




























Since the economic crisis of 2008 were growth in health spending has reached unsustainable levels many countries have reduced public spending on health but it is now rising again in Italy (OECD, 2017). This study proposes a new way to use the official indicators for healthcare monitoring in order to assesses the impact by the reform of the Italian National Health Service on the equity access to health care service. A preliminary analysis was performed in order to evaluate geographical hospital resource allocation taking into account both the amount of resources and the intensity of care needed. A second analysis, performed using a two-stage least squares (2SLS) regression model, was addressed to explain geographic lifespan differences between Italian regions. In conclusion, this study attempts to provide an alternative reading to “sector studies”, to highlight more clearly the extent of the “healthcare mobility” phenomenon and the role of the supply structure as a driver of this phenomenon.
Since the economic crisis of 2008 were growth in health spending has reached unsustainable levels many countries have reduced public spending on health but it is now rising again in Italy (OECD, 2017).
National recommendations cannot take into account local factors such as population needs, organisational priorities, budgets, capacity or capability; hence many crucial decisions have to be made at regional and institutional levels.
As stated by Lipsey and Lancaster (1956): “It follows, therefore, that in a situation in which there exist many constraints which prevent the fulfilment of the Paretian optimum conditions, the removal of any one constraint may affect welfare or efficiency either by raising it, by lowering it, or by leaving it unchanged.”
This study proposes a new way to use the official indicators for healthcare monitoring in order to assesses the impact by the reform of the Italian National Health Service on the equity access to health care service. It addresses the planning issues of hospital resource allocation and examining the involving services distribution between 2007 and 2013 as a consequence of the Italian health service reform.
Several strategies may be adopted in order to rationalise resources allocated and reduce relative cost, such as downsize number of beds, improve timely access to treatment, decrease hospital average of stay, but unfortunately many of these interventions do not provide these benefits and the outcomes are not easily measurable. (Harris, Green, Ramsey, Allen, & King, 2017; Klein, 2010; Polistena et al., 2013).
Moreover, health authorities, hospitals and other health care facilities have always moved resources from one area to another in order to rationalise scarce resources but decisions to restrict or reallocate resources are generally reactive, undertaken in response to established or emerging problems (Barilan, 2013; Pearson & Littlejohns, 2007).
The international scientific literature studies health care systems through a series of indicators in order to evaluate the efficiency of health care supply (such as beds, healthcare staff, technological equipment, etc.) taking into account the demand of services (inpatient admissions, outpatient services, emergency procedures). To this end, in Italy, the Decree of the Ministry of Health of 12 December 2001 established the official indicators for healthcare monitoring, defining them as “information selected to obtain knowledge about relevant phenomena, measuring their changes and hence helping to steer decision-making at the various policy levels”.
This paper focuses on the number of acute hospital beds available in Italian public hospitals. The analysis does not include the production factor relating to staff and technologies, which will be examined separately.
Moreover, according to the scientific literature, this study considers beds as a proxy of total amount of resources needed to supply health care and the other costs of hospitalisation directly proportional to the number of bad used.
2Preliminary analysis of Italian health service supplyA preliminary analysis was conducted in order highlight any differences in the use of health resources by considering the three macro-areas of the country: North, central and south of Italy.
The main indexes taking into account for the preliminary analysis are:
- •
Number of beds
- •
Hospital discharge rate
- •
Occupancy rate
- •
Number of days in hospital
- •
Average length of stay
- •
Case-Mix index
Following the reform of the Italian National Health Service, the number of public hospital beds for acute patients per 1000 inhabitants has fallen steadily, declining by almost 10% over a period of 6 years (Table 1).
Breakdown of this figure by macro-areas of the country shows that while this decline is common to all areas, it is sharper and deeper moving from the north to the south of the country. Overall, the number of available beds remains higher in the Regions of Northern Italy. This is likely to reflect their greater financial capacity and a healthcare structure, characterised by medium-large hospitals.
2.2Hospital discharge rateAs a consequence of rationalisation of the system, the reduction in the number of beds available seems to have impacted the population's behaviour in recourse to hospital care. This phenomenon, measured through the Hospital Discharge Rate, if calculated in its most elementary form, shows marked geographical differences. The index thus calculated (Table 2) shows an overall reduction in recourse to hospital care of almost 15% across the national territory.
Looking at in-country differences, while in 2007 the value of this indicator in Southern Italy was close to the national average, in 2013 it was markedly lower, with a drop of almost 22%.
2.3Occupancy rateWhile the drop in in-patient beds has discouraged recourse to hospital care, on the other hand it has pushed occupancy rates up; however, it has also created a difficult-to-handle problem, namely the degree of saturation of production capacity.
In general, the rise in the use of beds, as measured by the Occupancy Rate, exceeded already in 2007 the target rates (70–75%) laid down in the Ministry of Health's Decree of 12 December 2001. However, breakdown of this indicator in the period in question by geographical macro-area (Table 3), shows that occupancy rates only increased in Southern Italy, from 75.6% in 2007 to 78.5%, coming into line with the national average.
2.4Number of days in hospital and average length of stayThe increase in productivity described above is partly due to a decrease in potential per-capita days in hospital, which dropped from 0.87 to 0.76 (Table 4) and partly to an increase in the average length of stay, which rose from 7.6 to 7.8 (Table 5). However, this change seems to have been driven solely by the Regions of Southern Italy.
The Case-Mix index (Table 6) used to measure the complexity of the cases handled, is given by the ratio of the average weight by medical discipline calculated in the facility to the standard Italian average weight. It provides useful information on the productivity of a hospital/department and its level of specialisation compared to the benchmark value. Values of ICM>1 indicate that the cases treated are more complex than the standard, while values below 1 indicate less complex cases.
On the basis of this preliminary classification, calculating the ratio of the number of departments treating complex cases (ICM>1) to the total number of departments for each of Italy's geographical macro-areas, a clear disproportion emerges between the facilities of Northern Italy (48.9% in 2013) and Central Italy (45.3%) compared with those of Southern Italy (29.7%), even though the latter grew by 2.3 percentage points in the period in question.
However, the above geographical differences are only partly attributable to the individual Regions’ programming capacity. Indeed, the amount of resources allocated is strongly influenced not only by the size of the hospitals, but also by the Regions’ funding capacity, and by the long-term sustainability of funding.
In this respect, the devolution of powers does not seem to have eliminated recourse to deficits by the Regions to finance their excess expenditure. While the strengthening of local autonomy has produced benefits in terms of greater management responsibility, it is still affected by the different revenue-raising capacity of the various Regions (Carroppo & Turati, 2007). Consequently, the share of healthcare spending covered by regional funds has different features and strategies in the different areas of the country.
3The deficit repayment plansDespite the structural initiatives described above, the persisting deficits led the national authorities to intervene on spending levels with Budget Law 2005 (Article 1(180) of Law 311/04) which required Regional governments with an economic-financial imbalance to conclude an agreement with the Ministry of Health and the Ministry of the Economy and Finance. The agreement would set out the actions necessary to rebalance the Regions’ budgets while ensuring the delivery of minimum standards of healthcare. This agreement led to a plan for the reorganisation, upgrading and strengthening of the Regional health service, which is called “Deficit repayment plan” (Piano di Rientro). Under the agreement, an initial phase focused on identifying the general and specific objectives for achieving the expected result. This was followed by actions and implementing decisions to launch the system reorganisation process and by subsequent monitoring based on a set of healthcare and economic-financial indicators.
This measure, with a roadmap and intermediate milestones established for each Region, translates operationally into streamlining of the service, which often involves further cuts to the number of beds, the closure of hospital departments with a small number of admissions, and the conversion or closure of hospitals considered not to be cost-effective.
Currently, the Regions with a Deficit Repayment Plan are mostly located in Southern Italy, plus Lazio and Piedmont. The Region of Liguria and Sardinia have successfully passed the audit and have been granted the resources conditional on fulfilment of the conditions established in the Deficit Repayment Plan.
The strong deficits of most Southern Italian Regions clearly led the national Government to use invasive yet necessary instruments such as the above-mentioned agreements. However, it should be noted that the geographical areas subject to intervention on average seem to have low capacity to self-finance their healthcare expenditure compared with the other Regions of Central and Northern Italy. Therefore, any action to streamline their service will necessarily require significant cuts to the resources available. This notwithstanding, a purely economic-financial assessment would shift attention away from the main focus which should always be to plan the health service around the needs of citizens. These needs must be met at the appropriate standards as established by law, and ensuring adequate access to the service.
4Material and methodPrecise assessment of the size of the Italian National Health Service requires the measuring of hospital services by reference to the degree of urgency of each type of service and the number of resources dedicated to them. Accordingly, this section provides a reclassification of inpatient medical disciplines followed by detailed analysis of the hospital resources used by the country's individual macro-areas.
Based on the results obtained, proposals will be made for adapting service design in light of access to the service and the availability of resources.
To highlight the imbalances between the country's geographical macro-areas that can be reduced, several indicators have been used, only some of which are the standard indicators normally used to perform an economic analysis of health services. For this reason, starting from the data on clinical specialties and medical disciplines codified by the Ministry of Health (Statistical Yearbook of the Ministry of Health, 2013), the specialties have been grouped into four main classes distinguished by different levels of treatment effort within healthcare facilities. The outputs of this procedure are shown in Table 7. The last available data on resources utilisation released by the Ministry of Health.
The decision to analyse the supply of health services using this classification is due to the different intensity of use of funds by the four groups of medical specialties, regardless of the technical–professional level and the degree of specialisation of procedures. It is known in healthcare economics (Levaggi & Capri, 2008) that, for instance, an ICU requires a higher amount of financial, human and technological resources compared to other departments having the same level of specialisation.
This classification, which can be improved further, has already shown different degrees of propensity by individual hospitals to deliver the various types of services, as described in detail in the next section.
5Analysis of resources and their use according to the proposed classificationThe change to the offer structure described previously considers ordinary hospital beds as a homogeneous category, possibly only making a distinction between acute-care and long-term/rehabilitation patients. Studies using these parameters do not factor in the resources used for inpatient care, and their results may be distorted due to the grouping by medical disciplines. Reclassification of hospital beds on the basis of type of inpatient care, on the other hand, reveals differences according to these categories. We provide below the results of the analysis of the historical series for the period 2007–2013, for which the Ministry of Health has issued precise data on inpatient activity by hospital.
5.1Number of beds – intensive careThe demand for intensive care covers all types of urgent and non-deferrable admissions. This characteristic, besides suggesting the need for homogeneous distribution of resources across the national territory, proportionate to the resident population, requires that the service be able to meet demand for this type of care relatively rapidly. This type of admissions includes the Intensive Care Unit, the Coronary Care Unit and the Resuscitation Unit.
Table 8 shows that the beds allocated to this type of admissions are evenly distributed across the national territory and their number has not changed over time, except for the Regions of Central Italy.
The average length of stay in intensive units varies by 1–2 days between the country's macro-areas (Table 9). The changes over the 6-year period are significant only in Southern Italy, where the trend is towards faster discharge of patients from intensive units.
From the viewpoint of geographical accessibility, since urgent admissions cannot be deferred, the intensive units tend to be sized and distributed over the territory so as to ensure fast access and reasonable travel distance. This distribution discourages patient admissions outside their Region or Province of residence; this requires local authorities to provide a number of beds proportionate to their resident population. Therefore, the different discharge rates observed between macro-areas of the country (Table 10) are likely to be due to different reasons from the availability of beds; this issue deserves further investigation.
With regard to the complexity of the cases treated in intensive care units, the differences between the country's macro-areas is less pronounced, especially if we consider the data for 2013, partly due to the marked drop recorded in the hospitals of Northern Italy and especially of Southern Italy, respectively of 9.9 and 11.3 percentage points (Table 11).
Distribution of hospital department by ICM >1 – intensive care.
| ICM >1 | Δ 2007–2013 | |||
|---|---|---|---|---|
| 2007 | 2010 | 2013 | ||
| North | 50.0% | 47.2% | 40.1% | −9.9 |
| Central | 48.0% | 44.5% | 36.7% | −11.3 |
| South | 33.8% | 29.9% | 36.7% | 2.9 |
| Italy | 43.1% | 39.8% | 38.0% | −5.1 |
Source: Authors’ elaboration on data from “Ministero della Salute”
Lastly, it is felt that for intensive care admissions, service planning should take into account both an adequate degree of level service accessibility and the availability of an adequate number of beds for intensive units. Given the high use of resources by intensive units, beds in those units should be distributed proportionally to the catchment area and should be located within 60minutes’ travel time.
5.2Number of beds – specialised careSpecialised care beds concern specialties such Neurology, Ophthalmology and all kinds of surgery, except for General Surgery.
For these disciplines, service streamlining seems to have yielded good results, with uniform distribution over the country's macro-areas, as shown by the data in Table 12.
Southern Italy has fewer beds of this type than the rest of the country, but its average length of hospital stay is edging closer to that of the other macro-areas (Table 13).
The amount of travel for this type of hospital stays is affected by the strong reduction in resources, especially in Southern Italian Regions, where weakening of the level of specialisation risks affecting economies of scale and of learning. In particular, over the 6-year period, the drop in the number of beds recorded in Northern Italy (−10%) was reflected in a 12.3% reduction in discharge rates, while the sharper drop in bed numbers in the South (−20%) led to a 20.3% contraction of the discharge rate, hence a difference of 7 percentage points. (Table 14)
With regard to the complexity of the cases treated in specialist care units, the differences between the country's macro-areas are more pronounced, especially in Southern Italy compared with Northern and Central Italy. While in Central and Northern Italy half of hospital departments have a case-mix index higher than 1, in Southern Italy this threshold value is only exceeded by one third of specialist departments (Table 15).
For this type of inpatients, the service should be sized so as to ensure local availability of the service but with a degree of reachability of facilities different from intensive care units. In this case, since the treatment in question is not on an urgent/emergency basis, the requirement of less than 60 minutes’ travel time need not apply, and greater flexibility in resource distribution is possible. This flexibility makes it possible to estimate the possible effects of concentrating resources in limited areas of the territory and of developing centres of excellence that work as hubs supporting the regional hospital network.
5.3Number of beds – basic careThe basic healthcare areas include General Medicine, General Surgery, Gynaecology and Obstetrics and basic departments, also present in small hospitals, for healthcare needs not requiring intensive or specialised care.
Similarly, to specialist beds, the number of basic care beds too has incurred significant cuts in the six years under consideration (Table 16). In this case too, Southern Italy shows stronger changes than the national average, of −21.4% over the period examined.
The uniform downward trend in the number of beds has not been accompanied by a parallel change in the average length of hospital stay (Table 17). Thus, the reduction recorded in the Regions of Central Italy, as well as the increase in Southern Italy, do not imply any significant change in the operational management of resources.
The reduction in beds belonging to the basic disciplines, albeit substantial across the country, has maintained over time an imbalance in favour of the North and Centre vis-à-vis the South. The local availability of inpatient beds is essential to meet primary needs and to ensure continuity of care with community-based medicine. A decrease in discharges is observed across the country (Table 18). This is certainly the outcome of the drive to replace as much as possible inpatient care with home and community-based care launched with the reform of 1992, but reductions as marked as in Southern Italy are only partly attributable to reorganisation of the healthcare system. In 2013, the South differed by almost 12 percentage points from the North and by 15 points from the centre; this difference is likely to be due to gaps in basic services or to the local population's lack of confidence in the quality of locally-available health services.
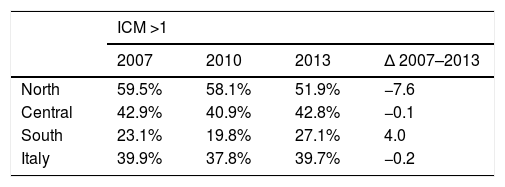
The level of complexity of the cases handled in the basic departments is especially imbalanced in the country's three macro-areas; the weight of complex cases decreases steadily moving from the North to the South of the country. Only 27% (2013) of basic healthcare departments in Southern Italy have a case-mix >1, against 42.8% of the Centre and no less than 51.9% of Northern Italy (Table 19).
Lastly, for this type of services, planning should target full coverage of the territory and adequate travel time. Although this type of care is not urgent, the level of geographical proximity and the availability of beds have a heavy impact on public perception of the quality of the local health service, and hence on choice of treatment facility. Thus, satisfying both elements at the same time can be an effective management strategy to reduce the mobility of patients between Regions.
5.4Number of beds – rehabilitative careRehabilitative care belongs to all post-acute admissions that involve a length of hospital stay exceeding 7 days. This class includes functional rehabilitation, haematology, haemodialysis and disciplines not requiring immediate or specialist intervention but nevertheless requiring a longer hospital stay than other types of admissions.
The number of beds in this category has not changed over time across the country's macro-areas (Table 20) and is highest in Northern Italy.
The average length of hospital stay in rehabilitation units is markedly higher than the length of stay in the preceding groups of disciplines (Table 21). For this class, average length of stay is also markedly longer in the North compared to Central and Southern Italy. The gap is widest between the North and the South, despite the 17% increase recorded in the South between 2007 and 2013.
As concerns the Discharge Rate (Table 22), the differences recorded over time do not appear to stem from changes in the availability of services. An exception is found in the South, where despite the number of beds being largely stable and average length of hospital stay being below the national average, the effect on the discharge rate is of a progressive reduction which lowers the index to 2.5×1000 inhabitants against 3.8 in Central Italy and 6.4 in Northern Italy.
This phenomenon might reflect the early effects of the economic crisis that reversed the migration flow, triggering a movement from the North to the South. This might have led to replacement of part of inpatient care with home care.
Lastly, as to the level of complexity of the cases handled in the rehabilitation departments, in this case too, and with a steeper curve, the weight of complex cases decreases steadily moving from the North to the South of the country. In this category, 20.7% (2013) of departments in the South have a case-mix >1, against 38.8% in Central Italy and 41.5% in Northern Italy (Table 23).
These figures show clearly that planning for rehabilitation units requires fewer beds compared with other types of inpatient care (0.3×1000 inhabitants), given the limited use of this category of hospital services (4.5×1000 inhabitants). Nevertheless, the average length of stay, which is 20 days, requires a high amount of resources with respect to speed of turnover. Therefore, planning of this type of service should be reviewed to make it available and accessible evenly across the country but also to organise it so as to facilitate transfer from hospital care to other care facilities, under the criterion of continuity of care.
6The 2SLS modelAnalysis of geographic differences of the Italian healthcare system must be completed by an analysis of geographical differences in lifespan. The question we addressed using a two-stage least squares (2SLS) regression model is whether geographical difference in health services and in social conditions can explain lifespan differences between Italian Regions.
Thus, a 2SLS model was built, using as dependent variable average age at death in each Italian Region and using two predictive variables, which are accessibility of health services and quality of welfare and care services, plus some technical variables linked to social conditions: inequality index, satisfaction, overweight level and per capita income. The data used are those published by the Italian Institute of Statistics (ISTAT) in its Indagine sul benessere equo e sostenibile delle regioni italiane (Survey of equitable and sustainable well-being in Italy).
The model can be written in the following form:
where Cancermortalitydeath is the rate of cancer mortality and healthservicesquality is the quality of health services.
The description and the outputs of the 2SLS model are described in Tables 24–27:
Model description.
| Type of variable | ||
|---|---|---|
| Eq. (1) | ageatdeath | Dependent |
| Cancermortalitydeath | Predictor | |
| healthservicesquality | Predictor | |
| procapiteincome | Instrumental | |
| Inequalityindex | Instrumental | |
| Satisfaction | Instrumental | |
| overweightindex | Instrumental |
Model summary.
| Eq. (1) | Multiple R | 0.613 |
| R Square | 0.376 | |
| Adjusted R square | 0.306 | |
| Std. error of the estimate | 1.097 |
ANOVA.
| Sum of squares | df | Mean square | F | Sig. | ||
|---|---|---|---|---|---|---|
| Eq. (1) | Regression | 13.038 | 2 | 6.519 | 5.417 | 0.014 |
| Residual | 21.661 | 18 | 1.203 | |||
| Total | 34.699 | 20 |
Coefficients.
| Unstandardised coefficients | Beta | t | Sig. | |||
|---|---|---|---|---|---|---|
| B | Std. error | |||||
| Eq. (1) | (Constant) | 107.106 | 5.034 | 21.276 | 0.000 | |
| Cancermortalitydeath | −0.081 | 0.048 | −0.476 | −1.696 | 0.107 | |
| healthservicesquality | 0.012 | 0.006 | 0.423 | 1.783 | 0.091 | |
The model has a good level of significance and explains regional differences in lifespan in terms of accessibility of healthcare and quality of welfare and care services.
This result confirms the importance of the analysis described earlier in this paper, because it highlights the link between the structure and organisation of the national healthcare system and the final outcome sought, which is to increase people's life expectancy. Efficient and accessible healthcare and care services over the long term increase the lifespan of communities.
Making health services efficient and accessible should be a key goal of economic policy, in order to boost social well-being and ultimately achieve greater cost-effectiveness, as greater efficiency drives down costs by preventing and reducing morbidity.
7ConclusionsThe analysis performed has shown a degree of imbalance between the Regions in terms of resources allocated and of the associated volumes of healthcare activity produced. In particular, study of the structure of the hospital services available, compared with the demand for healthcare shows a mismatch between demand and supply, which is only partly explained by the different geographical and population sizes of the different Regions (Fuchs, 2011; Levaggi & Zanola, 2003). The drive for greater regional autonomy in planning the delivery of health services is hampered by local and national healthcare budget constraints. To attempt to address this contradiction, the National Government has decided to intervene in operation of Regional Health Services, by agreeing with certain Regions actions to reduce immediately their financial deficit. The Regions undergoing review of their healthcare structure are mainly those of the South, which in addition to having a high budget deficit also have fewer beds×1000 inhabitants compared with the rest of the country. The lower healthcare delivery capacity quickly triggers a decline in the demand for care in the area concerned. This in turn feeds the phenomenon of patient mobility (recourse to other facilities) both within and between Regions. In both cases, this phenomenon triggers a decline in the technical quality of care and operational efficiency of local health services, deepening the budget deficit of Regional authorities. Faced by this vicious cycle, regional policy-makers often choose to reduce the services available (Marino, Miceli, & Quattrone, 2018).
Combining the data on the availability of services with those on their degree of use, significant differences emerge between the various areas of the country. In the south, the number of inpatient beds per 1000 inhabitants is lower than in the other macro-areas. The gap is widest for specialist, basic and rehabilitation medicine. Specifically, as concerns rehabilitation medicine, the number of beds per 1000 inhabitants has not changed over time but is accompanied by shorter average length of hospital stay in the South. This phenomenon, which marks a sharp difference between Northern and Southern Italy, could be due to greater involvement of family members at the time of discharge of rehabilitation patients, as shown by the lower discharge rates in these Regions.
Moreover, the present structure of the healthcare system generates lack of confidence, which feeds the vicious circle of patients seeking healthcare outside their Regions, a phenomenon mainly found in Southern Italy, which reduces potential development in this sector.
This analysis does not apply to intensive care units, where the type of demand is unlikely to be affected by the structure of supply. Nevertheless, the analysis shows that the Regions of Southern Italy are more likely to have this type of admissions. This aspect should be investigated further to assess whether these differences stem from the organisation of the service or from other than management reasons.
In conclusion, this study attempts to provide an alternative reading to “sector studies”, to highlight more clearly the extent of the “healthcare mobility” phenomenon and the role of the supply structure as a driver of this phenomenon.
The problems discussed here are a direct consequence of the local organisation of the healthcare system. These remarks should serve as inputs to healthcare policy-makers, to assess whether the service should be planned at the regional level or whether it might be more effective to consider a structure in which local autonomy is not pursued via budgetary criteria.

