



The level of hemoglobin A1c (HbA1c), also known as glycated hemoglobin, determines how well a patient's blood glucose level has been controlled over the previous 8–12 weeks. HbA1c levels help patients and doctors understand whether a particular diabetes treatment is working and whether adjustments need to be made to the treatment. Because the HbA1c level is a marker of blood glucose for the previous 60–90 days, average blood glucose levels can be estimated using HbA1c levels. Our aim in the present study was to investigate the relationship between estimated average glucose levels, as calculated by HbA1c levels, and fasting plasma glucose levels.
METHODS:The fasting plasma glucose levels of 3891 diabetic patient samples (1497 male, 2394 female) were obtained from the laboratory information system at the Izmir Bozyaka Training and Research Hospital in Turkey. These samples were selected from patient samples that had hemoglobin levels between 12 and 16 g/dL. The estimated glucose levels were calculated using the following formula: 28.7 x HbA1c – 46.7. Glucose and HbA1c levels were determined using hexokinase and high performance liquid chromatography (HPLC) methods, respectively.
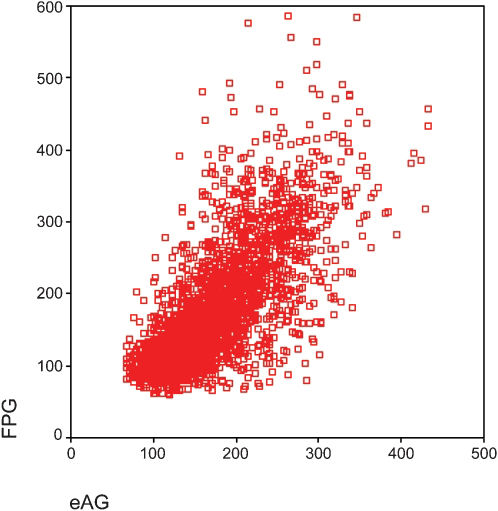
RESULTS:A strong positive correlation between fasting plasma glucose levels and estimated average blood glucose levels (r = 0.757, p<0.05) was observed. The difference was statistically significant.
CONCLUSION:Reporting the estimated average glucose level together with the HbA1c level is believed to assist patients and doctors determine the effectiveness of blood glucose control measures.
The management of diabetes mellitus requires an accurate evaluation of blood glucose control to assess the efficiency of a particular therapy. Whole blood hemoglobin A1c (HbA1c) measurements have been widely used in diabetes patients for more than 25 years to monitor long-term glycemic control.1,2 The measurement indicates a patient's average blood glucose level during the previous 60–90 days. It is recommended that diabetes patients have their HbA1c levels checked at least two times per year because quantitative and direct relationships have been identified between HbA1c concentration and the risk of diabetic microvascular complications.3 Therefore, clinicians use HbA1c test results to guide treatment decisions, and the test has become the cornerstone for assessing diabetes care.4
Various analytical methods based on different assay techniques, such as ion-exchange chromatography, affinity chromatography, immunoassays and electrophoresis, have been used to measure glycated hemoglobin levels.5 As a result, HbA1c results can vary considerably when measured by different laboratories or methods. Recently, the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) developed a new reference method that specifically measures the concentration of a single molecular species of glycated A1c.4 However, the new method results in values that are 1.5%–2.0% lower than current values, and the results are expressed in different units (millimoles per mole of unglycated hemoglobin), which may cause confusion for patients and health care providers.6
The relationship between the mean blood glucose level and the level of HbA1c has been investigated in different studies, and various equations have been obtained.2,7,8 Using Nathan's regression equation, which has been recommended by the American Diabetes Association (ADA), the estimated average glucose (eAG) level calculation and its relationship to the fasting plasma glucose (FPG) level were investigated in the present study.
MATERIALS AND METHODSThe fasting plasma glucose levels of 3891 diabetic patient samples (1497 male, 2394 female) were obtained from a laboratory information system at the Izmir Bozyaka Training and Research Hospital in Turkey. Blood samples were taken on the same day for the determination of both FPG and HbA1c. The study group was selected from patient samples that had hemoglobin levels between 12 and 16 g/dL because HbA1c results can be influenced by several factors, including anemia. In addition, samples from patients with hemoglobin abnormalities or uremia or who were pregnant were excluded. The estimated glucose levels (mg/dL) were calculated using the following formula: 28.7 x HbA1c – 46.7.6 According to the patients' levels of blood glucose control, we divided the samples into three groups: group A: FPG < 126 mg/dL; group B: FPG = 126–200 mg/dL; and group C: FPG > 200 mg/dL. Glucose levels were determined using the hexokinase method in an Olympus 2700 analyzer with commercially available Olympus kits (Olympus Optical Co. Ltd, Shizuoka-ken, Japan). HbA1c levels were determined using an HPLC method and an Agilent Technologies 1200 Series analyzer with commercially available kits (Chromsystems Instruments and Chemicals GmbH, München, Germany). Hemoglobin (Hb) levels were determined using a Beckman Coulter Gen S system (Beckman Coulter Inc., Fullerton, CA, USA).
All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS, version 11.0 for Windows, Chicago, IL, USA). Data were expressed as the means ± standart error of the mean (SEM). A p-value <0.05 was accepted as significant. The Kolmogorov-Smirnov test was performed to assess the normality of the variables. The Wilcoxon signed-rank test was used to compare the FPG and eAG levels, and the Mann-Whitney U test was used to compare the variables between males and females. The Spearman correlation coefficient (r) was used to test the relationship between the FPG and eAG levels.
RESULTSAccording to the Kolmogorov-Smirnov test, the distributions of age, HbA1c, FPG, eAG and Hb were abnormal (p<0.05). The study group consisted of 3891 individuals with a mean age of 56.5 ±0.2 (ranging from 18 to 92 years old) (Table&146;1). The mean FPG, eAG, HbA1c and Hb levels in the whole group presented in Table&146;1. A strong positive correlation was found between FPG and eAG levels (r = 0.757, p<0.05).
The levels of the glycemic parameters and the correlation coefficients for all groups (mean ±SEM).
| Entire group | Group A FPG: < 126 mg/dL | Group B FPG: 126–200 mg/dL | Group C FPG: > 200 mg/dL | |
|---|---|---|---|---|
| N | 3891 | 1736 | 1313 | 842 |
| Age (y) | 56.5 ±0.2 | 54.7 ±0.3 | 58.8 ±0.3 | 56.6 ±0.4 |
| FPG (mg/dL) | 159.4 ±0.9 | 103.2 ±0.3 | 155.3 ±0.6 | 281.7 ±2.3 |
| eAG (mg/dL) | 159.7 ±1.2 | 125.1 ±0.7 | 160.6 ±1.0 | 229.6 ±1.9 |
| Hb (g/dL) | 13.7 ±0.02 | 13.6 ±0.02 | 13.7 ±0.02 | 13.8 ±0.04 |
| HbA1c (%) | 7.2 ±0.03 | 6.0 ±0.02 | 7.2 ±0.04 | 9.6 ±0.07 |
| FPG vs. eAG | r = 0.757 | r = 0.300 | r = 0.443 | r = 0.450 |
Although the mean levels of FPG and eAG were close, according to the Wilcoxon signed-rank test, they were statistically significantly different (p<0.05).
The mean age and the HbA1c, FPG, eAG and Hb levels in groups A, B and C are shown in Table&146;1. The similarities in the average levels of FPG and eAG that were present for the group as a whole disappeared when the patient samples were separated into groups A, B and C. The correlation coefficients for these groups are presented in Table&146;1 (p<0.05). The eAG levels were higher in groups A and B than in group C compared to FPG levels.
The relationship between the levels of FPG and eAG was investigated for males and females using Spearman's correlation coefficients after verifying the normality of variables with the Kolmogorov-Smirnov test. The correlation coefficient was higher in women (r = 0.779) than in men (r = 0.723) (p<0.05). In addition, the mean levels of FPG, eAG, HbA1c and Hb were higher in males than in females (Table&146;2). A statistically significant difference was found for eAG, HbA1c and Hb levels between men and women (Table&146;2).
A comparison of the glycemic parameter levels in males and females (mean ±SEM).
| Male | Female | p-value | |
|---|---|---|---|
| n | 1497 | 2394 | |
| Age (y) | 56.4 ±0.3 | 56.5 ±0.3 | 0.711 |
| FPG (mg/dL) | 160.4 ±2.0 | 158.7 ±1.55 | 0.374 |
| eAG (mg/dL) | 162.8 ±1.5 | 157.6 ±1.1 | 0.001 |
| Hb (g/dL) | 14.2 ±0.03 | 13.3 ±0.02 | 0.001 |
| HbA1c (%) | 7.3 ±0.05 | 7.1 ±0.04 | 0.001 |
The HbA1c measurement is used to determine the average level of glycemic control over the previous 8–12 weeks; this measurement is accepted as a gold-standard measurement of chronic glycemia.4 Despite its wide international use, there is a substantial lack of standardization among HbA1c determination methods. The desire to standardize the HbA1c results obtained from different techniques led the IFCC to create a reference method, but this method created problems in reporting measurement results.7 One problem is the risk of decreasing a patient's glycemic control; when a patient's HbA1c measurement is lower than previous results, he or she might become confused and perhaps change diet, which could negatively impact his or her metabolic control.9 The other problem is the reporting of HbA1c levels in mmol HbA1c per mol total Hb, which could confuse patients. In addition, guidelines for diabetes have been based on standard levels that are derived from reports of the Diabetes Control and Complications Trial (DCCT) and the U.K. Prospective Diabetes Study (UKPDS). The equivalent of the current HbA1c targets of 6.5% and 7.5% are 48 milimoles per mole and 59 milimoles per mole in the new units. To resolve these problems, the ADA, the European Association for the Study of Diabetes (EASD) and the International Diabetes Federation (IDF) sponsored an international study to define a mathematical relationship between HbA1c and the eAG level.6 The following formula describes this relationship: 28.7 x HbA1c - 46.7 = eAG. This formula will assist health care providers and their patients in interpreting HbA1c values in units similar to those that the patients see regularly through self-monitoring.6
Using this formula, we calculated the eAG levels of our study group and investigated their relationship with the FPG levels. Surprisingly, the eAG levels were closely associated with the FPG levels when the measurements were taken the same day. There was not only a strong correlation between the eAG and FPG levels, but their mean levels were also very similar (159.7 mg/dL and 159.4 mg/dL, respectively). We at first thought that the eAG and FPG levels could be used interchangeably. It appeared that determining a patient's HbA1c level might be unnecessary if we could determine his or her FPG level because we could simply calculate it with the aforementioned formula. We decided to directly compare the eAG and FPG levels statistically. Although their mean levels seemed to be similar, they were actually significantly different (p = 0.001). Although we observed a significant difference between the average levels, this difference was not clinically meaningful. For 1567 samples, the eAG levels were lower than the FPG levels, whereas for 2324 samples, the eAG levels were higher than the FPG levels. These findings clearly demonstrate that the eAG and FPG values cannot be used interchangeably. We accepted the similar means of the eAG and FPG levels as a coincidence. This similarity in the FPG and eAG levels for the entire group disappeared when the subgroups were separated according to FPG level. In addition, the decrease in the significant strong correlation coefficient showed that the association depended on the patients' levels of glucose control. As glucose control worsened, the association became stronger.
On the other hand, most patients who come to the clinic for plasma glucose determination pay more attention to fasting and diet rules. The eAG levels in the study group were higher than the FPG levels not only because patients come to the lab in a fasting state but also because the eAG level is reflective of all plasma glucose levels over the previous three months, including the postprandial glucose levels. Sixty percent of patients had higher eAG levels than FPG levels. When we evaluated the eAG levels of patients in group C, we found that their eAG levels were lower than their FPG levels, in contrast with the findings for groups A and B (Table&146;1). We assumed that patients with higher FPG levels experienced stress before coming to the hospital to give blood or did not take their anti-diabetic drugs, since their FPG levels were higher than their average blood glucose levels.
We also wanted to understand the effect of gender on the eAG and FPG levels. Among age-matched samples, females had lower eAG and FPG levels than males (Table&146;2). The decreased levels of eAG and HbA1c in women were significantly different from those of males. In addition, there was a significant difference between the eAG and FPG levels in both men and women (p = 0.000). The eAG levels of females and males were higher than the FPG levels in most patients (58% and 62%, respectively), similar to the results found for the group as a whole (60%).
The IDF estimates that 285 million people worldwide have diabetes. This total number is expected to rise to 438 million within 20 years. Turkey, with approximately 70 million inhabitants, is a country where diabetes and impaired glucose tolerance are moderately common, but awareness of diabetes remains poor.10 It is thought that diabetic patients require better strategies to improve self-management.11 One of these strategies is the use of eAG levels together with HbA1c values. Although the clinical usefulness of eAG is not clear,12,13 we believe that every patient's eAG level should be calculated and reported along with his or her HbA1c level. This strategy will help patients better understand the importance of keeping their blood glucose levels within acceptable limits and maybe will rescue them from some invasive approaches for glucose homeostasis. 14
CONCLUSION
According to our data, patients with good to moderate blood glucose control are not entirely successful at managing their blood glucose, as reflected by their eAG levels, and the association between the FPG and eAG levels depends on the extent of blood glucose control.