





The number of mobile applications (apps) related to health is increasing, and diabetes mellitus (DM) is not an exception. The aim of this study was to assess the free mobile applications for the management of diabetes available, in Spanish, in the Spanish market.
MethodsGooglePlay (Android) and AppStore (iOS) were reviewed to identify free apps, in Spanish, aimed at people with diabetes. Their main functions and a series of quality and usability features were evaluated and scored. These scores were used to make a top list with the best apps.
ResultsOut of 794 registered apps, 42 were evaluated and included in the quality assessment, while 34 apps were included in the usability assessment. The main function of most of the apps was to act as a blood glucose diary (n: 30; 71.43%). As for privacy, most of the applications (33 apps; 78.6%) access device/personal data. Only a minority of apps [3 (7.1%)] reported being based on evidence, and only 3 apps (7.1%) had a quality label. The top scored apps were: OneTouch Reveal™, Social Diabetes™, mySugr: App Diario de diabetes™, Diabetes menú™, Tactio SALUD™ and Diabetes:M™.
ConclusionsThere are few free apps for diabetes management available in Spanish, most lack quality certification and very few provide scientific references about their content. Furthermore, most of the apps access personal/device data.
La cantidad de aplicaciones móviles (apps) relacionadas con la salud está aumentando, y la diabetes mellitus (DM) no es una excepción. El objetivo de este estudio es evaluar las apps móviles gratuitas disponibles en español para el manejo de la diabetes.
MétodosGoogle Play (Android) y App Store (iOS) fueron revisados para identificar apps gratuitas, en español, dirigidas a personas con diabetes. Sus principales funciones y una serie de características de calidad y usabilidad fueron evaluadas y calificadas. Estas puntuaciones se usaron para hacer una lista de las mejores apps.
ResultadosDe las 794 apps registradas, 42 fueron incluidas en la evaluación de calidad, mientras que 34 apps se incluyeron en la evaluación de usabilidad. La función principal de la mayoría de las apps era actuar como un diario de glucosa en sangre (n: 30; 71,43%). En cuanto a la privacidad, la mayoría de las apps (33 apps, 78,6%) acceden a datos del dispositivo/personales. Solo una minoría de apps (3 [7,1%]) informaron que se basaban en evidencia científica y solo 3 apps (7,1%) tenían un certificado de calidad. Las apps mejor puntuadas fueron: OneTouch Reveal®, SocialDiabetes, mySugr: app Diario de diabetes®, Diabetes menú®, Tactio SALUD® y Diabetes:M®.
ConclusionesHay pocas apps gratuitas disponibles en español para el manejo de la diabetes, la mayoría carecen de certificado de calidad, y muy pocas proporcionan referencias científicas sobre su contenido. Asimismo, la mayoría de las apps acceden a datos del dispositivo/personales.
The mobile technology used to improve health results, known as mHealth,1 is a practice in development.2 As a result, the number of mobile applications (apps) related to health is increasing: more than 100,000 health applications are available in the most used app stores,3 and their use in diabetes (DM) is no exception.4 Indeed, several systematic reviews and meta-analyses assess the effects of mobile applications on glycaemic control.5–11
Since these mobile apps can be used to make health-related decisions, their reliability is crucial. Thus, the working groups “Tecnologías aplicadas a la diabetes” and “Diabetes 2.0” from the “Spanish Diabetes Society” have developed recommendations on the use of Apps in DM, both for health professionals and for people with the disease.12 This guideline emphasizes aspects such as: the functionalities of the app, the identification of the people in charge of the app, clear identification of advertisements, the frequency in the update of the contents, the presence of reliable sources of information, the existence of clear terms and conditions of use, the consumption of device resources, adherence to data protection rules, the importance of checking with your doctor the use of the app and certification with a quality label.
Previous systematic reviews have been performed of DM apps available in English and German.13–14 Arnhold et al.13 considered the number of recently launched DM apps, their functions, target user groups, languages (English and German), price, user ratings, available interfaces and the association between price and user ratings. A similar study was carried out by Brzan et al.,14 who only included apps in English and did not evaluate the quality characteristics of the apps.
Therefore, the objective of this study was to evaluate mobile apps for the management of DM, in Spanish, available in the Spanish market and identify some that could be recommended to patients with the disease.
MethodsSearch methodA systematic review was made of mobile applications available in the main platforms on the Spanish market: GooglePlay (Android) and AppStore (iOS). Data collection was performed by one reviewer (AQR), with the support and supervision of a second reviewer (AMW) between 10/31/2017 and 03/03/2018, using the keyword “Diabetes”. Neither GooglePlay nor AppStore for iPad have a filter to select apps according to language, so apps with free access were downloaded and their language was checked.
Inclusion criteria were: free access, Spanish language and people with DM as intended users. Apps that did not work, premium, unavailable, fraudulent and plagiarized apps and those aimed at health professionals were excluded.
Apps or their functionalities were considered premium if they required a payment or a specific device (e.g. a certain glucometer) to be used and they were considered for professionals if it was specified in the description, if they were intended for hospital use or required advanced, specific knowledge.
Data collectionThe names and the version of all the apps that came up in the search results on each platform were collected in a spreadsheet. Subsequently, for those that met the inclusion criteria, the following, additional variables were collected: date of last update, description, store, operating system, developer, premium content, utilities and price, number of downloads (only available in GooglePlay), educational component, user rating, target audience (including type of diabetes), privacy (if the app accesses device data), scientific evidence, advertising, data importation from other devices (e.g. glucometers), hypoglycaemia indicator, ketone management, glycated haemoglobin (HbA1c) management, insulin dose calculation, contact with physician, generation of graphs, results registry, schedule notifications, lipid profile, other utilities, need for internet connection, memory consumed by app, account requirement and presence of a quality certification. For data collection, the information provided by the page of the app in the store was taken into account, as well as the information provided by the app itself. After collecting the data of the selected apps, quality and usability criteria were applied.
The data related to “privacy” were collected based on the permissions requested by the app and the privacy policies provided by the Store page or the app itself. Those apps whose privacy policies were not accessible, or which provided links that did not work, were considered as if they accessed private data. Time since last update of each app was broken up into five categories (on the 03rd March 2018): [0–3], (3–6], (6–9], (9–12], >12 months. Regarding users’ ratings, for apps with ratings from both stores, their mean was calculated; if the app was available in both Stores but only one had the rating available, the available rating was the only one that was taken into account. Those apps that have functionalities restricted by premium pass have been classified as if they did not have that function.
The apps were downloaded and tested on a Samsung Galaxy S6 SM-G920F 32GB mobile device (Android Version 7.0 – Kernel Version 3.10.61-10958180) and on an Apple iPad Air 2 – 64GB WiFi device (Model: MH182TY/A Version 11.2.6). Since the variable “operating system” has been qualified based on the result of the search for the keyword “diabetes”, there may be apps available in both stores, which were not registered. In addition, we evaluated the AppStore via an iPad. Thus, apps which are exclusive for iPhone devices could not be included in the evaluation. Additional devices were used and both stores re-checked, to assess selected apps at a later stage (see below), in June 2018.
Quality criteriaThe quality criteria were developed based on the recommendations of the Andalusian Health Service. This organization has developed a quality and safety strategy for mobile health apps and has created a certification, called “AppSaludable” [Healthy App].15 To obtain this certification, a series of 31 quality and safety recommendations are provided that an application should meet. Apps with this certification should allow citizens to use them reliably, minimizing risks. Most of the items were used to assess the quality of the apps, although some have been excluded, because they were assessed anyway, because they were aimed at app developers, or for pragmatic reasons, due to difficulties in their evaluation through the use of the app (see Appendix Table 1). Thus, a list of 24 recommendations remained (see Appendix) and an ad hoc score was developed for each item: 0: does not comply with the recommendation; 1: partially complies with the recommendation; 2: fully complies with the recommendation. Those apps that do not have advertising or do not access personal data have been rated with the highest score (2 points) in the respective items. Finally, the total score of each application has been calculated as the sum of the scores of each of the 24 recommendations (maximum score of 48 points).
Although we used the Andalusian AppSalud criteria for the quality assessment of the selected apps, three additional certification sources were explored: AppSalut, developed by the Catalonian Government,16 iSYScore, developed by the Spanish, non-profit organization Internet, Health and Society Foundation (Fundación Internet, Salud y Sociedad)17,18 and MyHealthApps, a UK-based, Patient View initiative.19
To certify an app, AppSalut assesses usability, technology, safety and contents.16 ISYScore includes popularity (user ratings, the use of two different platforms), reliability (validation by official body, authors and responsible entity identified, dedicated website, cites sources of scientific evidence, updated in the last year, funding information available) and utility (as a tool, as a learning means or as a social actor) in its rating, and the apps are assessed by a team of experts.17 MyHealthApps, on the other hand, represents the users’ perspective only, i.e. the patients and the carers who use health apps.19
Usability criteriaThe choice of “usability criteria” was based on the study by Arnhold et al.,13 which were rated by means of a 5-point Likert scale 1–5 or a dichotomous scale (0–1) (see Appendix Table 3). We added up these scores to obtain a total usability score for each app (maximum score: 47 points). The educational only apps, that did not allow any kind of interaction (e.g., enter values), were excluded from the usability criteria because there were difficulties assessing some of the variables.
It is worth noting that, for those applications available in both Android and iOS, the criteria of quality and usability have been applied to the Android version only.
Finally, a top list was developed with the applications that obtained the highest score in the quality and usability criteria. Two reviewers (AQR and AMW) reassessed these apps.
Statistical analysisThe SPSS™ (IBM SPSS Statistics 24.0.0) package for Windows (64 bits) was used. Normality distribution was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Correlations between quantitative variables were performed with Spearman's rank correlation coefficient. Comparisons between two groups were performed using the Mann–Whitney U test. A p value below 0.05 was considered significant.
ResultsIn total, 794 apps were registered: 215 exclusive for Android (27.1%), 554 exclusive for iOS (69.8%) and 25 available on both platforms (3.1%). Many (725) applications were excluded for different reasons (see flow-chart in Fig. 1). Thus, 42 apps were included in the Quality assessment and 34 apps were included in the Usability evaluation.
General aspects
The majority of the apps had been updated in the previous 3 months (n=18; 43.9%), whereas 4.9%, 17.1%, 4.9% and 29.3% had been updated in the (3–6], (6–9], (9–12] and >12 months period previous to the review. Among the 27 apps with a users’ rating, the mean score was 4.24 (SD: 0.43), out of a maximum of 5 points. Eighteen (42.9%) apps had premium content (1 of them, because it had the function to add values via one specific glucometer), with prices ranging between 0.50€ and 54.99€. The mean number of downloads (applicable to GooglePlay only), was 63,295 (SD: 103,614).
FeaturesThe main function of most of the apps was to act as a blood glucose diary (n: 30; 71.43%); while the remaining were educational only apps (n: 12; 28.57%). Almost one quarter of the apps (n: 9; 21.4%) allowed importation of blood glucose values. Furthermore, 5 apps had the function to indicate if the data entered was in the hypoglycaemia range. In addition, 5 apps (11.9%) had some form of ketone management function. Ten (23.8%) apps estimated HbA1c from glucose measurements, 3 (7.1%) allowed manual entry of the HbA1c value and 3 apps (7.1%) included both. In addition, 6 apps (14.3%) had the function to calculate pre-prandial insulin dose. Moreover, 3 apps (7.1%) allowed contact with their physician. Twenty apps (47.6%) had a function to export data and more than half of the apps (57.1%) generated graphs with the results. In addition, 28 apps (66.7%) provided a results history, 19 (45.2%) allowed to schedule notifications and 5 apps (11.9%) had a field to enter the lipid profile manually. Finally, 23 apps (54.8%) had some form of educational content.
Regarding the type of DM at which they were aimed, the majority of apps did not specify this (25 apps: 59.5%), 9 (21.4%) were oriented to DM1, DM2 and others, 6 to DM1 and DM2, 1 to DM1 only and 1 to DM2.
Quality featuresMost apps (33 apps; 78.6%) accessed device/personal data. There were 24 apps (57.1%) that did not require an account in order to be used, while 13 apps (31%) did and 5 apps (11.9%) had optional accounts to have access to certain functionalities. In contrast, very few apps [3 (7.1%)] refer to the scientific evidence used during their development and only 3 (7.1%) had some form of quality certification. In terms of advertising, 14 apps (33.3%) had some kind of ads.
In total, 42 apps were included in the quality score, whose mean was 28.2 (CI 95%: 25.3–31.0) (out of a maximum of 48 points). In agreement with the description above, the recommendations with highest mean scores were the recommendations “The health app adapts itself to its target audience” (mean: 2.00; SD: 0), “The health app neither presents any sort of known susceptibility nor any type of malicious code” (mean: 2.00; SD: 0) and “The health app follows the Principles of Universal Design, as well as reference accessibility standards” (mean: 1.95; SD: 0.216), while the lowest were “The health app offers concise information about the procedure used in order to select its content” (mean: 0.26; SD: 0.544), “The health app is based on one or more reliable information sources and takes into account the available scientific evidence” (mean: 0.31; SD: 0.643) and “The health app offers information about its funding sources, promotion and sponsorship, as well as about possible conflicts of interests” (mean: 0.48; SD: 0.804). For more details, see Supplementary file including the raw data.
UsabilityThe mean total usability score of the 34 apps assessed was 32.2 (SD: 1.0) (out of a maximum of 47) and the criterion mean score was 3.58 (SD 0.46) (maximum of 5 points). The criterion with the highest score was the “High fault tolerance/efficient fault management” (mean: 4.41; SD: 0.557). However, the “Simple, self-explanatory menu structures” was the variable with the lowest mean: 2.82 (SD: 1.218). Furthermore, only 2 apps (5.9%) had the ability to adapt the size of operating elements and displayed images; on the other hand, 16 apps (47.1%), had password-protected services. For more details, see Supplementary file including the raw data.
CorrelationsTotal quality score was correlated with total usability score (R=0.534, p<0.001), number of downloads (R=0.459, p<0.05) and time since the last update (R=−0.430, p<0.05), but not with users’ rating (R=0.208, p>0.05). There were no differences in the quality score in apps with and without premium content (z=−0.127, p=0.90), or with and without quality certification (z=−1.615, p=0.11). Regarding the usability score, it was not correlated with number of downloads (R=0.361, p>0.05), number of functions (R=−0.169, p>0.05) or users’ rating (R=−0.126, p>0.05).
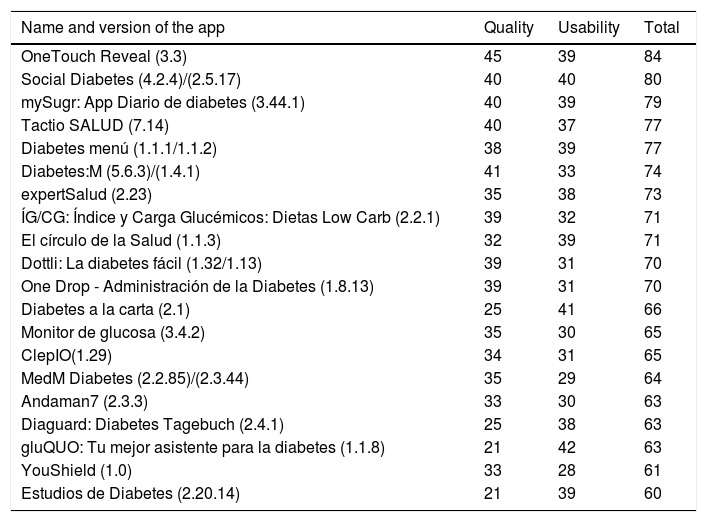
Top appsFinally, the apps with the best results in the total quality and usability score were: OneTouch Reveal™, Social Diabetes™, mySugr: App Diario de diabetes™, Diabetes menú™, Tactio SALUD and Diabetes:M™ (see key features in Fig. 2). Social Diabetes™ and mySugr: App Diario de diabetes™ are certified health products, whereas Tactio SALUD includes a list of references as supporting evidence. A list of the top 20 app, with their corresponding scores, is shown in Table 1.

Top 20 apps and their quality, usability and total scores.a
| Name and version of the app | Quality | Usability | Total |
|---|---|---|---|
| OneTouch Reveal (3.3) | 45 | 39 | 84 |
| Social Diabetes (4.2.4)/(2.5.17) | 40 | 40 | 80 |
| mySugr: App Diario de diabetes (3.44.1) | 40 | 39 | 79 |
| Tactio SALUD (7.14) | 40 | 37 | 77 |
| Diabetes menú (1.1.1/1.1.2) | 38 | 39 | 77 |
| Diabetes:M (5.6.3)/(1.4.1) | 41 | 33 | 74 |
| expertSalud (2.23) | 35 | 38 | 73 |
| ÍG/CG: Índice y Carga Glucémicos: Dietas Low Carb (2.2.1) | 39 | 32 | 71 |
| El círculo de la Salud (1.1.3) | 32 | 39 | 71 |
| Dottli: La diabetes fácil (1.32/1.13) | 39 | 31 | 70 |
| One Drop - Administración de la Diabetes (1.8.13) | 39 | 31 | 70 |
| Diabetes a la carta (2.1) | 25 | 41 | 66 |
| Monitor de glucosa (3.4.2) | 35 | 30 | 65 |
| ClepIO(1.29) | 34 | 31 | 65 |
| MedM Diabetes (2.2.85)/(2.3.44) | 35 | 29 | 64 |
| Andaman7 (2.3.3) | 33 | 30 | 63 |
| Diaguard: Diabetes Tagebuch (2.4.1) | 25 | 38 | 63 |
| gluQUO: Tu mejor asistente para la diabetes (1.1.8) | 21 | 42 | 63 |
| YouShield (1.0) | 33 | 28 | 61 |
| Estudios de Diabetes (2.20.14) | 21 | 39 | 60 |
No diabetes apps are available yet in AppSalut.16 In the iSYScore, 5 diabetes apps were included in the top 20 health apps for patients in 2017: Social diabetes (37 out of a maximum of 47 points), OneDrop (36 points), mySugr:App Diario de diabetes (31 points), Contour Diabetes (27 points) and Diabetes a la carta (24 points).18 All of them were included in our top 20 list, too, except for Contour Diabetes, which was not assessed, given the fact that it was linked to a specific device. In MyHealthApps, mySugr is included, with a comment by Diabetes Voice 2013 (IDF), but the link provided is not active. None of the other apps in our top 20 list is present in this platform.19
DiscussionIn view of these results, there are few apps available in Spanish in comparison with other languages like English. Furthermore, very few apps had scientific evidence and a quality certification, which is worrisome, considering that they are used by patients, who could follow the advice provided. Other problems are the privacy elements and the use of data that apps can access when they are installed, since most of the apps reviewed were able to access device and personal data; some may even share personal information with third parties. In addition, more than half of the applications did not specify what type of DM they were targeting, which can be a problem for patients when using the apps, since the different types of DM have specific needs. In favour of the apps, most had been updated in a period of 3 months, which reflects the attention of the developers to keep them free from errors and with updated content.
In terms of functionalities, the insulin dose function deserves to be mentioned. As Hirsch et al. stated, the safety and clinical efficacy of these smartphone-based bolus calculators are not known.20 Therefore, it should be checked if the applications provide some type of scientific reference and/or the procedures carried out to develop the insulin dose calculators. With regard to quality criteria, the mean total score was just above half of the maximum score. Thus, it is reasonable to say that the contents provided by most of the applications should be taken with caution.
As far as the usability criteria are concerned, the average total score was also half-way to the maximum score. The variable with the best result was High fault tolerance/efficient fault management, which shows the care that the developers of the applications have in the possibility of modifying the results, while the variable with the worst average (simple, self-explanatory and menu structures) reflects that more effort should be put not only to improve the contents of the applications but also the presentation and the ability to adapt to the user, since only 2 apps had the ability to adapt the size of operating elements and displayed images.
There were no apps for diabetes with a quality certification from the Andalusian Health Service,15 although there are several in the application process. It is worth noting that this quality certification and the Decalogue from the Spanish Diabetes Society are relatively recent, so it is expected that more apps will be included in the near future. Indeed, some of the apps do have the EC “health product” certification. Regarding other quality criteria, the Spanish iSYScore included 5 diabetes apps among their the top 20 health apps, 4 of them among our top 20 apps, too (see Table 1).18
Regarding the top app list, OneTouch Reveal™, Social Diabetes™ and mySugr™ were those with the highest scores. This means that they fulfil the prespecified criteria more than other apps, although patients might choose one or the other depending on their preferences regarding available functionalities, usability and privacy issues (see Fig. 2). For example, OneTouch Reveal™ had the highest quality and total scores, but does not include an insulin dose calculator, a feature that is highly valued by patients with type 1 diabetes, proficient in carbohydrate counting. Both mySugr™ and Social Diabetes™ include an insulin dose calculator and have a health product certification. Diabetes:M™, on the other hand, includes an insulin dose calculator and allows to count carbohydrates based on a food database, but does not have a health product certification or provides scientific references about its contents. Regarding people with type 2 diabetes, both OneTouch Reveal™ and Tactio Salud™ may be interesting apps. Indeed, the latter allows to monitor, not only blood sugar, but associated cardiovascular risk factors, too.
The main strength of this study is that, to our knowledge, it is the first systematic review about apps available in Spanish, and could be helpful for patients in Spanish-speaking countries. Furthermore, we have extensively assessed the quality properties of the apps and ranked the top 20. We believe that we provide valuable information to health care professionals who might want to recommend an app to their patients. Finally, we used adapted, PRISMA-based methods, a recognized reference in the performance of systematic reviews.21
If we stop to appreciate the differences with the rest of studies, we should compare this study with those performed by Arnhold et al.13 and Brzan et al.14 Regarding Arnhold's study, the main similarities are that we both included apps only available in Android and iOS and evaluated the usability of the apps. On the other hand, we have some differences with that study: they included premium apps, whereas we included only free apps. In addition, their search method included, not only diabetes, but also other keywords such as “Blood Sugar/Blutzucker, Glucose/Glukose” and chose the subcategories “Health and Fitness” and “Medicine” on AppStore, so they may have included a wider variety of apps. In addition, the usability criteria were assessed by three evaluators, whereas, in this study, we only had one evaluator, so the results may be more subjective than the results from the cited study. They also examined if the available applications served the special needs of DM patients aged 50 or more. However, they only focused on usability, and did not include quality criteria, as we did.13
With respect to Brzan's study, the main similarities are that they only included free apps and used the keyword “diabetes” in their search. However, they also included apps for windows phone, which may be of interest to patients that have devices with that operating system. Like Arnhold et al. three independent experts were included in the assessment for eligibility and in the testing phase. Again, they did not evaluate the quality characteristics of the apps. It should be noted that they used demanding inclusion criteria, which resulted in only 9 apps being analyzed.14
We also acknowledge that this study has some limitations. The exclusion of the paid apps (and exclusive access apps) may have left out relevant, even high-quality, apps, and we are also aware of the fact that including an additional reviewer throughout the whole process would have made the results more robust. Furthermore, apps are in constant development and what is true today might not be accurate in a few months’ time. We encourage users and prescribers to be updated on the conditions of use and the certification status of the most popular apps.
To summarize, there are few free apps available for diabetes management, in Spanish, in comparison with other languages and most of them act as a blood glucose diary. In addition, most of the available apps lack any kind of quality certification and very few provide scientific references about their content. Therefore, we recommend developers to focus on improving the quality of their applications. In addition, most of the apps accessed personal/device data, which should alert app users to read the terms and conditions thoroughly. In the future, quality elements should be considered when evaluating an app. Indeed, clear-cut recommendations are available for this purpose in Spain.
Conflict of interestsThe authors declare that there is no conflict of interests.
The present research has not received any specific grant from agencies of the public, commercial, or non-profit sectors. AMW was supported by a grant from the Spanish Research Board (PI16/00587), the European Horizon 2020 Programme (IC-HEALTH: SC1-HCO-12-2016, Proposal 727474) and European Union Regional Development Funds (MACBIOBLUE), during the performance of the study. This study was carried out as a final degree project (AQR, Universidad de Las Palmas de Gran Canaria, year 2017–2018).
The following are the supplementary data to this article:
