




In neonatal units, Salmonella infections have been attributed to food-borne sources and person to person transmission.
MethodsThe outbreak described is the first reported by Salmonella enterica serotype Newport in a neonatal facility in Spain.
ResultsThe index case was an 8-day premature newborn that developed clinical sepsis with positive blood cultures. The outbreak source was the mother of the index case.
ConclusionsIt is essential to improve infection control measures taking into account the parents, as they can be an important source of infection.
En unidades de neonatología, las infecciones por Salmonella han sido atribuidas a fuentes alimentarias y a transmisión de persona a persona.
MétodosEl brote descrito es el primero ocasionado por Salmonella enterica serotipo Newport en una unidad neonatal en España.
ResultadosEl caso índice era un recién nacido prematuro que desarrolló sepsis clínica con hemocultivos positivos. La fuente del brote fue la madre del caso índice.
ConclusionesAl implementar medidas de control de la infección nosocomial se debe tener en cuenta a los padres ya que pueden constituir una fuente importante de infección.
Nontyphoidal Salmonellae are important causes of reportable foodborne infection. These bacteria are especially problematic in a wide variety of individuals especially infants, elderly and immunocompromised hosts and can lead to serious conditions such as gastroenteritis, bacteraemia, septic arthritis, meningitis and pneumonia.1Salmonella as an etiologic cause of nosocomial infections is considered an infrequent agent. Health care-associated Salmonella outbreaks in neonatal units are rarely described but could be control challenging because of its persistence in the environment, the high prevalence of asymptomatic forms and prolonged carriage in infants.2 In neonatal units, Salmonella infections have been attributed to food-borne sources, including contaminated infant formula and breast milk3,4 and person to person transmission by means of infected health care workers (HCWs) and fomites.5,6 In Europe, during 2008, Salmonella enterica serotype Newport only accounted for 0.7% of all salmonellosis reported cases according to the European Surveillance System (TESSy), with the fifth place among the other serotypes.7 We described an outbreak of S. enterica serotype Newport gastroenteritis in a neonatal unit in Spain.
MethodsDescription of the outbreakThe outbreak occurred in the neonatal ward of the Hospital Universitari Vall d’Hebron (Barcelona, Spain). This is a 75-bed unit divided into 3 subunits: low-risk care (30 beds), intermediate care (20 beds) and intensive care unit (25 beds). The outbreak occurred in the low-risk care unit; this unit has 3 rooms communicated between them (room 4, 5 and 6). The outbreak period was defined from January 28th to February 15th, 2008. The index case was an 8-day premature newborn (34 weeks gestational-age) hospitalized since birth in room 4. On January 30th he developed gastroenteritis with dehydration and clinical sepsis, the blood and stool cultures were positive for S. newport. Empiric antibiotic treatment was initiated with ampicilin and gentamicin, and then changed to cefotaxime according to results of antimicrobial susceptibility. Contact isolation precautions were initiated and the epidemiological investigation was undertaken by the infection control team to trace the source of infection.
Epidemiological and microbiological investigationA case of nosocomial Salmonellosis was defined as either the isolation of S. newport from blood or stool specimen or more than 1 episode of diarrhea and/or vomiting in an infant who was hospitalized in the neonatal unit during the outbreak period. The following variables were collected for each case: age, sex, gestational age, birth weight, date of birth, date of admission, hospitalization room, instrumentations, oral medications, type of milk or powdered formula, symptoms and date of onset, gastrointestinal symptoms in family members, results of cultures and outcomes.
Hospital staff members who worked in low-risk care unit during the outbreak period and parents of infant cases were interviewed to assess the presence of gastrointestinal symptoms and were requested to submit stool samples for Salmonella culture. Also, microbiological investigation was conducted in all family members of the index case. Active surveillance for salmonellosis among current hospitalized patients was initiated and stool specimens were collected from all symptomatic and asymptomatic newborns who shared the same rooms with the cases.
Microbiological study and antimicrobial susceptibilityStool samples were plated on selective and differential media to study Salmonella (selenite enrichment broth, MacConkey agar, Salmonella-Shigella agar and xylose-lysine-desoxycholate agar). Cultures media were incubated at 37°C in aerobic atmosphere. To bacterial identification we used the identification card and software AMS-GNI (Vitek. BioMerieux, Francia). Salmonella isolates were serotyped, based on the antigenic properties of their O (somatic), H (flagellar) and Vi (capsular) antigens, using agglutination test with specific antiserum in accordance with the existing Kauffmann-White serotyping scheme (WHO Collaborating Centre for Reference and Research on Salmonella, which is located at the Pasteur Institute in Paris, France).8
Antibiotic susceptibility tests were performed by disk diffusion method on Mueller-Hinton agar and Rosco disks (Neo-Sensitabs. Rosco Diagnostica Taastrup. Denmark) following the interpretation of results by Clinical and Laboratory Standards Institute (CLSI) recommendations for Enterobacteriaceae. The antibiotics tested for the susceptibility study were: ampicillin, cefalotin, cefuroxime sodium, cefotaxime, ceftazidime, cefepime, cefoxitin, amoxicillin/clavulanate, piperacillin/tazobactam, aztreonam, gentamicin, tobramycin, amikacin, imipenem, nalidixic acid, ciprofloxacin, nitrofurantoin, fosfomycin and trimethoprim/sulfamethoxazole.
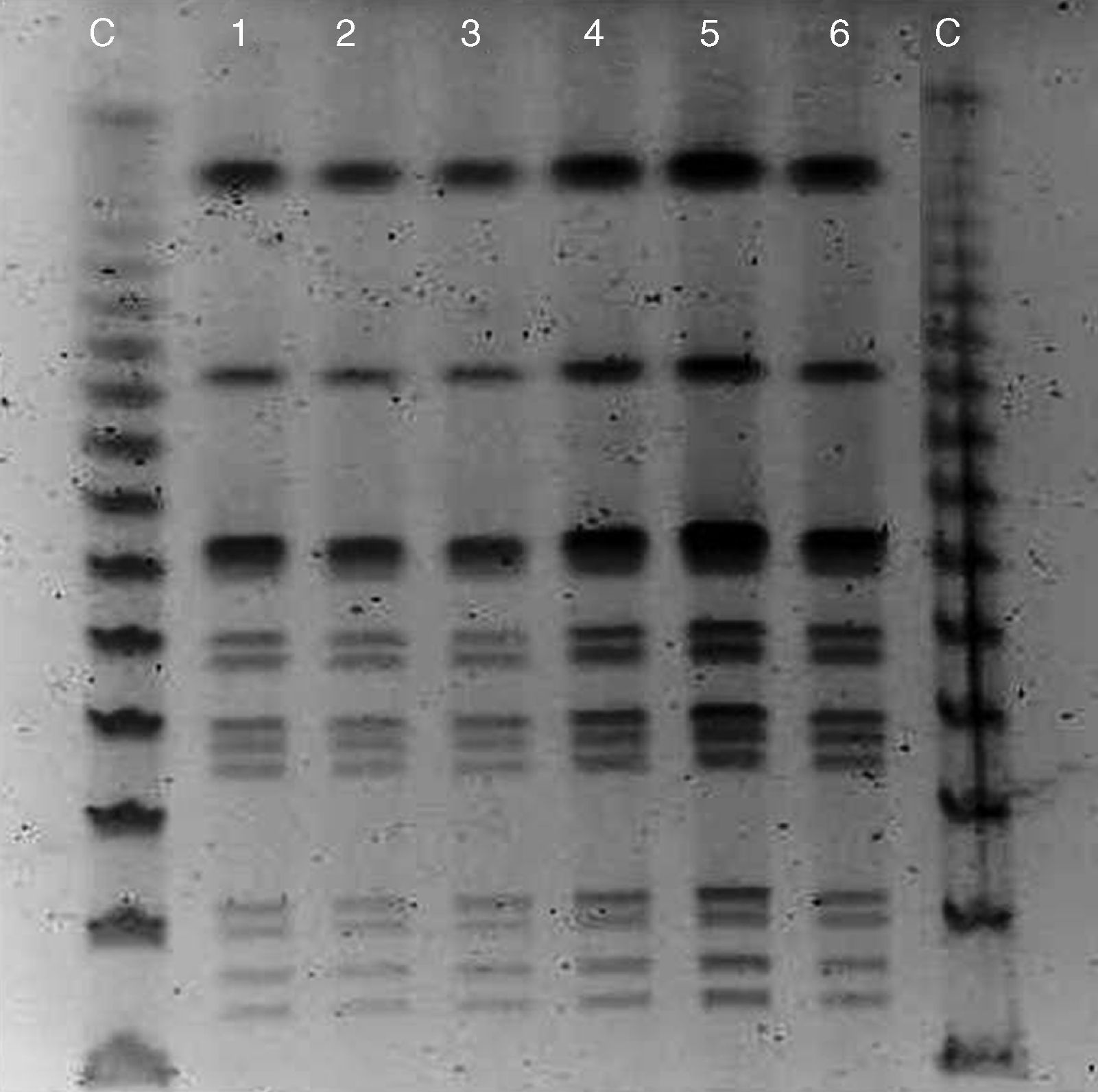
In order to establish the clonal relationships of the identified isolates of Salmonella the pulsed-field gel electrophoresis of restriction fragments (restriction enzyme: Xba1) of the chromosomal DNA were determined. Band patterns were visually interpreted following the criteria of Tenover et al.9
Infection control measuresAll of the cases were under contact precautions and housed in nursing cohorts until discharge or until a negative stool sample was obtained. Hand hygiene was reinforced and more alcohol-base hand sanitizers were conveniently placed on all inpatient rooms. Health-care workers (HCWs) with positive culture were placed on sick leave until they had a negative stool sample.
ResultsWhen the index case was reported, there were 20 newborns hospitalized in the low-risk care unit. Besides the index case, 40 people underwent microbiological testing: 11 neonates (2 symptomatic and 9 asymptomatic newborns hospitalized in rooms 4, 5 and 6), 27 HCWs and 2 parents. In total, six more cases were positive to S. enterica serotype Newport: 4 newborns (2 symptomatic and 2 asymptomatic cases), 1 parent and 1 nurse, the demographic and clinical characteristics of the cases are described in Table 1. The first secondary case was a premature 3-month infant with onset of gastroenteritis on January 31st (the day after the index case) and who had been hospitalized in room 5. She was discharged the 28th but remained under home visits by an ambulatory care nurse, who collected the stool sample that tested positive for S. newport. The next case was a 7-day full term newborn inpatient who was hospitalized also in room 5. The next two cases were asymptomatic infants who shared the same hospitalization rooms with the index case (room 4) or with the first secondary case (room 5). Only one case was detected among HCWs studied; it was an asymptomatic nurse who had attended three of the infant cases. All the infected newborns shared in some point of the outbreak period the rooms 4 or 5, they had common HCWs attending them but no medical or dietary risk factors were identified. The outbreak source was the index case's mother, a 30 year-old woman with Crohn's disease, without gastrointestinal symptoms at that moment but with a stool culture positive for S. newport. The seven isolated strains had the same antibiotic profile of resistance. All strains tested were sensitive to nalidixic acid, amoxicillin/clavulanate, ampicillin, aztreonam, cefepime, cefotaxime, cefoxitin, ceftazidime, cefuroxime sodium, ciprofloxacin, trimethoprim/sulfamethoxazole, fosfomycin, imipenem, nitrofurantoin, piperacillin/tazobactam, and showed intermediate susceptibility to amikacin, cefalotin and gentamicin. These results and also PFGE showed it was the same strain (Fig. 1). All infected patients recovered completely without complications.
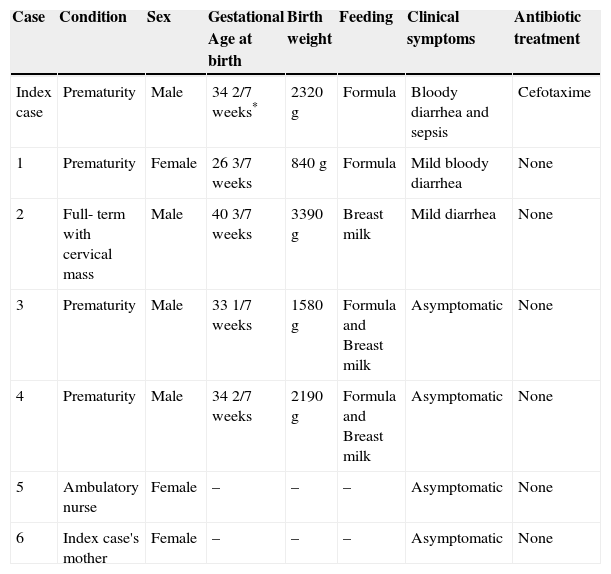
Demographic and clinical characteristics of Salmonella newport cases.
| Case | Condition | Sex | Gestational Age at birth | Birth weight | Feeding | Clinical symptoms | Antibiotic treatment |
|---|---|---|---|---|---|---|---|
| Index case | Prematurity | Male | 34 2/7 weeks* | 2320g | Formula | Bloody diarrhea and sepsis | Cefotaxime |
| 1 | Prematurity | Female | 26 3/7 weeks | 840g | Formula | Mild bloody diarrhea | None |
| 2 | Full- term with cervical mass | Male | 40 3/7 weeks | 3390g | Breast milk | Mild diarrhea | None |
| 3 | Prematurity | Male | 33 1/7 weeks | 1580g | Formula and Breast milk | Asymptomatic | None |
| 4 | Prematurity | Male | 34 2/7 weeks | 2190g | Formula and Breast milk | Asymptomatic | None |
| 5 | Ambulatory nurse | Female | – | – | – | Asymptomatic | None |
| 6 | Index case's mother | Female | – | – | – | Asymptomatic | None |
 of restriction fragments from 6 cases of the outbreak (except the nurse). The pulsotype profiles are almost identical and they can be attributed to the same strain of Salmonella enterica serotype Newport.")
This outbreak is the first reported in a neonatal facility by this serotype of Salmonella in Spain. The epidemiological investigation suggests as the origin of this outbreak, the index case's mother. She was an asymptomatic carrier of S. newport and the bacteria was spread from person to person in the low-risk care unit. At the time of the index case detection, the occupancy in this unit was 87%, probably contributing to a disruption in hand hygiene compliance by HCWs. In France, Cartolano et al.10 have reported one case of Salmonella branderburg from a premature newborn in a neonatal intensive care unit. This patient developed a septic shock syndrome on the 12th day of life and S. branderburg was isolated in his gastric aspirate and a stool sample; according to the outbreak investigation the pathogen was almost certainly transmitted by contaminated hands because the mother had a positive stool specimen but her milk was free of Salmonella. In our outbreak, the route of transmission was probably the same, as the newborn was fed with artificial formula. Besides the four secondary cases occurred by horizontal transmission among the unit, the affected nurse probably was infected during domiciliary care of one of the infected newborns. As far as the clinical course is concerned, it was noticed that the newborns being breastfed (mixed or exclusive) were asymptomatic in two cases or had mild diarrhea in one case. In contrast, the index case and one secondary case that had bloody diarrhea were exclusively fed with formula. These incidental findings could suggest a possible protective role of breastfeeding for severity of Salmonella infection already mentioned in other studies.11 The rapidity of the diagnosis, the prompt application of control measures and reinforcement of hand hygiene helped to avoid transmission to more children and HCWs within our neonatal unit. Thus, it is mandatory to improve infection control measures with HCWs but also with the parents of hospitalized infants, specially reinforcing hand-washing, as they can be an important source of infection in this setting.
Conflict of interest statementThe authors declare that they have no conflicts of interest.

