



A 20-year-old woman was diagnosed with mitral regurgitation due to an anterior mitral leaflet perforation. After completing the preoperative study no clear etiology was found, considering it to be of congenital origin.
Surgical repair was performed with a patch of bovine pericardium and a ring annuloplasty. Serial echocardiograms taken postoperatively showed no regurgitation across the mitral valve.
Mujer de 20 años diagnosticada de insuficiencia mitral por perforación de velo mitral anterior. Tras realizar el estudio preoperatorio no se encontró una etiología clara, considerándose de origen congénito.
La reparación quirúrgica se realizó con parche de pericardio bovino y anuloplastia con anillo. Los ecocardiogramas en serie realizados después de la cirugía no mostraron regurgitación residual.
A congenital perforation on the anterior leaflet is a very rare cause of mitral regurgitation (MR).1,2 We report the case of a young adult with mitral regurgitation due to an isolated anterior leaflet perforation without any other valve anomaly and with no evidence of previous endocarditis, systemic disease or trauma. The mitral valve was surgically repaired using a pericardial patch and ring annuloplasty.
Case reportA 20-year-old asymptomatic woman was diagnosed with mitral regurgitation due to a cardiac murmur.
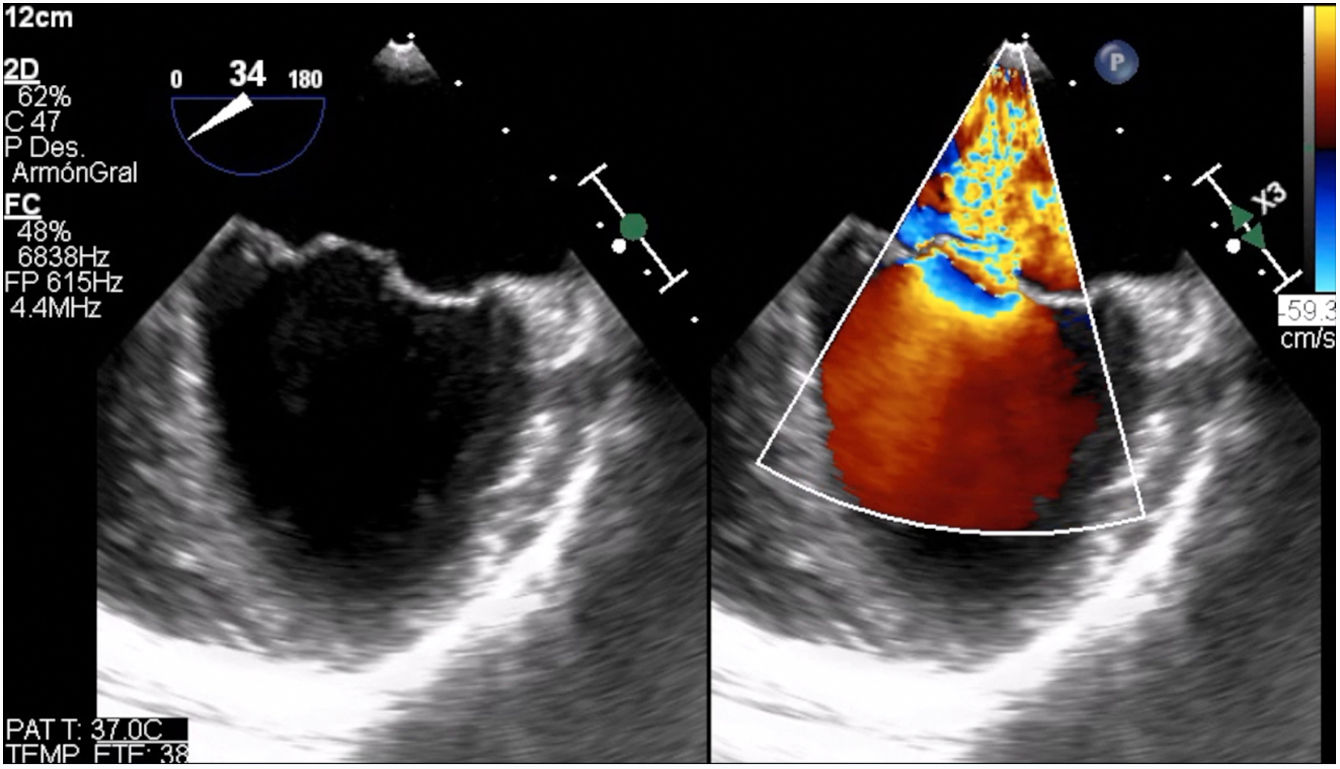
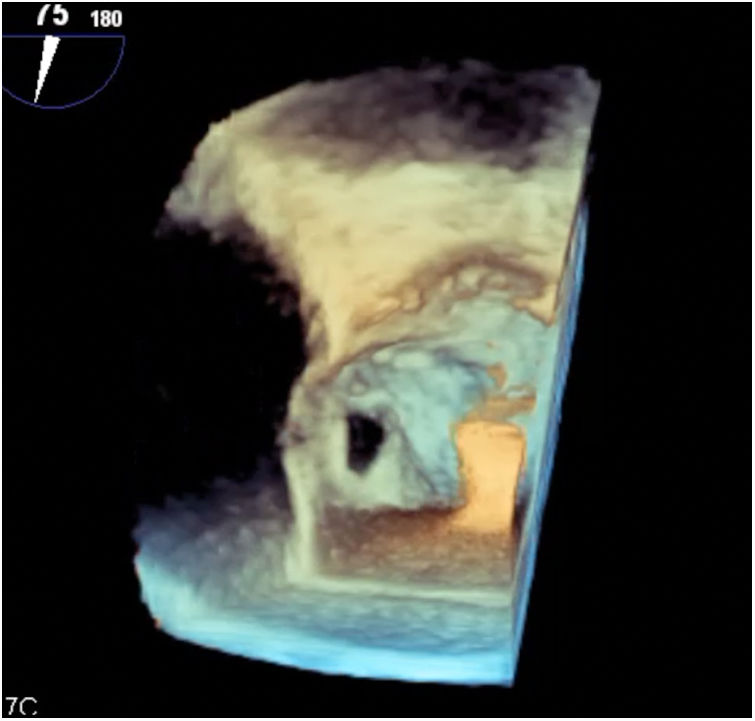
The transthoracic and transesophageal echocardiography (TTE and TEE) identified a Carpentier type I severe MR secondary to an isolated anterior mitral leaflet perforation with ventricular and atrial dilatation (LVEDV index 37mm/m2, Left Atrium: 75ml/m2), and preserved left ventricular ejection fraction (LVEF 69%). Ventricular septal defects and other cardiac anomalies were excluded. No other mitral valve abnormalities were found. No vegetations were seen, and no previous fever or signs of infective endocarditis were found in the clinical examination (Figs. 1 and 2, Online Resource 1).


Despite the absence of symptoms, the patient was referred for surgical repair due to the significant dilation of left cavities and the severity of the regurgitation.
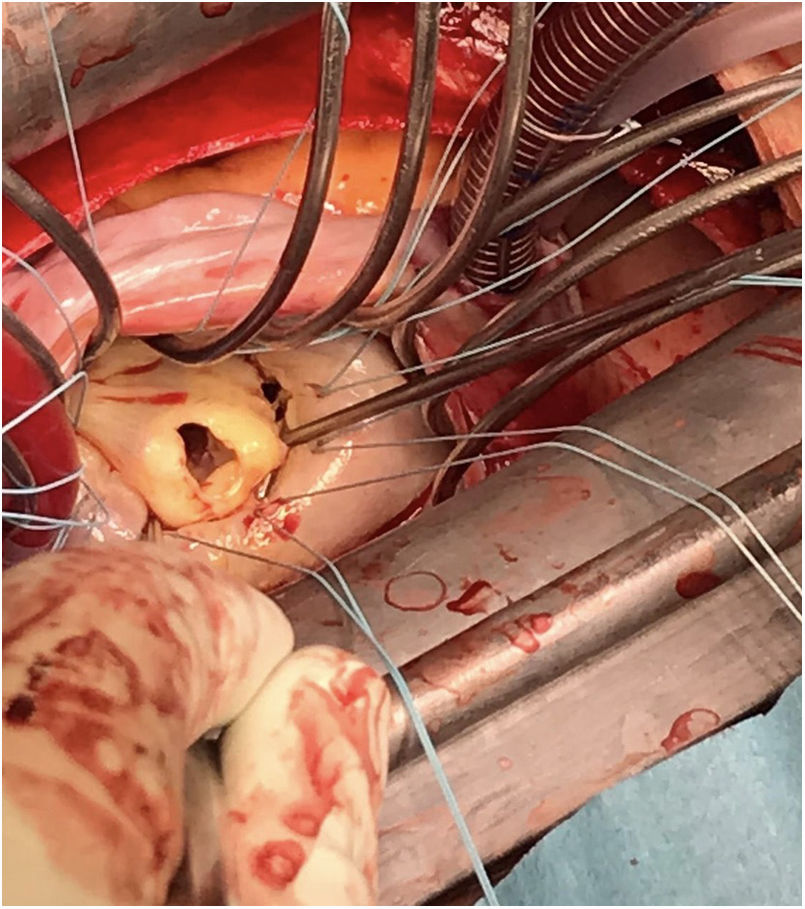
Surgical exploration showed a 7mm isolated perforation in the A2 segment. Free edge and mitral chordae of the anterior leaflet were normal. The entire posterior leaflet, both commissures and the subvalvular apparatus were normal. Mitral annulus was slightly dilated. No visual signs of mitral valve endocarditis were found (Fig. 3).

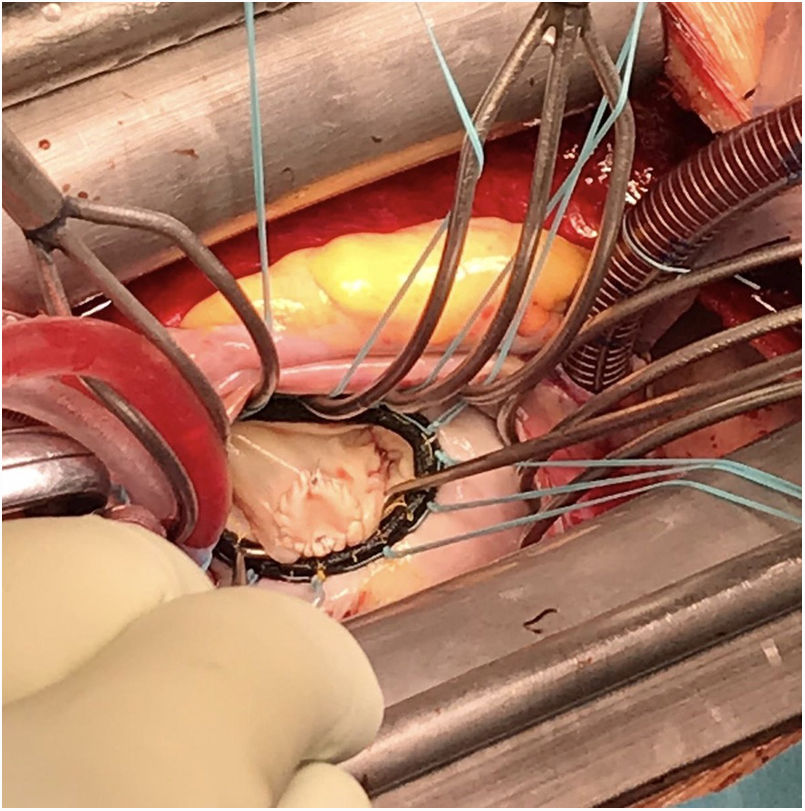
Mitral valve repair was performed by closing the defect with a circular patch of bovine pericardium and continuous suture. A mitral annuloplasty was performed using a 32mm Memo 3D Rechord ring (Sorin Group®) (Fig. 4).

Intraoperative TEE showed no residual MR or stenosis. As postoperative complications, the patient presented electrocardiographic signs of pericarditis and moderate pericardial effusion without hemodynamic compromise in the TTE, treated with nonsteroidal anti-inflammatory drugs. Patient was discharged on the 5th day after surgery. TTE before discharge revealed a minimal residual mitral regurgitation (Online Resource 2).
Four months after surgery the patient is in NYHA class I.
DiscussionMitral valve leaflet perforation is a rare cause of MR.2 Secondary leaflet perforations are normally associated with infective endocarditis, inflammatory or connective tissue diseases and iatrogenic or traumatic lesions.1,3 In some cases, an aortic regurgitation jet as a cause for mitral leaflet perforation has been suggested.4 Congenital mitral regurgitation is normally associated with clefts, leaflet malformations, congenital prolapse or chordae or subvalvular malformation.
In the reported case, a casual diagnosis of a severe mitral regurgitation due to an isolated anterior mitral leaflet perforation was made. No clinical history or signs of infective endocarditis, trauma or systemic inflammatory disease was found. TTE and TEE revealed an isolated leaflet perforation as a single mechanism for the severe mitral regurgitation. No other valve abnormalities were found either in the mitral or any other valve. The leaflet perforation was believed to be congenital as we were unable to find any other cause for it. Congenital isolated anterior leaflet perforation has been described as cause for mitral regurgitation in children,5 but to the best of our knowledge this is the first case reported in a young adult. In our case, surgical repair was performed closing the defect with a bovine pericardial patch and a ring annuloplasty, with trace residual MR in the postoperative echocardiography.
ConclusionIsolated anterior leaflet perforation is a very rare cause of mitral regurgitation in adults. Surgical repair with pericardial patch closure and annuloplasty is a safe and effective treatment.
Ethical considerationsPatient written consent for taking pictures for a scientific and formative purpose was obtained, explaining that the any images taken would never be accompanied of potentially identifiable information.
FundingNone.
Conflict of interestNone declared.

