






Description of clinical and epidemiological characteristics of patients who underwent surgery for oral cancer in a Medical School Teaching Hospital, and determination of differences with respect to other institutions and/or periods of time.
METHODThe charts of patients undergoing surgery for oral cancer from 1994 to 2002 were reviewed. Data were collected in a spreadsheet in order to analyze clinical and epidemiological features..
RESULTSA total of 374 patients having undergone 406 operations was identified. Their ages varied from 14 to 94 years (mean = 57.4 years), with 255 men (68.2%), and 295 out 366 Caucasian (80.6%). A majority had tumors of the tongue and/or floor of mouth (55.6%), while 20.3% had lip cancer. Squamous cell carcinoma was found in 90.3%, and glandular carcinoma in 4%. T4 tumors in 39.6%, Tis or T1 lesions in 15.2% of all patients. Nearly 62% had no regional metastases, and the relative incidence in young patients (40 years or younger) reached 8.6%.
CONCLUSIONIn spite of the predominance of locally advanced tumors, a majority of patients had no neck metastases. The 31.8% incidence in females indicates an increasing incidence of oral cavity cancer among women when compared to previous periods at the same institution.
Caracterizar epidemiológica e clinicamente a população atendida por câncer de boca em hospital-escola de atenção terciária e quaternária e verificar variações em relação a outras casuísticas e períodos.
MÉTODOSProcedeu-se à revisão dos prontuários dos operados por câncer oral de 1994 a 2002. As características clínicas e epidemiológicas foram colocadas em planilhas e analisadas.
RESULTADOSForam identificados 374 portadores de câncer da boca que foram submetidos a 406 operações. A idade dos doentes variou de 14 a 94 anos (média = 57,4 anos). Duzentos e cinqüenta e cinco eram do gênero masculino (68,2%). Duzentos e noventa e cinco entre 366 doentes eram caucasianos (80,6%). A maioria era portadora de tumores da língua e/ou do soalho da boca (194 entre 349 doentes; 55,6%), e 71 (20,3%) tinham tumores dos lábios. O carcinoma epidermóide foi encontrado em 90,3% e carcinomas glandulares em 4%. Os tumores T4 estavam presentes em 39,6% dos doentes; 15,2% tinham lesões Tis ou T1. Quase 62% dos pacientes não tinham metástases cervicais. A incidência relativa em jovens (com até 40 anos de idade) atingiu 8,6%.
CONCLUSÃOApesar dos achados freqüentemente referidos na literatura terem se confirmado (como o predomínio de lesões avançadas localmente), a maioria dos doentes não apresentava metástases cervicais. Acima do observado em outras casuísticas, os 31,8% de mulheres na presente casuística indica a preocupante e crescente incidência no gênero feminino.
Cancer of the oral cavity represents 2.6% of all malignancies affecting the Brazilian population according an estimate from the Brazilian National Cancer Institute (INCa) for 2003. Oral cancer is the eighth most common cancer in Brazil and occupies the sixth place when only men are considered. Regarding mortality, a total of 2.8% of deaths by cancer was due to malignancies in the mouth, which places oral cancer in the ninth place for mortality among all malignant tumors.1
Despite this marked importance of oral cancer, its main risk factors, namely the tobacco smoking and alcohol consumption, are well known and may be avoided.2,3,4 In addition to being primarily preventable through through avoidance of these risk factors, oral malignancies may be diagnosed in early stages with no major difficulties, making these tumors also suitable to secondary prevention. In fact, the oral cavity may be easily examined by health care professionals such as doctors, dentists, nurses, and speech therapists.5 The individual may personally conduct an auto-examination5 (during the morning oral hygiene, for example).
In spite of the relative ease of mouth examination, the systematic examination of the oral cavity by health care professionals and oral auto-examination have not been routinely and widely employed and have received little attention from both professionals and patients. As a result, advanced cancer predominates in the services of Head and Neck Surgery, Dermatology, Oncology, and Dentistry in hospitals of tertiary and quaternary attention where most patients have their diagnosis of oral cancer.3,4,6,7 The treatment of advanced head and neck cancer including oral cancer is carried out in Head and Neck Surgery and Oncology services and will have worse results in terms of survival, function, and cosmesis when compared to results obtained after treatment of initial disease.8–12
Regarding oral cancer in its initial presentations, it seems to be more reasonable (both in terms of diagnostic and therapeutic approaches) to determine which are the individuals and/or populations most frequently affected in order to delineate strategies for secondary prevention. It also appears that a strategy for primary prevention (such as spreading information about the need to avoid the main risk factors) allows health professionals and individuals at risk to be more cautious about the disease and, consequently, contributes to the diagnosis of oral cancer in early stages.
The aim of the present study is to describe clinically and epidemiologically the population of patients who underwent surgery for oral cancer in our service from 1994 to 2002, and to determine whether there are differences when the profile of this group of patients is compared to other series from the same service in previous periods and to other tertiary and quaternary attention institutions in 2 major Brazilian cities. Our service is responsible for the treatment of patients coming from the entire country with cancer of the oral cavity at any stage, including patients who require high complexity treatment modalities.
PATIENTS AND METHODSThe charts of all patients undergoing surgery for oral cancer from 1994 to 2002 were retrospectively reviewed. Some of them underwent other treatment modalities preoperatively or postoperatively. Demographics (age, gender, and ethnicity), habits (tobacco smoking and alcohol consumption) and clinical data (symptoms, duration of symptoms, location of the tumor, histologic type, TNM stage, and pTNM stage) were collected in a spreadsheet and analyzed.
RESULTSFrom 1994 to 2002, 374 patients with oral cancer underwent 406 surgical procedures. Their ages varied from 14 to 94 years (mean = 57.4 years). Only 8.6% of patients were 40 years old or younger. There were 119 (31.8%) women. A total of 295 (80.6%) patients were Caucasians.
Regarding habits, tobacco smoking was identified in 202 of 250 patients (80.8%). Alcohol consumption history could be retrieved in 138 of 244 patients (56.6%).
The period of time between the appearance of the first symptoms to the first visit to the Service varied from 10 days to 20 years. The mean duration of symptoms was 14.1 months. The most frequent symptoms were the presence of a lesion in the mouth and local pain (Table I).
Prevalence of symptoms at the time of diagnosis/treatment
| Symptoms | n = 305 | Prevalence |
|---|---|---|
| Oral lesion | 268 | 87.9% |
| Oral pain | 108 | 35.4% |
| Weight loss | 40 | 13.1% |
| Enlarged neck node | 29 | 9.5% |
| Bleeding | 17 | 5.6% |
| Dysphagia | 14 | 4.6% |
| Odynophagia | 9 | 2.9% |
| Otalgia | 8 | 2.6% |
| Trismus | 8 | 2.6% |
| Halitosis | 7 | 2.3% |
| Loss of tongue mobility | 5 | 1.6% |
| Sensation of foreign body | 3 | 1.0% |
| Pruritus | 1 | 0.3% |
Squamous cell carcinoma was found in 317 of 351 patients (90.3%). Glandular carcinoma (adenoid cystic carcinoma, adenocarcinoma and mucoepidermoid carcinoma) was found in 14 individuals (4%), and verrucous carcinoma in 4 (1.1%).
The most frequent sites of the primary tumors were the tongue, the floor of the mouth, and the lips. Figure 1 shows the distribution of patients according to the site of the primary tumor.
. Synchronous refers to 2 or more tumors (1 in the oral cavity and another in any site of the upper aerodigestive tract)")
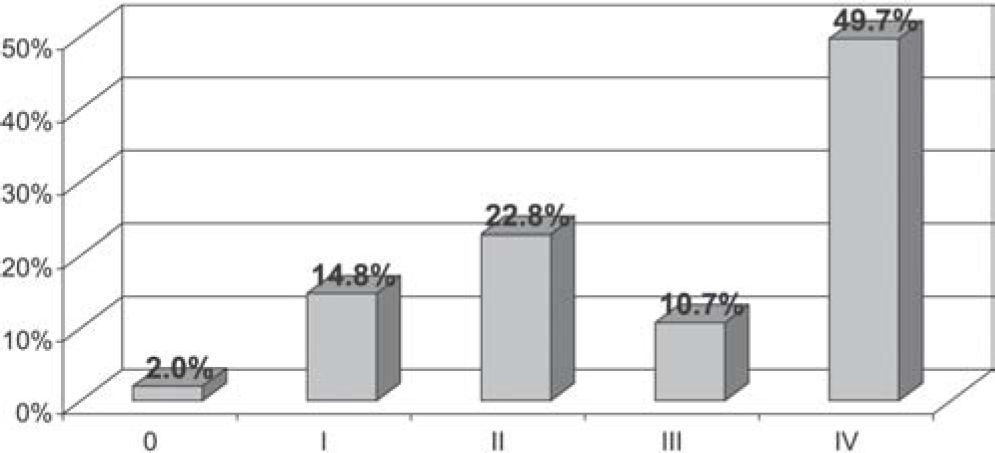
Regarding the stage of disease, the majority of the patients had advanced local disease. T4 lesions were found in 39.6%. Prior to the pathology report, 153 of 298 patients (51.3%) were classified in stage IV according to the TNM Classification, and only 14.5% were classified as having stage 0 or I disease. After the macroscopic and microscopic pathologic study, 16.8% were classified in stages 0 and I. The majority of patients (61.6%) did not present regional metastases. Figures 2, 3, and 4 illustrate the distribution of patients according to T classification, TNM stage, and pTNM stage.
")
")
")
During the 9-year period of this study, 374 patients underwent surgery for oral cancer (average of 41.5 cases per year).
In 1998, Araujo Filho et al.6 reported 54 patients operated on for oral cancer at the same institution during a period of 10 years. Kawata13, in 2004, analyzed retrospectively 141 records of patients with mouth cancer admitted for surgical treatment between 1985 and 1997, also in the same service. These data reveal an evident increase in the number of cases of oral cancer undergoing surgery in our service during recent years. In another tertiary service in the same city, Fardin et al.14 reported 1,440 mouth cancer patients seen between 1977 and 1998 (average of 65.5 cases/year). This greater incidence in their institution may be explained by the inclusion in their series of patients that had never undergone surgical treatment. Barbosa et al.15 published a study from Hospital do Cancer of the INCa, in Rio de Janeiro, with 258 patients treated between 1975 and 1980 (average 43 cases/year) representing a tertiary service in that city. Analyzing these reports, we conclude that close to 40 or 50 patients are treated in main Brazilian specialized head and neck services every year.
The most frequent age at presentation was between 50 and 60 years, which underwent no significant variations over time in our service. In the study by Barbosa et al.,15 the highest incidence occurred between 40 and 50 years. Although Fardin et al.14 did not publish the average age at presentation, 52% of their patients were between 50 and 65 years of age. Young patients were considered to be those 40 years of age or less and comprised 8.6% of all individuals in our series.
The fact that oral cancer affects many more men than women may be observed in all series from western countries2,4. In the present study, 31.8% of all patients were women. Araujo Filho et al.6 and Fardin et al.14 found less than 20% women in their series. Barbosa et al.15 reported 26.4%, and Kawata13 25.5% women in their studies. All of these 4 studies were carried out some time ago, 2 of them6,13 being from our service. This suggests that we have had a relative increase in the incidence of oral cancer in women, at least in our hospital. The percentage of women reported in the present paper is uncommonly high if compared not only with the above mentioned studies, but also to the 27.1% estimation for Brazilian women for the year 2003.1 This increase is attributed by most authors to the increasing number women who smoke in the general population2,4. In addition, this increase of smoking has led women to develop more smoke-related diseases/conditions in recent decades. In 2004, Kazerouni et al. found an increase of 382% in mortality for chronic obstructive pulmonary disease in North-American women between 1968 and 1999 much more compared to the increase of 27% in men. In addition, the authors observed the same tendency in the mortality for lung cancer: an increase of 266% in women versus 15% in men.16 There is also evidence that women are more susceptible to the effects of smoking than men, at least regarding oral17, lung17 and bladder18 cancers.
Caucasians comprised 80.6% of our patients. This is comparable to 82.6% found by Kawata13 and 88% of Caucasians and Asians reported by Fardin et al.14 in their studies, which were also carried out in the city of São Paulo. However, differentiation according race seems to be of little relevance in the studied population because there is great race miscegenation in the Brazilian population, thus turning race definition into a quite subjective exercise by the physician. Nevertheless, the data suggest a predominance of oral cancer in Caucasians. In this series this may be also explained by the inclusion of lip cancer in the study population. Lip cancer has a marked predominance in Caucasians and is associated with exposure to solar irradiation.
Considering the medical records analyzed, lifestyle habits were registered in only 70%, indicating that the 2 main risk factors for mouth cancer were often ignored by physicians. Smoking was observed in 80.8% of our cases for which lifestyle habits were recorded. Araujo Filho et al.6 found 88.9% smokers, and Kawata13 reported 82.3% smokers, both data from our service. Fardin et al.14 and Barbosa et al.15 also reported 88.2% and 89.9% smokers, respectively. This shows that smoking is the most marked risk factor in any sample of mouth cancer patients. Alcohol consumption was observed in 56.6% of our cases, while Araujo Filho et al.6 reported 65%, Kawata13 53.2%, and Fardin et al.14 75%. Barbosa et al.15 reported 60.5% of smokers and alcohol beverage consumers in their series. These data suggest that alcohol consumption is a frequent habit of oral cancer patients, but less prevalent than smoking. The literature shows the extensive relationship between smoking and drinking, probably acting in synergism, with mouth cancer incidence. However, we found that only 70% of the charts had a reference to the patient's lifestyle habits, in spite of the fact that recording them is absolutely imperative and of major importance for adequately characterizing the sample and the exposure of patients to the main external risk factors.
Regarding the complaints, oral lesion (87.9%) and local pain (35.4%) were the most frequently reported symptoms. Fardin et al.14 reported the main complaints as “lesion in the mouth” in 46% and pain in 18%. Duration of symptoms before diagnosis averaged of 14.1 months, which is higher than that observed by Araujo Filho et al.6 from our service, who reported less than 6 months duration of symptoms in 50% of that sample. A total of 79.6% of all patients in that series had less than 1 year of symptoms. Fardin et al.14 reported a duration of symptoms prior to diagnosis of 6.3 and 9.1 months on average, depending on the anatomic site of the tumor. In Rio de Janeiro, Azevedo et al.19 found an average of 6 months of symptoms before diagnosis in 170 patients seen for oral and oropharyngeal cancer between March 1994 and September 1995. These data show that the average duration of symptoms before diagnosis in our service is high and is increasing through time. Since it is well know that a long duration of symptoms is related to a worse prognosis (because it is closely related to the stage of disease), every effort should be employed in primary and secondary prevention, the latter aiming to reduce the time to diagnosis and treatment. Professionals and affected individuals must receive information aimed at making them more conscious of the risk of oral cancer in order to involve the head and neck surgery and oncology services earlier in the development of treatment.
In the present series, 55.6% of patients had cancer of the tongue and floor of the mouth, outnumbering other oral anatomic sites (lips, hard palate, retromolar area, superior and inferior alveolar ridge, and buccal mucosa). Fardin et al.14 found 71.8% and Kawata13 reported 80.2% tumors of the tongue and floor of mouth. However, these authors did not include lip tumors in their studies, which represented 20% of tumors in this series. Squamous cell carcinoma was the most frequent histologic type, and was present in 90.3% of all specimens obtained from patients included in this study. Glandular carcinomas were found in 4% of them. All these numbers agree with other Brazilian4,20 and with foreign21,22 studies.
Local advanced disease was more frequent than initial disease (39.7% for T4 versus 15.2% for T1 plus Tis). Similarly, 51.3% of mouth cancer patients were clinically classified in stage IV according to TNM Classification. After surgery and histopathology analysis, 49.7% of all patients were classified as stage IV (pTNM Classification). These numbers show that half of all patients, demanded aggressive treatment and a multidisciplinary approach. Despite all efforts, oncologic, aesthetic, and functional results after treating this subgroup were usually poor, especially when compared to those obtained in patients with initial disease. The evaluation of these results is beyond the scope of this paper (which aims essentially to characterize our patients). The results presented in this study are comparable to other series in major Brazilian cities. Fardin et al.14 reported 57% of their patients with stage IV disease in a sample from the same population of São Paulo. Barbosa et al.15 observed 40.7% patients with stage IV disease in Rio de Janeiro. Taking these figures into account, it is important to reinforce the urgency of making efforts directed to secondary prevention strategies in order to diagnose and treat oral cancer at earlier stages, thus achieving better prognosis and quality of life for patients.5,12
In contrast to the large percentage of patients with advanced disease, patients with initial disease (Stage 0 and I) comprised 15.2% in the present series, which was higher than the numbers from Fardin et al.14 and Barbosa et al.15, who reported 6% in São Paulo and 4.3% in Rio de Janeiro, respectively. In our institution, the number of patients with initial oral cancer has been increasing with time.6,13,20 This can be explained by the formation (in 1995) of a student enrolling organization devoted to the prevention and treatment of oral cancer in the São Paulo University School of Medicine teaching Hospital where our service is located. Additionally, we receive referrals from an organization founded to study buccal neoplasias at the School of Dentistry in the same University.3,7 The aim of these organizations may have been partially achieved, since some oral cancer patients have apparently had an earlier access to medical assistance than in the past.
Considering that squamous cell carcinoma (found in 90.3% of our patients) tends to spread to regional lymph nodes,4,6–11 it is amazing that 61.1% of them did not have regional metastases (N0), confirming previous reports from our service.6,20 The absence of regional metastases is a positive prognostic factor and is associated with a decrease of 50% in mortality. Carvalho et al.23 reported 50.1% N0 necks in another large series from a tertiary hospital in São Paulo. This seems to be a low incidence considering the large number of patients with local advanced disease. Some authors do not detail the incidence of regional metastases in their papers, merely reporting the TNM staging.
CONCLUSIONThe profile of patients with oral cancer in our service is similar in several aspects to those presented by other investigators in Brazil and abroad. There is a marked predominance of men and Caucasians around the fifth and sixth decades of life. Also, there is a predominance of tobacco users, and more than half of the patients have an alcohol intake history. Regarding the tumors, squamous cell carcinoma is the most frequent histologic type. The most frequent sites are the tongue and the floor of the mouth.
The sample of patients in this study presented some differences to those of other studies, including the high and increasing incidence of oral cancer in women and the low incidence of regional metastases (even with the marked predominance of advanced local disease).
The fact that half of the patients in this study presented with advanced oral cancer (stage IV) illustrates that prevention and early-detection strategies are urgently needed. The approaches might include the continuous education of health care professionals (i.e., the dissemination of the systematic examination of the oral cavity and emphasis on the importance of adequate reporting habits in patients’ charts) and information to general population (ie, spreading concepts like how to conduct an oral auto-examination, how tobacco smoking and alcohol drinking may be hazardous to the health, and the importance of seeing a health professional when a suspicious lesion appears in the mouth).