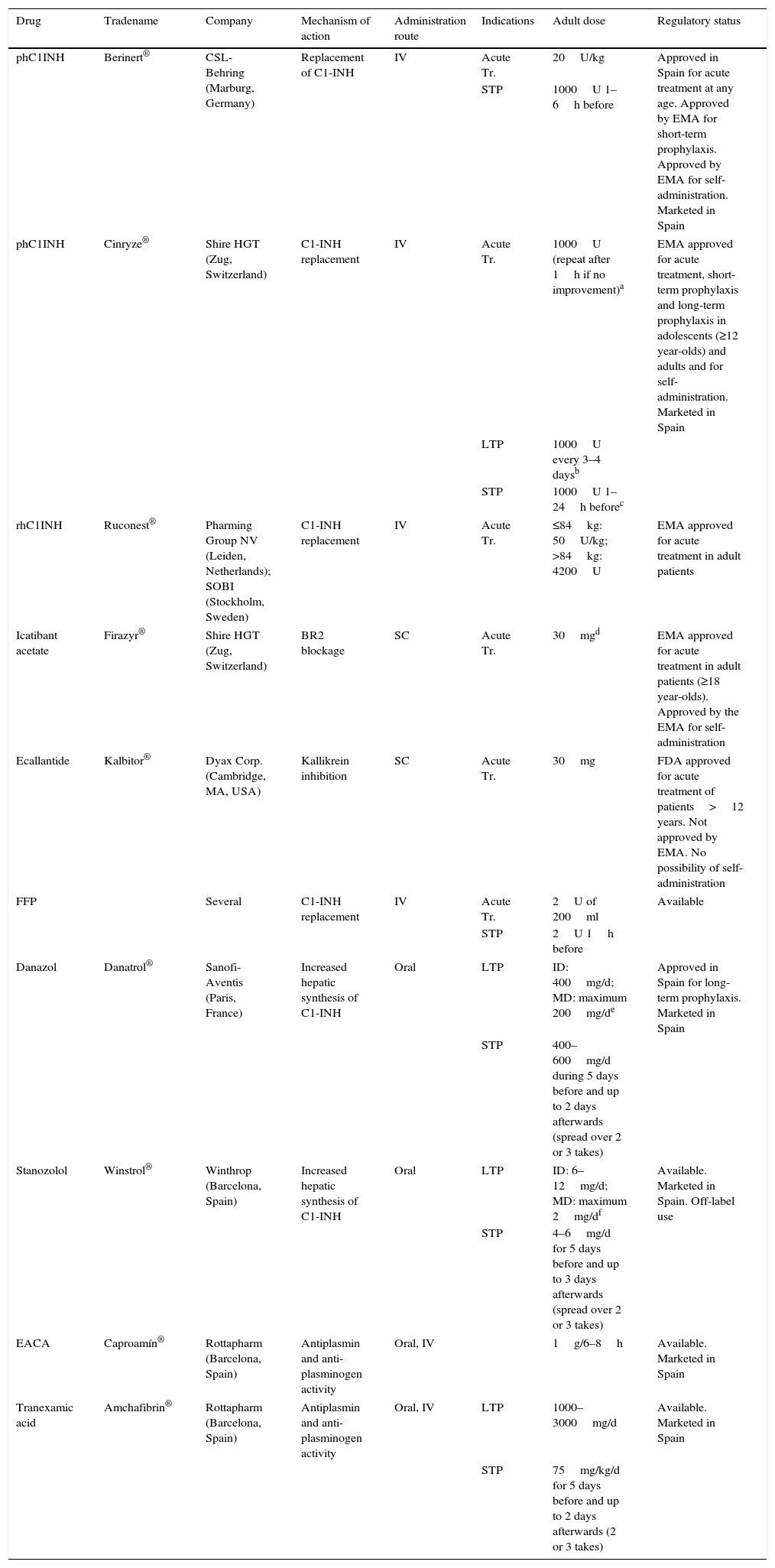
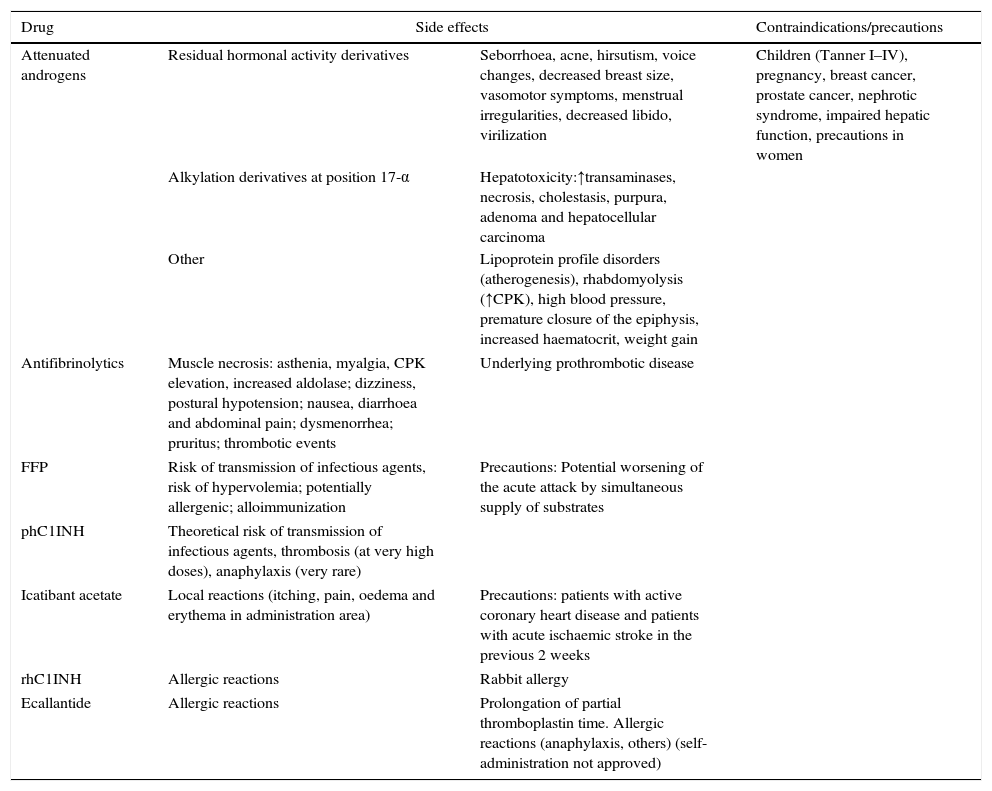
Table 5. Side effects and contraindications of drugs used in hereditary angioedema.
Show moreShow less
Article
These are the options to access the full texts of the publication Medicina Clínica (English Edition)
Subscriber
Subscribe
Purchase
Contact
Phone for subscriptions and reporting of errors
From Monday to Friday from 9 a.m. to 6 p.m. (GMT + 1) except for the months of July and August which will be from 9 a.m. to 3 p.m.
Calls from Spain
932 415 960
Calls from outside Spain
+34 932 415 960
E-mail
