




The aim of this study is to evaluate the usefulness of Vicryl Plus® suture in reducing the rate of postoperative wound infection in elective colorectal surgery.
MethodsA prospective case–control multicenter study with 480 patients undergoing elective colorectal surgery was performed between 2006 and 2007. Patients were divided in 2 groups of equal sample size: group 1, closure of the abdominal wall using Vicryl Plus® and group 2 where PDS II® was used. The study involved 5 hospitals in the Spanish State. Wound infection was classified into superficial and deep. All patients diagnosed of wound infection during the hospital stay and up to 30 days after discharge were studied. For the statistical analysis Chi-square test and Fisher exact were used for bivariate analysis and logistic regression model for multivariate analysis.
ResultsWound infection rates were significantly lower in group 1: 14.6 vs 29.2. Multivariate analysis showed that risk of wound infection was higher in patients with cancer, lung disease, anemia, operative time greater than 2h, lack of second dose intra-operative prophylactic antibiotic and laparotomy closure with PDS suture II®.
ConclusionsThe use of suture coated with triclosan can be an effective prophylactic tool in reducing wound infection rate in patients undergoing elective colorectal surgery.
El objetivo de este estudio es evaluar la utilidad del material de sutura Vicryl Plus® en reducir la tasa de infección de herida postoperatoria en cirugía colorrectal electiva.
MétodoEstudio de casos y controles prospectivo multicéntrico sobre 480 pacientes intervenidos de cirugía colorrectal electiva entre el 2006 y 2007, divididos en 2 grupos de igual tamaño muestral, sometidos a cierre de pared abdominal mediante uso de Vicryl Plus® (grupo 1) y PDS II® (grupo 2). En el estudio participaron 5 centros hospitalarios del Estado Español. La infección de herida fue clasificada en superficial y profunda. Fueron incluidos todos los pacientes diagnosticados de infección de herida durante la estancia hospitalaria y hasta 30 días después del alta. Para el estudio estadístico fueron utilizados el test del Chi-cuadrado y el exacto de Fisher para el análisis bivariante y el modelo de regresión logística para el análisis multivariante.
ResultadosLa tasa de infección de herida observada fue significativamente inferior en el grupo 1: 14,6 frente al 29,2 del grupo 2. Según el estudio multivariante, el riesgo de infección de herida es superior en los pacientes con neoplasia, enfermedad pulmonar, anemia, tiempo operatorio superior a 2h, falta de segunda dosis profiláctica intraoperatoria y cierre de laparotomía con sutura de PDS II®.
ConclusionesEl uso de material de sutura recubierto de triclosan puede ser una herramienta profiláctica eficaz para disminuir la tasa de infección de herida operatoria en los pacientes intervenidos mediante cirugía colorrectal electiva.
Wound infection is the most common complication among patients undergoing elective colorectal surgery; it has a significant impact on morbidity and health care costs. Incidence varies between 5% and 40%; the main reason for this discrepancy depends on whether infections occurring after hospital discharge are included or not.1–5 The etiology of surgical infection is multifactorial and results from the interaction of many variables related to the patient, germ, intervention and hospitalization. Diabetes, malnutrition, immunosuppression, obesity, anemia and transfusion have been the main risk factors studied.6–20
Other causes have been related to the surgical intervention, such as hypothermia, hypoxia, surgery type, bowel preparation, procedure duration, use of wall protection methods, antibiotic prophylaxis and the time of administration.6–13 In recent years, there has been growing interest in how suture materials influence wound infection development. The hypothesis is that suture materials favor bacterial colonization, reducing local and systemic therapeutic measure effectiveness.8 Vicryl Plus® is a suture thread coated with triclosan to fight Gram-positive and Gram-negative bacteria, thus reducing the potential for infection initiation and propagation; in vitro studies and animal models have demonstrated its effectiveness.14–19 However, there is less scientific evidence of its efficacy from a clinical point of view. This study has aimed mainly to evaluate the possible clinical benefit of Vicryl Plus® in reducing wound infection rates and decreasing hospital stay for patients with infected wounds from elective colorectal surgery laparotomy closures.
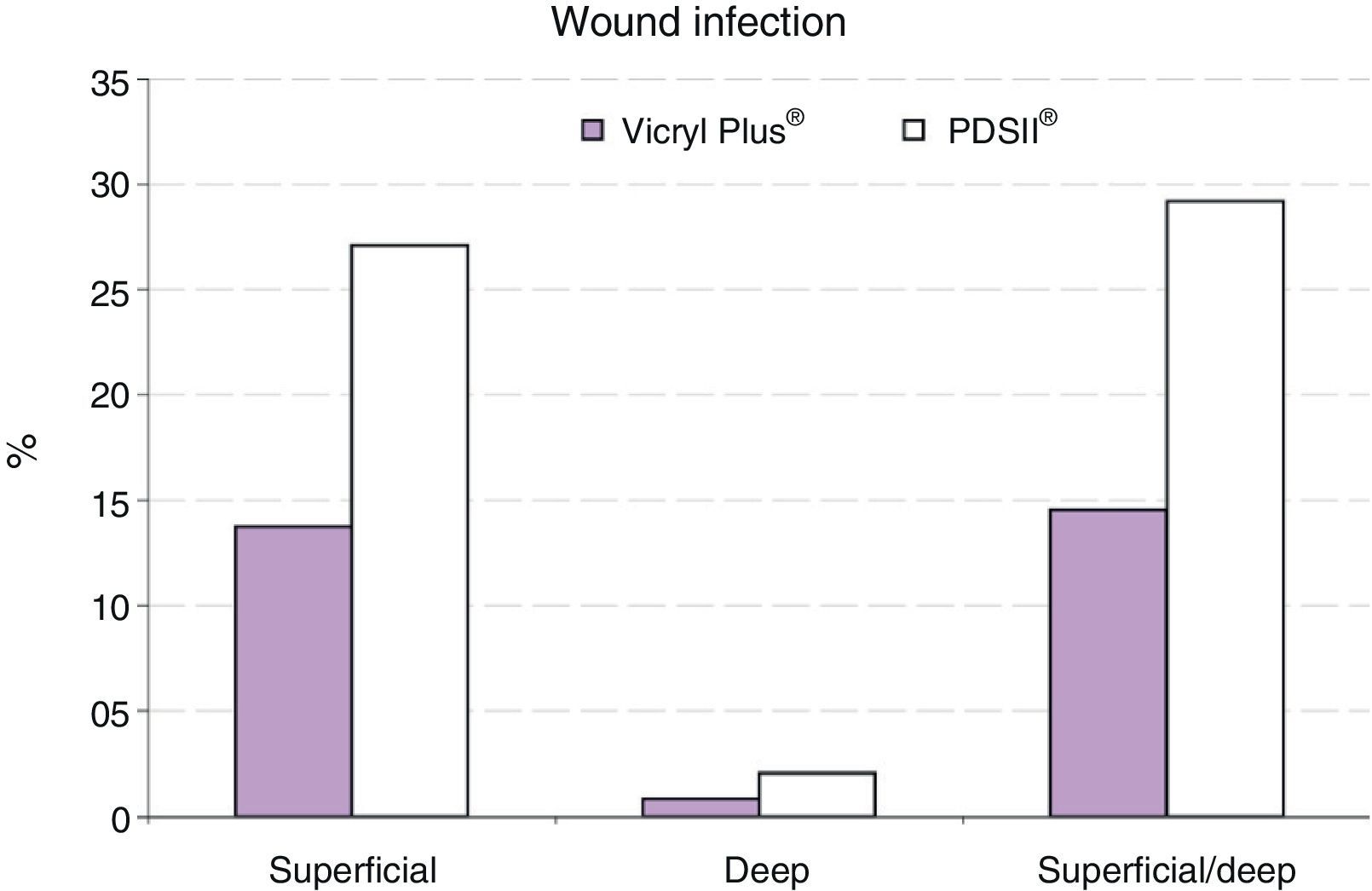
MethodIn order to assess the actual benefit of a suture material with antiseptic properties on laparotomy closures, a prospective case–control study was conducted including patients who underwent surgery for elective colorectal disease in 2006–2007. The study group comprised 240 consecutive patients who underwent abdominal wall closure with Vicryl Plus® (Triclosan, Ethicon Deutschland, Norderstedt, Germany coated antibacterial polyglactin 910), whereas the control group comprised 240 patients who underwent laparotomy closure with conventional PDSII suture® (Polydioxanone, Ethicon Deutschland, Norderstedt, Germany). Control patients were selected retrospectively with the same inclusion and exclusion criteria of the studied group. All surgical procedures included were classified as clean-contaminated surgery. The study excluded patients with emergency colorectal resection, colorectal disease with multivisceral resection, and contaminated colorectal surgery cases. Wound infection was defined as spontaneous drainage of purulent material from the wound or from the surgeon's deliberate revision and positive culture of drained serous fluid. Infections were classified as superficial (skin and subcutaneous tissue), and deep (fascia and muscle tissue). All wound infection cases diagnosed during hospital stays were included, and those up to 30 days after discharge, diagnosed during ambulatory follow-up. Patients were classified based on malignant etiology (neoplasia) and benign etiology (diverticular and inflammatory bowel disease). Different variables considered as potential risk factors for surgical infection were studied by bivariate analysis: age over 70 years, malignant etiology, diabetes, chronic renal insufficiency (serum creatinine>1.2mg/dL), hypoalbuminemia (serum albumin<3.5g/dL), obesity (BMI>30kg/m2), anemia (hemoglobin<12g/dL), concomitant steroid therapy, and chronic lung disease. Evaluated surgical variables were: surgery duration longer than 2h, administration of a second dose of intraoperative antibiotic prophylaxis, and using Vicryl Plus® for laparotomy closure.
Statistical AnalysisFor the categorical variable study, Chi-square and Fisher's exact tests were used, based on application conditions. The Mann–Whitney U test was used to analyze quantitative variables. Odds ratios were used to measure associations. The multivariate logistic regression method and the Hosmer and Lomeshow test were applied to study the relationship between dependent and independent variables.
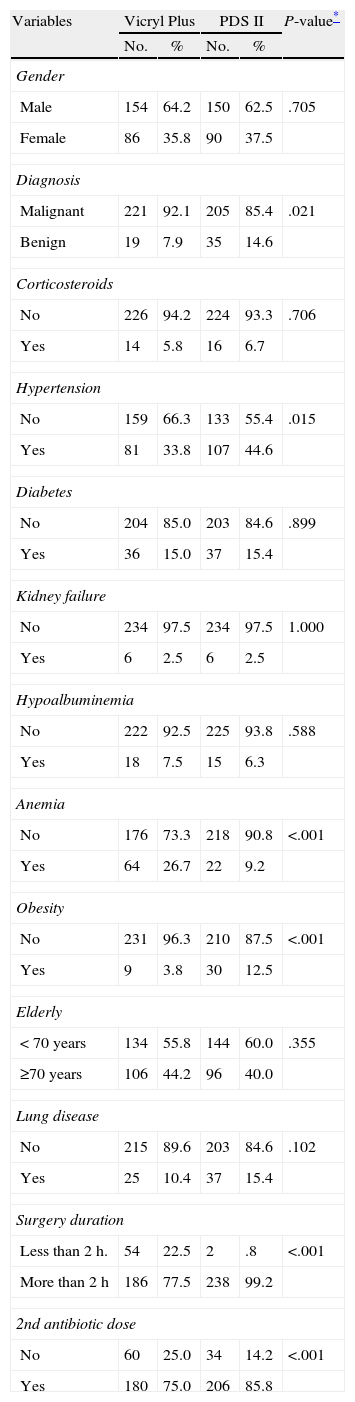
ResultsStudy Group CharacteristicsCharacteristics of patients in the 2 study groups are reported in Table 1. Average patient age for the case group was 64.2 years (18–86 year range), and 65 years for the control group (20–89 year range). Not all variables considered were homogeneous in the 2 groups. Differences were found regarding etiology, anemia, obesity, surgery duration, and administration of a second antibiotic dose at 3h. after surgery. Neoplasm was the most common etiology in both groups: 92.1% (221/240) for the case group, and 85.4% (205/240) for the control group (P=.021). 26.7% (64/240) of patients in the Vicryl Plus® group had anemia, compared to 9.2% (22/240) of the PDS II® group (P<.001). A BMI greater than 30kg/m2 was observed in 3.8% (9/240) of patients in the case group, and 12.5% (30/240) of patients in the control group (P<.001). Surgery duration was greater than 2h for 77.5% (186/240), and 99.2% (238/240) of patients, respectively (P<.001). All patients received antibiotic prophylaxis during induction of anesthesia; 75.4% (181/240) of cases in the Vicryl Plus ® group, and 85.8% (206/240) of cases in the PDSII® group, received a second antibiotic dose at 3h. after surgery (P=.004). Abdominal wall protection was applied during each surgical procedure.
Characteristics of Patients in the 2 Groups.
| Variables | Vicryl Plus | PDS II | P-value* | ||
| No. | % | No. | % | ||
| Gender | |||||
| Male | 154 | 64.2 | 150 | 62.5 | .705 |
| Female | 86 | 35.8 | 90 | 37.5 | |
| Diagnosis | |||||
| Malignant | 221 | 92.1 | 205 | 85.4 | .021 |
| Benign | 19 | 7.9 | 35 | 14.6 | |
| Corticosteroids | |||||
| No | 226 | 94.2 | 224 | 93.3 | .706 |
| Yes | 14 | 5.8 | 16 | 6.7 | |
| Hypertension | |||||
| No | 159 | 66.3 | 133 | 55.4 | .015 |
| Yes | 81 | 33.8 | 107 | 44.6 | |
| Diabetes | |||||
| No | 204 | 85.0 | 203 | 84.6 | .899 |
| Yes | 36 | 15.0 | 37 | 15.4 | |
| Kidney failure | |||||
| No | 234 | 97.5 | 234 | 97.5 | 1.000 |
| Yes | 6 | 2.5 | 6 | 2.5 | |
| Hypoalbuminemia | |||||
| No | 222 | 92.5 | 225 | 93.8 | .588 |
| Yes | 18 | 7.5 | 15 | 6.3 | |
| Anemia | |||||
| No | 176 | 73.3 | 218 | 90.8 | <.001 |
| Yes | 64 | 26.7 | 22 | 9.2 | |
| Obesity | |||||
| No | 231 | 96.3 | 210 | 87.5 | <.001 |
| Yes | 9 | 3.8 | 30 | 12.5 | |
| Elderly | |||||
| <70 years | 134 | 55.8 | 144 | 60.0 | .355 |
| ≥70 years | 106 | 44.2 | 96 | 40.0 | |
| Lung disease | |||||
| No | 215 | 89.6 | 203 | 84.6 | .102 |
| Yes | 25 | 10.4 | 37 | 15.4 | |
| Surgery duration | |||||
| Less than 2h. | 54 | 22.5 | 2 | .8 | <.001 |
| More than 2h | 186 | 77.5 | 238 | 99.2 | |
| 2nd antibiotic dose | |||||
| No | 60 | 25.0 | 34 | 14.2 | <.001 |
| Yes | 180 | 75.0 | 206 | 85.8 | |
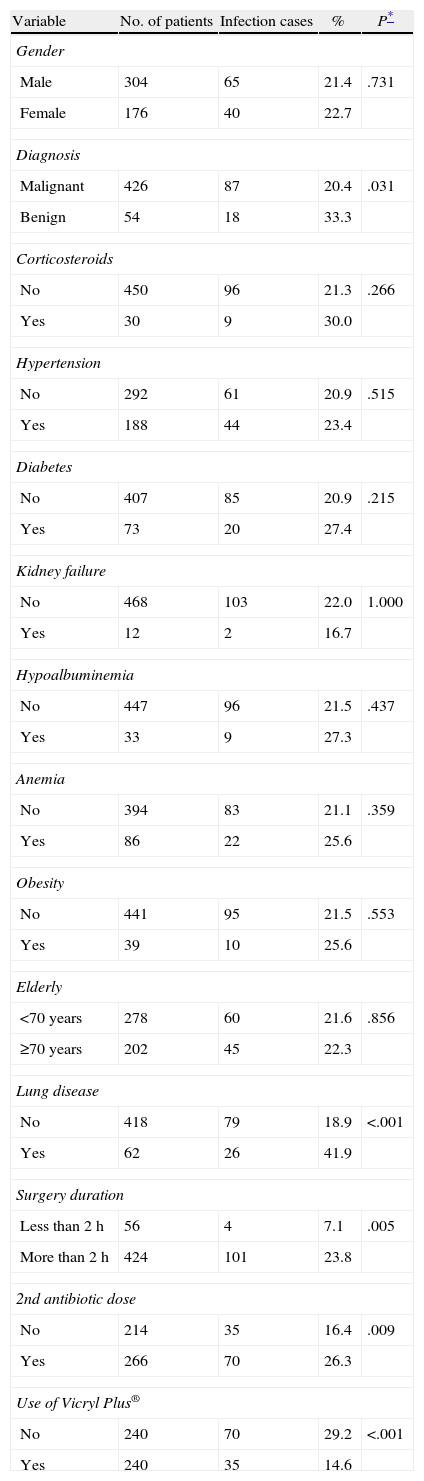
The bivariate study on different variables showed that the wound infection rate was significantly higher in cancer patients and chronic lung disease patients, if the surgery exceeded 2h, in the event that no second antibiotic dose was administered at 3h after surgery, and for laparotomy closures with conventional suture (PDS II®) (Table 2).
Variables Related to Wound Infection.
| Variable | No. of patients | Infection cases | % | P* |
| Gender | ||||
| Male | 304 | 65 | 21.4 | .731 |
| Female | 176 | 40 | 22.7 | |
| Diagnosis | ||||
| Malignant | 426 | 87 | 20.4 | .031 |
| Benign | 54 | 18 | 33.3 | |
| Corticosteroids | ||||
| No | 450 | 96 | 21.3 | .266 |
| Yes | 30 | 9 | 30.0 | |
| Hypertension | ||||
| No | 292 | 61 | 20.9 | .515 |
| Yes | 188 | 44 | 23.4 | |
| Diabetes | ||||
| No | 407 | 85 | 20.9 | .215 |
| Yes | 73 | 20 | 27.4 | |
| Kidney failure | ||||
| No | 468 | 103 | 22.0 | 1.000 |
| Yes | 12 | 2 | 16.7 | |
| Hypoalbuminemia | ||||
| No | 447 | 96 | 21.5 | .437 |
| Yes | 33 | 9 | 27.3 | |
| Anemia | ||||
| No | 394 | 83 | 21.1 | .359 |
| Yes | 86 | 22 | 25.6 | |
| Obesity | ||||
| No | 441 | 95 | 21.5 | .553 |
| Yes | 39 | 10 | 25.6 | |
| Elderly | ||||
| <70 years | 278 | 60 | 21.6 | .856 |
| ≥70 years | 202 | 45 | 22.3 | |
| Lung disease | ||||
| No | 418 | 79 | 18.9 | <.001 |
| Yes | 62 | 26 | 41.9 | |
| Surgery duration | ||||
| Less than 2h | 56 | 4 | 7.1 | .005 |
| More than 2h | 424 | 101 | 23.8 | |
| 2nd antibiotic dose | ||||
| No | 214 | 35 | 16.4 | .009 |
| Yes | 266 | 70 | 26.3 | |
| Use of Vicryl Plus® | ||||
| No | 240 | 70 | 29.2 | <.001 |
| Yes | 240 | 35 | 14.6 | |
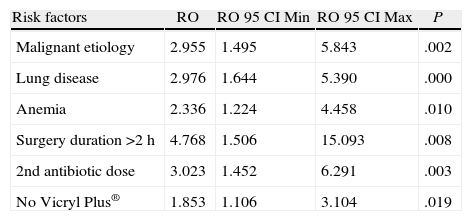
The multivariate analysis of the variables identified as potential surgical infection risk factors, and the non-homogeneous variables resulting from comparing the 2 groups, showed that the wound infection risk was 2.95 times higher in cancer patients, 2.97 times higher in chronic obstructive pulmonary disease patients, 2.33 times higher in anemia patients, 4.76 times higher if surgery exceeded 3h, 3.02 times higher if no second antibiotic dose was administered during surgery, and 1.85 times with conventional suture compared to Vicryl Plus® (Table 3).
Multivariate Analysis: Factors Related to Surgical Infection.
| Risk factors | RO | RO 95 CI Min | RO 95 CI Max | P |
| Malignant etiology | 2.955 | 1.495 | 5.843 | .002 |
| Lung disease | 2.976 | 1.644 | 5.390 | .000 |
| Anemia | 2.336 | 1.224 | 4.458 | .010 |
| Surgery duration >2h | 4.768 | 1.506 | 15.093 | .008 |
| 2nd antibiotic dose | 3.023 | 1.452 | 6.291 | .003 |
| No Vicryl Plus® | 1.853 | 1.106 | 3.104 | .019 |
The overall wound infection rate after wall closure with Vicryl Plus® was significantly lower compared to closure with PDS II1. Eleven cases of infection (31.4%) were diagnosed after hospital discharge.
Patients who suffered wound infections had longer hospital stays than patients who did not: 21.2 compared to 9.7 days (P<.001). However, for cases of wound infection, the average stay of patients in the Vicryl Plus® group was significantly lower than for those in the PDS II® group (Table 4).
DiscussionIn this study, the authors wanted to evaluate the impact of several risk factors for wound infection in elective colorectal surgery, with special emphasis on the influence of the suture material used for laparotomy closure. Short-medium absorption suture such as Vicryl Plus® was used, rather than long-absorption monofilament suture, due to the fact that it was the only available triclosan coated suture at the time of the study.
Various research projects have studied triclosan's antibacterial activity, in vitro and with animals.15–19 Other studies tested biocompatibility and safety of triclosan-coated 910 Polyglactil for clinical use.14,21 Ford et al. demonstrated the efficacy of Vicryl Plus® in pediatric patients with a randomized clinical trial.22 A systematic review published in 2012 showed no significant differences between Vicryl® with and without triclosan, considering a large sample of 836 patients derived from a pooled analysis of 7 randomized studies.23 Moreover, a subsequent meta-analysis with greater statistical power, including 17 randomized studies, showed a significant benefit from triclosan-coated sutures in clean-contaminated abdominal surgery and in adult patients.24 Nakamura et al. have recently published a randomized prospective study on the effects of Vicryl Plus® on elective colorectal surgery, demonstrating a significant decrease in the rate of surgical infection compared to patients where Vicryl® without triclosan was used, 4.3% compared to 9.3%.25
One of the limitations of this study is related to the characteristics of the patients. Some of the variables were significantly different for the comparative analysis of the 2 groups. These differences are probably due to the fact that they are 2 consecutive series of patients. To reduce the influence of this bias on study results, a multivariate analysis was performed to determine the influence of variables potentially involved in surgical site infection.
In our experience, patients treated with Vicryl Plus® had a 14.6% wound infection rate, significantly lower compared to 29.2% for the group treated with PDSII®. In a 2009 prospective study comparing Vicryl Plus® to PDSII®, Justinger et al. reported a significantly lower wound infection rate using Vicryl Plus®: 4.9% compared to 10.8%.26 However, the study included non-homogeneous patients due to the inclusion of different procedures, surgery contamination degree and surgical setting: hepatobiliopancreatic, intestinal, colorectal, vascular surgeries, as well as elective and emergency surgeries. In this study, the derivative impact of using Vicryl Plus® was evaluated, specifically in elective colorectal surgery on a series of 240 consecutive patients prospectively included. In order to increase the significance and consistency of the results, a control sample of patients was considered; they were included based on the same patient inclusion criteria in the group of interest; patients in the control group were treated with laparotomy closure using PDSII®, because it is a very commonly used suture and conventionally used by surgeons belonging to the group of authors.
Eleven wound infection cases were diagnosed after hospital discharge. According to the results of a study by Smith et al., 49% of the wound infections in the patients included were diagnosed after discharge.4 The reason for the lack of consistency in the results in the literature may lie in the different system used to record wound infections; probably, the series with higher infection rates also include cases observed after hospital discharge.
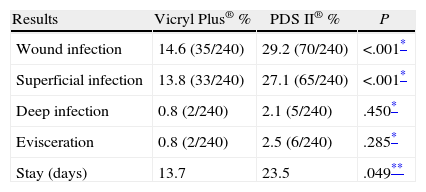
In this study, the bivariate analysis showed that using Vicryl Plus® produced a significant reduction in wound infections, with a 14.6[%] rate, compared to 29.2% when using PDSII®.
However, the risk of infection was also found to be associated with other factors such as cancer, chronic pulmonary disease, surgery duration exceeding 2h, and no administration of a second prophylactic antibiotic dose at 3h. after surgery. For that reason, and because of the incomplete homogeneity of the 2 study groups, we applied a multivariate analysis; using Vicryl Plus proved to be a useful independent preventive measure; the risk of wound infection being 1.85 times higher in patients treated with polydioxanone suture. Other factors such as neoplastic etiology, chronic lung disease, anemia, surgery duration exceeding 2h, and failure to administer an additional antibiotic prophylaxis dose at 3h. after surgery were also associated with increased infection risk.
An important finding was the significant difference in hospital stay between patients with wound infections in the group treated with Vicryl Plus® compared to patients with infections in the control group: 13.7 and 23.5 days, respectively. This result suggests the possibility that the bacteriostatic effect of triclosan favors less colonization of the suture material by the microorganisms, therefore allowing for faster response to the medical treatment of the infection.
Given that this study is non-randomized, it is limited to highlighting the differences in results in terms of wound infection, comparing the use of Vicryl Plus® and PDSII®.
The results shown indicate that using 910 Polyglactil with triclosan in clean-contaminated surgery, such as elective colorectal surgery, helps reduce abdominal wall infection rate, and consequently, hospital stays and healthcare costs. Additional randomized studies are needed to corroborate our findings (Fig. 1).

Please cite this article as: Fraccalvieri D, Kreisler Moreno E, Flor Lorente B, Torres García A, Muñoz Calero A, Mateo Vallejo F, et al. Factores predictivos de infección de herida en cirugía colorrectal. Estudio observacional multicéntrico de casos y controles. Cir Esp. 2014;92:478–484.
