



To describe and test a practical protocol to measure common carotid intima-media thickness that uses the combined values of two longitudinal examination angles to increase sensitivity.
METHODBetween February and September 2005, 206 patients underwent duplex scan examination of carotid vessels, and the intima-media thickness of 407 common carotids were measured in three angles: transversal, longitudinal posterolateral, and anterolateral, with three intima-media thickness measurements for each near and far wall. In addition to numbers obtained from the three angles of measurement, a fourth visual perspective was obtained by combining the intima-media thickness results of posterolateral and anterolateral longitudinal views and considering the thickest wall measurement.
RESULTSTwo hundred seventy (66.3%) carotid arteries had an intima-media thickness thicker than 1mm. The mean intima-media thickness values achieved by the different incidences were 1.26±0.6mm (transversal), 1.17±0.54mm (longitudinal anterolateral), and 1.18±0.58mm (longitudinal posterolateral). A significant difference in intima-media thickness measurement values was observed when the three angles of examination plus the combined positive results of both longitudinal angles were compared by ANOVA (P=0.005). The LSD Post-Hoc test determined that the combined longitudinal view results were similar to the transversal views (P=0.28) and had greater intima-media thickness means than isolated anterolateral or posterolateral longitudinal views (P=0.02 and 0.05, respectively).
CONCLUSIONSThe protocol presented is a practical method for obtaining common carotid artery intima-media thickness measurements. The combined longitudinal posterolateral and anterolateral longitudinal views provide a more sensitive evaluation of the inner layers of the carotid walls than isolated longitudinal views.
The measurement of the common carotid artery intima and media combined layers as determined by high-resolution B-mode ultrasonography is now widely recognized as a useful tool for early identification for systemic atherosclerosis. Intima-media thickness (IMT) evaluation can identify individuals at risk for future cardiovascular events,1–7 and also evaluate the effectiveness of different therapy modalities for controlling morbidities that lead to the development of atherosclerotic-based diseases by identifying regression in IMT values after such interventions.8–13
IMT measurement methods have become more complex since the initial reports. The necessity of same-patient serial measurements in prospective cohort studies demanded a homogenization of the technique in order to avoid differences between repeated exams due to technical reproducibility difficulties as opposed to real IMT changes. Also, a uniform technique would prevent significant measurement differences between different observers. However, complex models require longer examination periods, are more expensive, and require auxiliary devices and additional human resources.
The objective of this study was to test and describe a practical protocol to measure common carotid IMT that uses the combined values of two longitudinal examination angles to increase its sensitivity.
METHODBetween February and September 2005, 210 patients underwent duplex scan examination of carotid vessels at our institution. Generally, the indication for carotid investigation was the occurrence of a neurological event (stroke, TIA, or both), assessment of cardiovascular status in patients with risk factors for atherosclerosis, and preoperative evaluation for vascular surgeries. Four patients performed examinations due to carotid trauma, and were excluded. The remaining 206 patients were evaluated in a cross-sectional study where conventional carotid and vertebral duplex investigation was complimented by IMT measurements taken from both common carotid arteries (CCA), except in five cases due to unilateral CCA occlusion. All examinations were performed by a single physician with certified skills in duplex scan diagnostic procedures. The exams were initially performed with an ATL HDI 1500 ultrasound system (Phillips Medical Systems, Bothel, WA, USA) using a 10–12 MHz linear transducer. In the latter included patients, a Logiq 5 ultrasound system (GE Healthcare, Milwaukee, WI, USA) and a 7–10 MHz linear transducer were used.
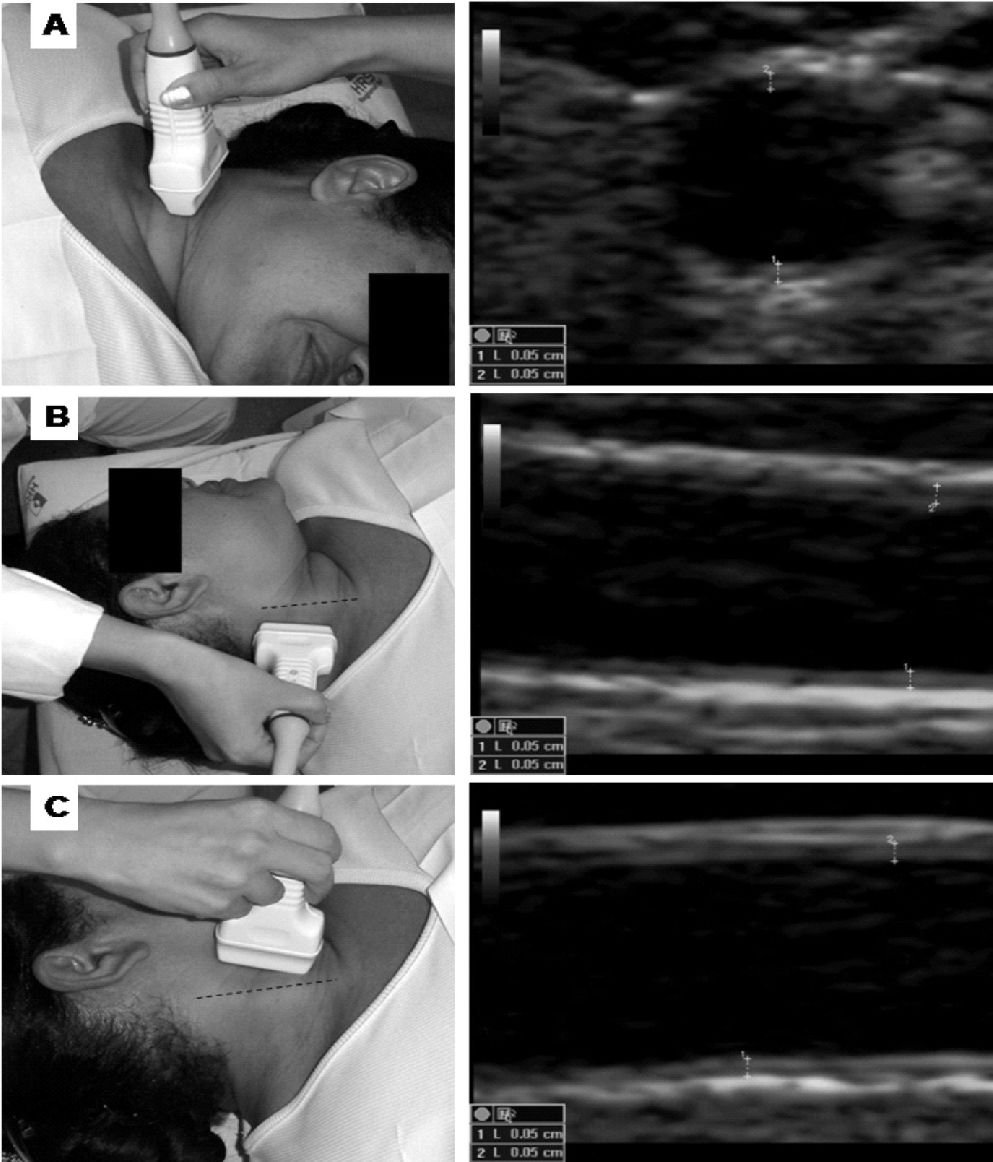
Technique DescriptionIMT measurements were obtained with the patient lying in the supine position and with the neck rotated to the opposite side of examination. CCA images were obtained to measure IMT by using three different angle views for each vessel (Figure 1). Initially, a transversal scanning view of the ACC was performed in the longest extension possible from the base of the neck to the carotid bulb. At least three IMT points were measured in the near and far walls in the most thickened area of each vessel. Also, lateral wall measurements were taken when both thickening was evident and accurate images were possible. Subsequently, the vessel was scanned by two longitudinal views: posterolateral (PL), with the transducer positioned parallel to the posterior border of the sternocleidomastoid muscle, and anterolateral (AL), with the transducer positioned parallel to the anterior border of the sternocleidomastoid muscle; at least three IMT measurements were obtained for each near and far wall. Optimal B-mode settings of gain, depth, focal zone placement, and compression were individually adjusted for each vessel to enhance arterial wall structures and image quality. IMT was measured by manual technique using electronic calipers, similar to the method of Sidhu and Desai.14 The maximum IMT value was selected for each angle. An IMT superior to 1.0mm was considered to be an abnormal finding.15

Quantitative IMT measurement differences between the different angles were calculated by ANOVA with the LSD post-hoc test. Qualitative differences were calculated by McNemar’s test. A level of significance was defined as a P< .05.
RESULTSThe population studied had a mean age of 60.8±12.9 years, and 106 (51.5%) of the individuals were male. Four hundred seven CCAs were evaluated. Reliable measurement images could be achieved in 406 vessels in the transversal angle view, 404 in the longitudinal posterior view, and 398 in the longitudinal anterior angle view. The mean time necessary to take measurements was 8.1±1.24 minutes.
Comparing the thickest measurement obtained from all views, 270 (66.3%) carotid arteries had an IMT greater than 1mm. The mean IMT values achieved with the different incidences were 1.26±0.6mm (transversal), 1.17±0.54mm (longitudinal AL), and 1.18±0.58mm (longitudinal PL). Detailed data of mean IMT for each angle view are presented in Table 1.
General measurement data showing mean values of intima-media thickness (IMT) and the distribution of common carotid arteries (CCA) divided by angle of view and groups of normal and thickened vessels. Combined views represent the thickest measurement obtained from the two longitudinal views
| View | Mean intima-media thickness (mm) | Distribution of CCA in units (%) | |||
|---|---|---|---|---|---|
| General | IMT up to 1.0mm | IMT > 1.0mm | IMT up to 1.0mm | IMT > 1.0mm | |
| Longitudinal AL | 1.174±0.542 | 0.764±0.129 | 1.387±0.553 | 190 (47.7) | 208 (52.3) |
| Longitudinal PL | 1.186±0.583 | 0.75±0.14 | 1.412±0.597 | 197 (48.4) | 207(50.9) |
| Combined AL/PL | 1.306±0.618 | 0.811±0.119 | 1.554±0.61 | 159 (39.2) | 247 (60.8) |
| Transversal | 1.257±0.602 | 0.736±0.151 | 1.526±0.57 | 154 (37.9) | 252 (62.1) |
AL, anterolateral; PL, posterolateral.
A significant difference in IMT measurement values was observed when the three angles of examination plus the combined positive results of both longitudinal angles were compared by ANOVA (P=0.005). The LSD Post-Hoc test identified that the combined results of longitudinal views had similar results to transversal views (P=0.28) and higher IMT means than isolated AL or PL longitudinal views (P=0.02 and 0.05, respectively).
A direct comparison of the different angles of measurement was obtained with McNemar’s test. No statistical difference was observed in comparison between AL and PL longitudinal angles (P=0.63). The transversal view identified a greater number of arteries with increased IMT in comparison to the anterior or posterior longitudinal examination angles (P<0.001 for both). The combined results of the two longitudinal angles show superior results over isolated longitudinal views (P<0.001 for both) and similar results to transversal measurements (P=0.52). These data are detailed in Table 2.
A direct comparison of the accuracy of the combined positive results of longitudinal views with the accuracy of the isolated transversal and longitudinal measurement angles– number of common carotid arteries with increased intima-media thickness (>1mm)
| Combined positive results of longitudinal views | P | |||
|---|---|---|---|---|
| Normal | Increased IMT | |||
| Longitudinal | Normal | 155 | 34 | <0.001 |
| anterolateral | Increased IMT | 00 | 208 | |
| Longitudinal | Normal | 158 | 39 | <0.001 |
| posterolateral | Increased IMT | 00 | 207 | |
| Transversal | Normal | 137 | 17 | 0.522 |
| Increased IMT | 22 | 229 | ||
IMT measurement is a simple, feasible, and cost-effective method for assessing systemic atherosclerosis and cardiovascular risk in adults.1 Also, is somewhat easy to provide specific training for professionals with previous vascular ultrasound experience to take IMT measurements that meet good quality standards after a short period of practice.14 In this study, we proposed an objective and practical method to evaluate IMT with the intention of improving the measurement quality by a short increase in the time required for carotid examination while maintaining its characteristic simplicity.
Recent protocols for determining carotid IMT include a series of sophisticated features. Specific software16–20 has been developed for automatic IMT evaluation that minimizes the subjectivity of direct eye observation. Computer-assisted IMT measurements are widely used in other countries for longitudinal cohort studies and are encouraged by latest consensus.21–22 However, such an option demands complex human and material resources. Although software can perform more than a hundred measurements from each segment in a short time, the results obtained were not proven to be more accurate than manual measurements.23
Another improvement is the concomitant use of ECG24 during examination, which allows the observer to take measurements only during systolic activity, preventing small differences that could appear during the diastolic period when the inner arterial layers are less compressed. Also, external devices that measure head rotation and transducer position in degrees, such as the Meijer Arc, make it possible to reproduce the same positions in repeated examinations. These improvements bring many advantages and raise the quality of the data obtained, but such procedures also require more time24 and are more expensive. The application of such protocols should be preceded by a careful cost-benefit analysis that depends on the objectives of each investigation.
We also avoided the use of external devices for probe positioning. Only the sternocleidomastoid and the carotid bulb were used, which represent simple anatomical references that remain virtually unchanged over time.
The transversal angle view provided a panoramic observation of the CCA, thus allowing the observer to identify and measure the thickest IMT points, even of the side walls. However, measurements taken from the transversal view may result in poor quality images, which are subject to many artifacts that are mainly the result of refraction from the side walls. Rather than being a proper measurement angle, the transversal view is useful as a screening image to guide longitudinal view measurements.
Previous authors have performed IMT measurements from a single longitudinal view,14,25–26 which can provide limited observation of the vessel walls, leading to the underestimation of early atherosclerotic processes. We avoided directly comparing our findings with these reports due to the methodological differences of each study. Instead, we used the numbers obtained in our investigation to compare the combined results of IMT measured from the two longitudinal views with results from each single longitudinal view. As shown in the results, isolated longitudinal views had poorer sensitivity on identifying areas of increased IMT. The longitudinal views obtained in this investigation provided at least 12 different measurement points (three from each wall), covering the whole extension of the CCA in perpendicular angles to generate virtual tri-dimensional information about carotid wall thickness.
Although some authors believe that the near wall images are not accurate enough for IMT measurements,27–28 we decided to consider these values. In many cases, the near wall presents layers that are far thicker than those in the far wall, which may even have normal values. Thus, ignoring these findings would underestimate the real state of the carotid artery atherosclerotic process.29–30
Recent studies revealed a tendency to use the mean maximum thickness of the CCA, carotid bulbs, and internal carotid artery (ICA).31 In this investigation, we avoided taking measurements from the carotid bulb or ICA for the following reasons: First, even though bulb and ICA measurements may be worthwhile, they present limitations: as opposed to CCA, they can be measured only in limited angles that may not reflect the thickest portions of vessel wall.32–33 Also, up to 52% of images can fail to obtain accurate bulb and ICA measurements.34 The variance of results of bulb and ICA IMT amongst repeated examinations and different physicians is higher than CCA measurements, making longitudinal comparisons more unreliable.35–37 Finally, CCA, bulb, and ICA have morphological differences that make direct IMT comparison among them inaccurate.21 Yet, CCA/bulb/ICA measurements do not appear to be superior to CCA IMT alone.38
We believe that the suggested protocol is an inexpensive method to measure IMT. We avoided expressing costs in numbers because values may vary from country to country and from private to public healthcare models. Thus, the eventual cost calculation in our institution may not reflect the reality for many readers.
Although we did not show numbers to confirm our impression, we judged that the presented technique is less expensive because it does not uses complimentary devices and does not depend on external software to analyze the obtained images. Human resources would be required to deal with ancillary equipment. The acquisition and maintenance of the necessary devices would certainly impact the final costs of examinations. The mean time expended in taking all measurements was about 8 minutes. This value is shorter than other models suggested,24 thus representing less of an impact in terms of physician human resources than more complex models.
CONCLUSIONThe protocol presented is a fast and practical method for obtaining common carotid artery intima-media thickness measurements. The combined values of anterolateral and posterolateral longitudinal views provide a more sensitive evaluation of the inner layers of the carotid walls than isolated longitudinal views.