



Nonmyxomatous primary cardiac tumors are rare. Primary neurogenic tumors of the heart originating in the nerve sheath are extremely uncommon, and to date, 10 cases of neurilemomas, or schwannomas, have been reported.1–8
We report the case of a patient with a right atrial tumor who underwent a successful resection; histological examination revealed a benign primary schwannoma of the heart.
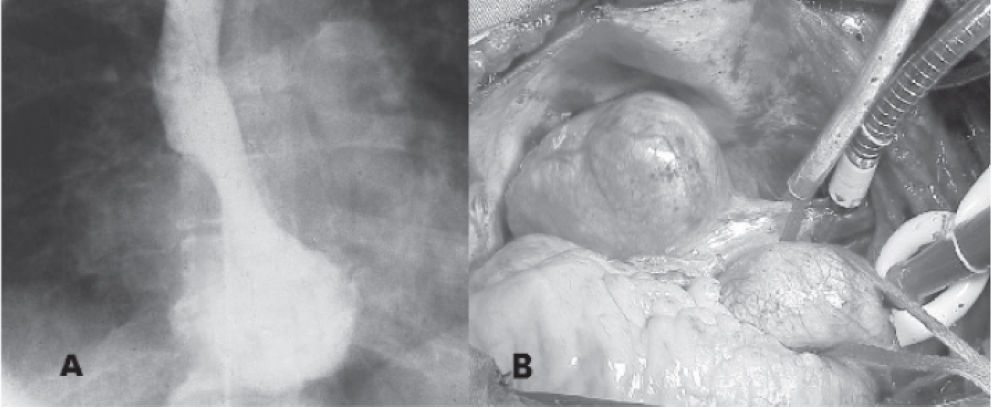
A 56-year-old asymptomatic woman had a spongy mass found in the bladder wall during cystoscopy. Resection was recommended and a preoperative chest roentgenogram showed an abnormal right cardiac silhouette. Computed tomography revealed a heterogeneous solid tumoral mass in the right atrium wall, with calcifications inside, leading to compression of the right atrium and superior vena cava. Angiogram and coronary arteriography were performed. No coronary lesions were found, and a mass was found in the right atrium wall projecting into the chamber (Fig. 1-A).

The patient underwent surgery with cardiopulmonary bypass, but without cardiac arrest; a venous cannula was placed in the superior vena cava. The mass was found in the right atrial wall close to the cavo-atrial junction and was completely removed. (Fig. 1-B) The right atrial wall was reconstructed with a bovine pericardial patch.
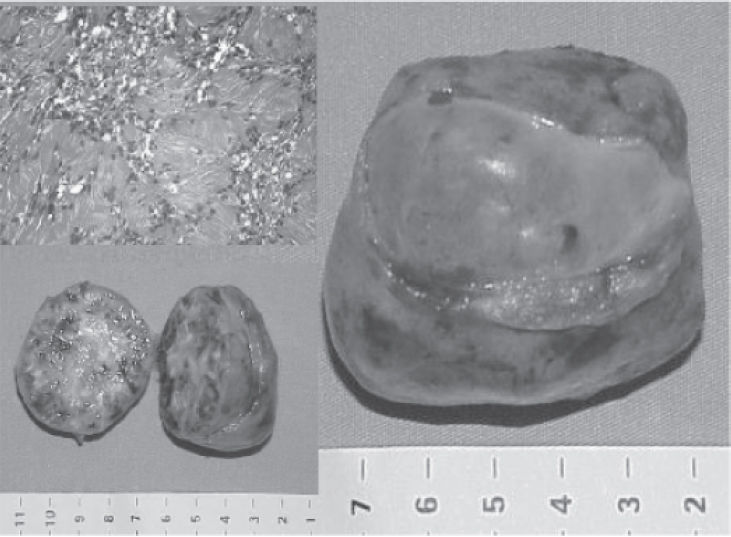
The mass consisted of an encapsulated ovoid tumor, measuring 6.0 x 4.8 cm and weighing 67 g, with brown and reddish heterogeneous tissue, with white and yellow strips on the cut section; it had a fibroelastic consistency and small calcified areas (Fig. 2). Microscopic sections revealed a mixed proliferation of Antoni type A tissue, with hypercellularity and palisading nuclei and fibers, and Antoni type B tissue with hypocellularity, forming the Verokay corpuscles. (Fig. 2) The diagnosis of benign schwannoma was established.
.")
The patient had pleural effusion and acute atrial fibrillation that were promptly and successfully treated in the early postoperative period. As she resumed sinusal rhythm, no anticoagulation therapy was applied. After discharge, she had an uneventful late outcome and remains asymptomatic 36 months after surgery; echocardiograms have shown no recurrence of the disease.
Primary cardiac tumors are rare, found in 0.0017% to 0.28% of autopsies, with 76% being benign, and of these, 40% being myxomas.1 Schwannomas (neurilemomas) are neurogenic neoplasms arising from a nerve sheath, which often involve cranial nerves, posterior spinal nerve roots, nerve of the extremities, the posterior mediastinum, and the vagus nerve.2
Neurogenic cardiac tumors are extremely rare, and they are almost always benign and primary, although they may sometimes present as malignant and metastatic tumors.3,4
When found as primary neoplasms, schwannomas frequently arise from the nervous system of the heart, which resides in the epicardial fat and contains both myelinated and unmyelinated axons, located primarily on the right side of heart, particularly in the right atrium and close to the cardiac plexus.5 This was the very same location found in this patient. However, schwannomas can be found in the left atrium near the pulmonary arteries or in the atrioventricular groove.6,7
The cardiovascular symptoms of these tumors are related to their location, causing extrinsic compression and pericardial effusion when located in the atrial wall or in the pericardial sac; or they may lead to valvar obstruction when they are inside the atrial chamber. Symptoms also depend on the size, the rate of growth, and how promptly they are detected and removed. The most common clinical findings are chest pain, dyspnea, orthopnea, distal edema, syncope, arrhythmias, and conductive disorders, and these symptoms are frequently associated to pericardial effusion1,5 and acute atrial fibrillation.6 Nevertheless, cardiac schwannomas can have a benign and asymptomatic presentation, such as in the patient reported here, as well as in other previously reported cases,8 where early identification and consequently smaller tumor size or location favored a lack of symptoms. Right ventricular outflow obstruction,5 thromboembolism, cardiac failure, and sudden death may also be late developments.6
Cardiac schwannomas can be revealed by echocardiography, but computed tomography and magnetic resonance imaging can better define the location, extent, and involvement of other structures, while coronary arteriography must be performed in patients at risk for coronary disease. Video thoracoscopy can be used safely for pericardial drainage and biopsy of intrapericardial masses.6
The macroscopic appearance of these tumors is as follows: an isolated ovoid encapsulated mass with a fibroelastic consistency, frequently involving the atrial wall, with a size that varies from 6 x 4 cm to 12 x 8 cm and weight ranging from 70 to 360 g. Microscopically, a schwannoma is identified by the presence of high and low cellularity areas, Antoni type A (with nuclear palisading and Verocay bodies), and Antoni type B tissues. The macroscopic and microscopic characteristics of this case are concordant with previous descriptions in the literature.
In the case reported here, the radical resection of the tumor also involved the right atrial wall, and reconstruction was accomplished with a bovine pericardial patch, though synthetic tissue and autologous pericardium have also been used to correct the defect.6 Involvement and reconstruction of the atrial wall and the sutures which were performed may have contributed to the acute atrial fibrillation that occurred in the early postoperative period, which was promptly treated; no anticoagulation therapy was required since she remained in sinusal rhythm.
Complete removal of the tumor must be effected as soon as diagnosis is established and metastatic disease ruled out, even in the absence of symptoms, to avoid future growth and its life-threatening complications such as compression, embolization, valve obstruction, and sudden death.2,6
Although some patients can be operated on without cardiopulmonary bypass; its use is usually mandatory, since it provides safe hemodynamic conditions and a clean operative field favoring a radical and free-margin resection. After surgical treatment and complete resection, the patients reported in the literature have experienced good outcomes and excellent prognoses, and no adjuvant therapy has been needed. Late control may be performed through echocardiograms, as we are doing in this case, with no recurrence being reported.
This report adds a new rare case of schwannoma of the heart to the small number of cases already published, and emphasizes the importance of early diagnosis and the excellent result of surgical treatment.