


Management of patient records in a hospital is of major importance, for its impact both on the quality of care and on the associated costs. Since this process is circular, the prevention of the building up of bottlenecks is especially important. Thus, the objective of this paper was to analyze whether the Theory of Constraints (TOC) can be useful to the logistics of medical records in hospitals. The paper is based on a case study conducted about the 2007-2011 period in the Medical Records Logistics Service at the Hospital Universitario Virgen Macarena in Seville (Spain). From April 2008, a set of actions in the clinical record logistics system were implemented based on the application of TOC principles. The results obtained show a significant increase in the level of service and employee productivity, as well as a reduction of cost and the number of patients’ complaints.
In this section, we describe the process of logistics of medical records and the management tool that was used to improve it: the Theory of Constraints.
1.1Medical recordsIn spite of the fact that medical records (MR) are involved in several roles (Tejero Álvarez, 2004), such as research, teaching, and planning, priority lies with the healthcare purpose, for which it is important to efficiently manage records in order to guarantee case follow-up and, therefore, proper medical care of patients. Although the trend in this field is the replacement of the physical files by electronic patient records systems (Waterson, Glenn, & Eason, 2012), physical support records are still common, implying a logistics management of material flows. In such cases, a key element for this objective is to maintain efficient logistics of clinical documents that ensure the presence of medical records right where and when they are needed in the most effective and efficient way. In fact, is the same logistic problem that has the materials management service (Aguilar-Escobar, Bourque, & Godino-Gallego, 2015)
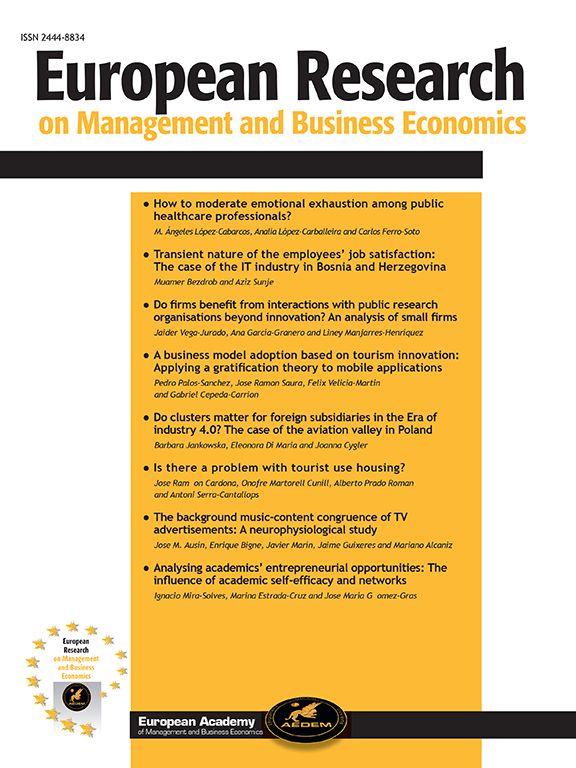
In MR management, the goal is to maximize the number of MR delivered to the clients in time (doctors are the internal customers in this process). As can be seen in Fig. 1, MR logistics involve lending out the MR to medical services and then taking these MR back to the storage area. This can be divided into four processes: preparation for MR to be lent out for consultations, MR delivery to medical services, its collection, and storage. It is, therefore, a process of a circular nature because, to make it possible to prepare new consultations, MR must be taken back by the medical services and properly stored. Circular processes are common in lending activities, such as libraries, rent-a-car, video-clubs, and even include certain financial activities. In healthcare, it is also the case of the central sterile services department. In these cases, the prevention of bottlenecks is especially important because, once one is formed, other parts of the process then suffer from that constraint.

Another singularity of the MR process is that the agents of the process could react to the constraint by making their own decisions, which usually exacerbate the problem, thereby creating a vicious circle. This situation is possible since certain agents (middle managers, i. e. doctors) have the authority to make decisions that affect the system as a whole.
The presence of these two characteristics together renders bottleneck management as a critical issue.
1.2The Theory of Constraints (TOC)From the perspective of logistics, the challenge to be faced is similar to that in any economic activity and the goals are also the same: the improvement of service, the reduction of costs, and the increase of client satisfaction (Aguilar-Escobar & Garrido-Vega, 2013). In order to meet such a challenge, several methodologies have been applied (Simón Martín, Flores Varela, & Arias Coello, 2010; Moro Cabero, 2011). In the business management field, various approaches have been developed for the improvement of management, such as MRP, Lean, and Theory of Constraints (TOC), among others (for a comparative analysis of these three approaches, see Gupta & Snyder, 2009). The Theory of Constraints (TOC) is based on eliminating the restrictions of the system (or bottlenecks), which prevent the productive flow from being able to satisfy the demand. TOC philosophy appeared in the 1980s from the evolution of a previous version in the production/operation area, called Optimized Production Technology (OPT). OPT was initially created as a scheduling software program (with a secret algorithm) in 1980 by Eliyahu Goldratt and was quickly applied in western companies (Goldratt & Cox, 1992). A few years later, the nine OPT rules upon which this program was based was released (Goldratt & Fox, 1986). Since then, this technique has evolved from a production programming method to a management philosophy (TOC), which can be useful for ascertaining and improving the performance of complex systems (Gupta, 2003; Watson, Blackstone, & Gardiner, 2007; Naor, Bernardes, & Coman, 2013). TOC can be analyzed from two different perspectives: organizational system management and ongoing quality improvement (Siha, 1999; Gupta, 2003).
From the first perspective, TOC remarks that every organization has a final objective, a goal, and it can be understood as a number of inter-dependent events subjected to fluctuations, in such a way that the system's global performance at any given moment is always constrained by a number of factors: bottlenecks.
As regards the second perspective, TOC proposes a number of tools for ongoing quality improvement of the system, from among which two are worth bearing in mind (Siha, 1999): effect-cause-effect (ECE) diagrams, and the five-focusing-steps (FFS) process. ECE diagrams form part of the “Thinking Processes” tools, introduced by Goldratt in 1994 in his book “It's Not Luck” (Watson et al., 2007), which are aimed at rigorously and systematically identifying unstructured problems related to management policies. Since ECE diagrams are not used in this case, this tool will not be discussed further.
The FFS technique is a methodology described by Goldratt in his book “The Goal” in 1984 (Watson et al., 2007) designed as an ongoing problem-solving process, and consists of: 1) identifying the constraints of the system; 2) deciding how to exploit those constraints; 3) subordinating all the other parts of the system to the previous decision; 4) elevating the constraints of the system; and 5) returning to step 1, while striving to prevent inertia. Each of these phases are briefly explained below.
Phase 1: TOC considers a constraint as any area, process, or specific element of a system which prevents its performance from being increased and its goal from being reached. Typically, the factors acting at any moment as a constraint number either only one or just a few. These constraints may be external (from suppliers or customers) or internal. The latter are of two types: physical, when they are due to a lack of resources; and political, when they are brought about by inefficient procedures or policies. To identify constraints, TOC starts by identifying a number of undesirable effects (UDEs).
Phase 2: The purpose in this phase is to maximize efficiency of the present constraint, by concentrating efforts on eliminating those activities involving waste or loss of time in the constraint. In this phase, actions are generally focused on making organizational changes in those procedures and policies that imply no economic outlay. The aim is to make the most of the bottleneck-factor potential, although this is usually insufficient to eliminate the constraint, as we will see later.
Phase 3: This phase implies synchronizing the operations in other non-bottleneck processes or elements of the system so that they will not provoke any setback in the use of the constraint. Like the previous step, this usually involves changes in policies and procedures without incurring additional significant expenses.
Phase 4: If steps 2 and 3 are insufficient to eliminate the constraint, then the solution is to increase the bottleneck potential, which was performed in this case. This action involves incurring expenses and making an investment.
Phase 5: If the constraint disappears as a result of the previous steps, it will be necessary to return to step 1, because there will be, without a doubt, another constraint emerging either inside or outside the system. Likewise, it is also necessary to pay attention and prevent the system from returning to the previous configuration due to inertia, which is extremely common in all systems.
One of TOC strengths, as opposed to other improvement approaches tending to optimize performance in each area of the system (such as TQM, Six Sigma and Lean), is that it is based on systemic thinking, by focusing improvement efforts on critical components of the system (Reid, 2007).
TOC has been successfully implemented in a number of organizations, mainly in manufacturing companies (Mabin & Balderstone, 2003; Chou, Lu, & Tang, 2012), its application remains much more reduced in services (Reid, 2007; Cox & Schleier, 2010; Nowakowska-Grunt & Moroz, 2013). In spite of this, services offer major room for improvement through applying TOC concepts and tools (Cox & Schleier, 2010). It is true that services present certain unique characteristics which must be taken into account when TOC is applied (in performance measures, in the nature of the constraints, etc.) and these characteristics depend to a great extent on the type of service (Siha, 1999). Although scant, among all service industries, it is in the healthcare sector where TOC applications have been more extensively developed (Ronen & Pass, 2010). Goldratt himself envisaged that TOC principles were perfectly applicable to healthcare (Goldratt & Fox, 1986). In this field, apart from some theoretical contributions (Motwani, Klein, & Harowitz, 1996; Breen, Burton-Houle, & Aron, 2002; Young, Brailsford, Connell, Davies, Harper, & Klein, 2004; Wright & King, 2006; Ronen, Pliskin, & Pass, 2006; Aoki, Ohta, Kikuchi, & Oishi, 2008; Sadat, Carter, & Golden, 2013), to the best of our knowledge, research has been mainly aimed at patient-flow management (Womack & Flowers, 1999; Rotstein, Wilf-Miron, Lavi, Seidman, Shahaf, Sharar, Gabay, & Noy, 2002; Umble & Umble, 2006; Stratton & Knight, 2010), although other studies have dealt with different areas, such as budget management (Taylor and Churchwell, 2004) or health technology assessment (Groop, Reijonsaari, & Lillrank, 2011).
This work focuses on studying the applicability of TOC principles to MR management, and constitutes unprecedented research in this field. Specifically, the following research questions arise: Can Theory of Constraints constitute an appropriate approach for the improvement of the management of medical records, and in general of the management of circular logistics processes? Why? If appropriate, how should TOC be applied in these cases?
Our study is structured as follows: Section 2 explains the case study methodology in use; further details are given of the results achieved in this case (section 3); these results are discussed in light of the application of TOC techniques and principles (section 4); and the paper then finishes by setting out the conclusions of the study (section 5).
2MethodsDue to the exploratory nature of our research and its mainly explanatory purpose (based on “how” and “why” questions), case study research methodology has been chosen (Barratt, Choi, & Li, 2011). Case studies are the most convenient research strategy when: a) “how” and “why” questions are addressed; b) the researcher has little control over events; and c) the focus is a contemporary phenomenon within some real-life context (Yin, 2008). The main advantage of the case study is that it enables a phenomenon to be intensively studied over time within its natural context.
To conduct this research, we have tried to follow the methodological recommendations for inductive case studies compiled by Barrat et al., 2011) from research in various subjects. They identify the following steps: 1) Justification of research approach; 2) Research focus and specification of unit of analysis; 3) Research purpose and role of existing theory; 4) Sampling issues, case selection, and number of cases; 5) Data collection and analysis; 6) Organization of results; and 7) Presentation of research outcomes. Thus, after justifying the research approach (step 1, immediately above), and with antecedents having been analyzed in the previous section (step 3), in this section we focus on explaining the questions related to the unit of analysis (step 2) and sample (number and selection of cases) (step 4), as well as the sources to obtain the data (step 5). The last two steps are covered in the following sections.
In order to ensure rigor in the research in field studies, including case studies, four criteria are often used (Gibbert, Ruigrok, & Wicki, 2008) internal validity, construct validity, external validity, and reliability. Reliability is associated with the elimination of random error, while validity refers to the non-random or systematic error. Various measures have been proposed to ensure or control each of these quality criteria, which are applicable in different stages of research (Yin, 2008; Gibbert et al., 2008) Thus, in this study, the external validity will be considered in the stage of sampling and case selection (Section 2.1), reliability and construct validity in the data collection stage (Section 2.2), and internal validity in the data analysis stage (Section 4).
2.1Unit of analysis and selection of case study: Hospital Universitario Virgen Macarena.The study of one case was carried out for this research. This type of research design presents the advantage of capturing, in greater detail, the context within which the phenomenon under study takes place, and it is also useful when the purpose is to carry out a longitudinal study (Barratt et al., 2011). The case chosen was the Hospital Universitario Virgen Macarena of Seville, Spain (HUVM), because it was in this hospital where a re-engineering process of its logistics system, based on the use of TOC concepts, took place starting in 2008. Choosing this hospital is justified from a theoretical point of view: it is a typical case of a Spanish public hospital similar to many others, while representing a unique case, because this hospital is the first to use TOC concepts in its MR logistics management. This selection has therefore been made while considering the external validity or generalizability of the study, that is, the possibility of extending the conclusions beyond the actual case analyzed.
The unit of analysis is the MR storage and management service in the aforementioned hospital. The time span of the case study is from 2007 to 2011, that is, from the year before the implementation of the plan to the last year that provided data concerning the service level (2011). As a whole, the HUVM deals with a population of about 525,000 and consists of two hospitals, three specialty centers and other minor centers, with 955 hospital beds and 27 operating theaters. From the MR Service viewpoint, around 3,200 MR requests for consultations were dealt with on a normal day in 2011, although this average goes down in summer months and holiday periods due to lower demand.
2.2Data collection and research variablesThe main data sources used for this research work include: structured interviews, the hospital's internal and external documents, direct observation work, and participant observation.
Regarding the interviews, two were carried out with the hospital's middle managers (Chief of Medical Records Logistics Service and Chief of consultation preparation process) using open questionnaires. On average, each middle manager was interviewed for a total of four hours distributed over three interviews. In these interviews, several aspects of the MR logistic process were addressed, including the description of the process, the chronology of the changes, and the results obtained. The consulted documents mainly refer to economic and logistic data. Direct observation was carried out through visits to the MR storage area and MR delivery points. Finally, participant observation was also performed since one of the researchers was employed as the hospital economic-administrative director and, therefore, as head of the clinical record logistics, during most of the period under study (April 2008-September 2010). Although this investigation was carried out several years after the period under study, this participation can be considered another source of information. While this source of evidence may have introduced potential bias into the study, it also brings with it significant advantages, such as the opportunity it provides in gaining access to otherwise unattainable information.
This multiplicity of sources was used in an effort to achieve data triangulation to enhance reliability and validity (Yin, 2008). The fact that three researchers have participated in the collection and analysis of data implies yet another type of triangulation to ensure construct validity, which refers to the quality of conceptualization of these variables. The main variables in this study, as discussed in the Results and Discussion sections, on the one hand refer to those actions or interventions in MR management enacted following the TOC approach, and, on the other hand, to the performance of this MR service.
Moreover, a hermeneutic unit for the case study was created in Atlas.ti version 7, with all the documents, photos, and summaries of the interviews, and with the bibliography. This allowed the coding of the aspects identified in each document and the search for relationships between these aspects. This could facilitate the replicability of the study, which is a key aspect to ensure reliability.
3Results3.1Initial situation of the Medical Records Logistics ServiceBy early 2008, the HUVM management was concerned about the operation of the medical records service. The interviews we conducted revealed the existence at that time of serious problems, including:
- 1)
Three warehouses in different locations, all with different archiving systems, and all of these warehouses were saturated.
- 2)
A significant delay in the archiving of medical records.
- 3)
A lack of confidence in the medical records logistics service shown by many hospital services, which led to many records being retained and even to the development of these services’ own archives.
- 4)
The high risk to patient care due to the lack of records.
- 5)
The duplication of many records for the same patient, even in separate locations.
- 6)
The inflexibility in the computer system in generating reports.
- 7)
A complete lack of measurement of performance parameters. The number of complaints from the patients was high.
- 8)
A general feeling of dissatisfaction with the medical records service among physicians and patients.
- 9)
A lack of motivation and feelings of frustration at the problems by the medical records service staff.
- 10)
The large number of passive medical records and obsolete documents in the warehouse.
When, in April 2008, it was decided that the Logistic Services Clinical Documentation fell under the economic-administrative management, a baseline analysis was conducted in order to identify areas for improvement. Within this analysis, performance evaluation indicators, previously non-existent, were established (e.g. percentage of orders of medical records not served), and work environment and physical conditions of the warehouse were checked.
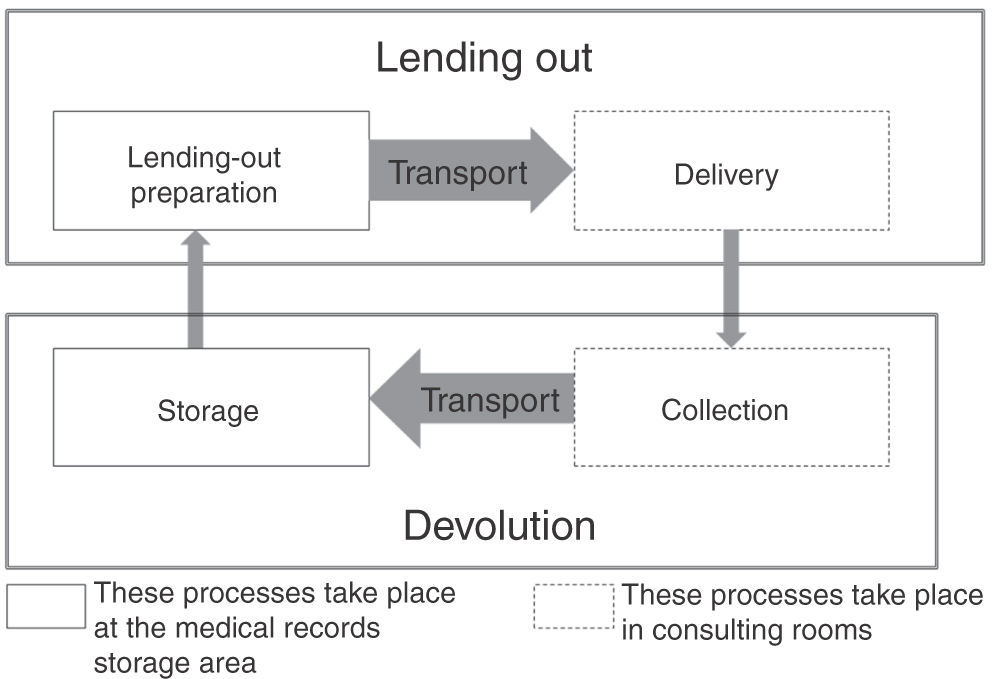
3.2Final situation of the Medical Records Logistics ServiceUpon application of a series of TOC-philosophy-guided interventions, which will be described in the following section, the status of the medical records service showed a number of major improvements as reflected in the following figure and tables.
The average daily number of potential undelivered MR (latent risk) was reduced between 2008 and 2011 (Fig. 2).
.")
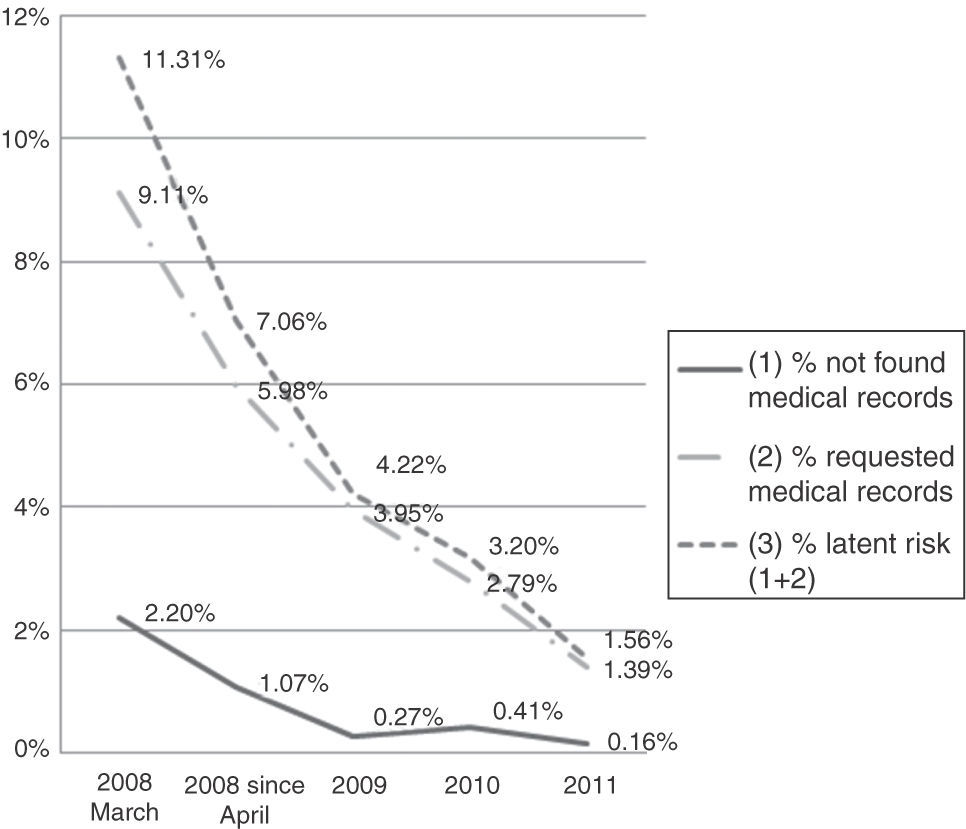
Table 1 shows how the number of complaints has decreased since 2009, starting from a previous situation (2005-2008).
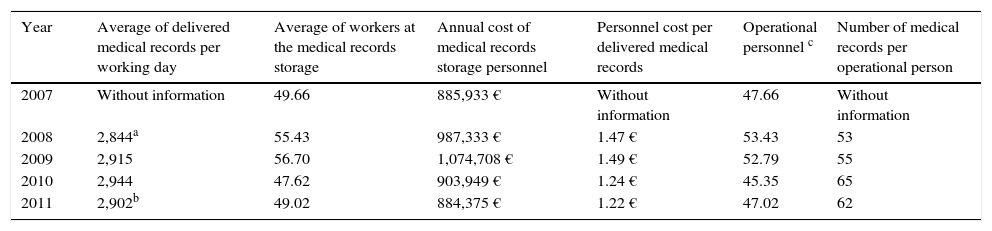
Finally, Table 2 reveals how the daily productivity ratio (number of delivered MR per employee- Stratton & Knight, 2010) has risen during the period under study, especially during the last two years involved.
Personnel cost per delivered medical records and productivity ratio (2007-2011).
| Year | Average of delivered medical records per working day | Average of workers at the medical records storage | Annual cost of medical records storage personnel | Personnel cost per delivered medical records | Operational personnel c | Number of medical records per operational person |
|---|---|---|---|---|---|---|
| 2007 | Without information | 49.66 | 885,933 € | Without information | 47.66 | Without information |
| 2008 | 2,844a | 55.43 | 987,333 € | 1.47 € | 53.43 | 53 |
| 2009 | 2,915 | 56.70 | 1,074,708 € | 1.49 € | 52.79 | 55 |
| 2010 | 2,944 | 47.62 | 903,949 € | 1.24 € | 45.35 | 65 |
| 2011 | 2,902b | 49.02 | 884,375 € | 1.22 € | 47.02 | 62 |
Faced with the initial situation of the medical records service described in Section 3.1, the hospital economic manager decided to implement TOC as the quality improvement approach. Among TOC tools and techniques, the manager chose those linked to the ongoing quality improvement perspective and, specifically, the five-focusing-steps (FFS) method. Previous to its implementation, it requires (Ronen et al., 2006): 1) a decision regarding the system's goal, and 2) establishment of global performance measures.
Although TOC represents a global management approach for the organization, it can also be implemented in sub-systems or specific processes, as long as the goal of the latter is perfectly in line with the goal of the whole system or organization (Reid, 2007). In the case of a public hospital such as HUVM, the goal is to maximize the high-quality medical service provided to customers, at present and in the future, subject to two conditions: meeting budget constraints, and providing safe and satisfactory working environments to employees (Reid, 2007; Ronen et al., 2006; Sadat et al., 2013). So that the performance measures in MR could achieve the final goal, three operational measures were considered: customer satisfaction, delivery date compliance, and operational expenses. In this way, we can say that an action is correct, and therefore leads to the goal, if customer satisfaction and delivery date compliance increase, and/or operational expenses decrease.
- a)
Phase 1: Identifying the constraints of the system
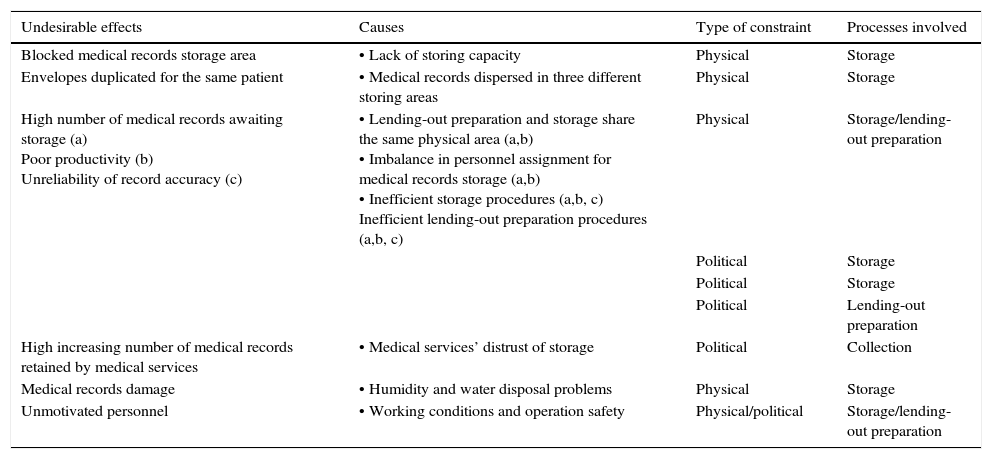
When tackling the initial situation of MR at the HUVM in April 2008, a major lack of awareness was observed of the scope of the problem as there were scant performance assessment indicators. In view of the situation, a number of these indicators were established, such as the calculation of the daily average of MR that had not been delivered in time, which reached at least 2.2%, clearly showing how far management were from achieving the goal. Further observation of processes, as well as of other established indicators, such as the claims received by storage, the physical conditions of the MR storage areas, and the working environment, led to the identification of a number of what in TOC are called undesirable effects, UDEs (see Table 3 below). The analysis allowed identification of the main causes (Table 3) and, from among these, the determination of the potential constraints or bottlenecks (in bold in Table 3). As can be observed, one process was particularly problematic, where most constraints were found: storage, with both physical and political constraints.
Main problems and constraints in medical records management at March 2008.
| Undesirable effects | Causes | Type of constraint | Processes involved |
|---|---|---|---|
| Blocked medical records storage area | • Lack of storing capacity | Physical | Storage |
| Envelopes duplicated for the same patient | • Medical records dispersed in three different storing areas | Physical | Storage |
| High number of medical records awaiting storage (a) Poor productivity (b) Unreliability of record accuracy (c) | • Lending-out preparation and storage share the same physical area (a,b) • Imbalance in personnel assignment for medical records storage (a,b) • Inefficient storage procedures (a,b, c) Inefficient lending-out preparation procedures (a,b, c) | Physical | Storage/lending-out preparation |
| Political | Storage | ||
| Political | Storage | ||
| Political | Lending-out preparation | ||
| High increasing number of medical records retained by medical services | • Medical services’ distrust of storage | Political | Collection |
| Medical records damage | • Humidity and water disposal problems | Physical | Storage |
| Unmotivated personnel | • Working conditions and operation safety | Physical/political | Storage/lending-out preparation |
Physical constraints resulted in the lack of storing capacity. The demand for the service was growing and room was becoming more and more scarce. Furthermore, there were three storage areas in different centers, which made MR management even more complicated. Furthermore, storage and lending-out preparation shared the same physical area, which prevented them from being carried out at the same time.
Political constraints emerged from the inefficient organization of storage and the imbalance in human resources, due to the assignation of a disproportionately higher number of workers to lending-out preparation for consultations than to taking back the MR to the storage area. Despite the help given by 8 employees from external companies, a daily average of 13,000 MR remained awaiting storage. Emphasis had been placed on one part of the process, that of preparation, which was not the bottleneck, and the result was ineffective effort since, as pointed out by rule 5 of the 9 OPT rules (Goldratt & Fox, 1986), “an hour saved at a non-bottleneck is a mirage”. As a consequence of this, although consultations were prepared, the daily lack of MR rose above 2.2%, plus 9.1% of requested MR to clinical services. Another OPT rule came true here, number 2: “the level of utilization of a non-bottleneck is not determined by its own potential but by some constraint in the system”. Therefore, approaching the goal (i.e. increasing the number of complete MR delivered in time) would not be achieved until the storage process problem had been solved.
Although the ideal is to approach constraints one by one, the managers decided to tackle, almost at the same time, both physical and political constraints.
- b)
Phase 2: Exploiting the system constraint
As far as the physical constraint is concerned, in order to make better use of the storage area, the first step to take was to filter and identify passive MR. An appointment analysis revealed that 97.5% of the requested MR had had an appointment the previous year. Therefore, this was established as the new criterion to distinguish between active and passive MR, which led to 134,515 MR being taken out of storage and the further freeing-up of space. Moreover, it was decided to filter, at least once a year, the MR storage. This measure was taken along with the elimination of sub-archives within an archive, such as that which used to serve particularly big MR, also called “special MR”.
As regards the second source of constraints, political constraints, three measures were taken so as to improve those constraints with the available resources: elimination of compact sliding file cabinets, changes in the codification system (these two measures were essentially aimed at making storing procedures more dynamic), and re-assignment of personnel.
Focusing on the first measure, most MR were filed in compact cabinets with sliding shelves on rails, leaving just one real corridor for normal operations. As other authors pointed out (Tejero Álvarez, 2004), space is more efficiently used with this system, but it is limited to admitting only one worker, since the other corridors of the module must remain closed. The solution was to keep the compact cabinets as fixed shelves by removing several cabinets in each module. This change brought about the loss of some storage space, but time for MR storage was also reduced (as well as that for accessing MR).
The second measure was to adapt all files to the terminal triple-digit system (as opposed to the double-double digit or sequential systems that had previously been used). This system, while allowing for a balanced growth in the storage area, makes storing procedures easier to carry out.
The last measure was to re-assign personnel who had been working in lending-out preparation to be allocated to the storage process, thus increasing the bottleneck process potential and balancing the flow within the system. In a circular process, as is the case here, there are no initial and final phases for the patients’ MR and, therefore, it is important that all processes be balanced in their potential in order to yield a regular flow.
- c)
Phase 3: Subordinating the other processes to previous decisions
In this particular case, the actions taken in this phase would refer to the other two processes presenting difficulties (see Table 3), but were not bottlenecks: lending-out preparation for consultations and taking MR back to storage (collection). The purpose of these actions was to prevent either of these processes from affecting the storage process which, as we should bear in mind, was the bottleneck of the system.
Actions consisted of: 1) restructuring and simplifying MR lending-out preparation procedures; 2) in the case of the taking-back process, carrying out several actions on delayed MR.
In order to prevent this re-assignment of personnel from making the preparation process become a bottleneck, it was decided to carry out process re-engineering from the analysis of some good-practice experiences in storage management. Prior to this, the whole process of preparing the daily MR demands implied three phases and it took one day. Such a complex process required a lot of manpower, since the MR were handled several times before being delivered for consultation. The solution was to simplify the procedure, reducing it to two phases, while consultation carts were replaced, small boxes were introduced, and the preparation area was redesigned. Today's process takes 6hours, one hour to take out all MR of the day, and 5hours to put the 3,200 MR into the small boxes.
The MR taking-back process after consultations also affected the operations of the system. Due to erroneous operations in the storage process, medical services tended to retain the MR of those patients who had another consultation. The MR, being a unique document, prevents any other service from having access to those MR when needed. According to an analysis carried out by the hospital in October 2008, 75% of the non-delivered MR was due to the fact that the records had not been taken back into storage from another service, or from another doctor of the same service. The following actions, among others, were adopted to avoid this dysfunction of the system: setting up daily checks on the accumulated MR by each service and, every now and then, checks on the number of delayed MR (those retained for more than 10 days); collective and individual meetings with the delaying services; establishing MR regulations with a specific section for requesting and lending the records out; fixing specific points at medical services to leave and collect MR; collecting delayed MR still in the possession of the services and eliminating any illicit MR mini-archives in those services.
- d)
Phase 4: Increasing the constraint of the system
It was decided to transform the three storage areas of the HUVM into only one storage area. Taking into account that the aforementioned actions in previous phases could not eliminate the lack of storage capacity and that, due to the storage unification, there was even more need for space, then the constraint was increased, which in this case involved expanding the space for MR storage. This was possible thanks to the freeing-up of space after moving the hospital's consumable supply storage to a logistics platform. In total, the storage space was increased by 1,261 m2, equivalent to 3,396 lineal meters for shelves to hold 261,246 MR. This meant increasing the storage capacity by 100%. In this way, at the end of the expansion process, the HUVM Central Archive had a total area of 6,750 lineal meters and a storage capacity of 519,211 MR.
Moreover, a new working area was made available, and was provided with IT equipment for MR records and storage, and so both processes, lending-out preparation and storage, could be dealt with at the same time. Within a very short time, (only one month and 20 days), this change led to the reduction, to zero, of the number of MR waiting to be filed, for virtually the whole period remaining under study.
As far as political constraints are concerned, since the personnel re-assignment in Phase 1 ended up being insufficient, it was decided to hire more workers temporarily.
- e)
Phase 5: Back to step 1, avoiding inertia
In this particular case, since so many measures and changes, both physical and in policies and procedures, had been carried out, it was necessary for managers to be on the watch. It was especially essential to continue making the most of the storage space, and to keep a constant filter of passive MR. It was also important to maintain order and accuracy in MR location, and to replace the envelopes for others with color codes instead of with numbers, which makes any errors in the storing process easier to detect. Furthermore, it was also important to watch and adjust the new working procedures in the preparation process.
By implementing all these measures, it became clear that the new constraint was to be found on the demand side (external constraint). According to Pretorius (2014), this is the ideal situation, since the best possible constraint location is “the size of the market chosen to be served well”.
- f)
TOC results
In order to analyze the level of success of the changes applied in management and of the measures adopted in the MR logistics service, according to TOC we should check to what extent the system has moved closer to its goal: maximization of the number of complete MR delivered in time. Since we are trying to establish a causal relationship between the application of TOC and results, internal validity is an important issue. Setting this validity implies ruling out other factors that may cause the results rather than the application of TOC. Although this is difficult in a study such as this, the evolution of the results that will be presented next and the connection with the timetable of measures taken allow us to conclude that the results are at least largely due to the implementation of the measures taken following TOC.
Fig. 2 shows how the number of maximum non-delivered-in-time MR (latent risk) decreased after implementation of the changes in the management system. Global Efficiency Index (100% minus latent risk) was at least 98.44% in 2011. Therefore, we can affirm that the system is approaching the goal. In order to properly evaluate the result, we can refer to another recent case (Asensio Villahoz & Vicente Vírseda, 2011), where a Global Efficiency Index of 95% was achieved.
Another piece of evidence that the goal is being approached is the reduction in the number of complaint forms about MR turned in by the hospital patients, as can be seen in Table 1.
As pointed out above, there are two mandatory conditions on approaching the goal. The first is budget restrictions or economic efficiency. In the case under study, the main cost is that of personnel. Table 2 shows the evolution between 2007 and October 2011 of the number of workers, the annual cost of personnel and the personnel cost per medical record delivered. It also shows how both the annual cost and the cost per unit (per clinical record delivered) have decreased since 2010. This improvement in efficiency is better observed in the last column in Table 2, which reveals how the daily productivity ratio (number of delivered MR per employee- Moreno Vernis, 1997) has risen during the period under study, especially for the last two years involved.
The second necessary condition is to create a proper, safe working environment for employees. Let us remember that lack of motivation was one of the undesirable effects found in the previous situation analysis. Along these lines, in addition to the changes in work procedures and in the storage, numerous actions aimed at improving working conditions or operation security were adopted: provision of dressing rooms, establishment of new actions for protection against fire, freeing-up emergency corridors, a new safety ladder, air-conditioning in working areas, significant improvement in the lighting system, new work clothes and security footwear, etc.
5ConclusionsThe main purpose of this research work was to analyze the applicability of the Theory of constraints (TOC) principles to the logistics of clinical documents in a hospital. This experience has clearly shown that they are perfectly applicable, as the MR storage is in fact a circular process, where there are bottlenecks and which needs ongoing improvement in its management. In the case of MR, the interest lies in the constraint being situated on the demand side, which ideally must be completely covered.
The previous analysis provided evidence that, in the period before April 2008, inefficient results were obtained in spite of the intensive use of resources. The results of a comprehensive conception of clinical record logistics and determined action based on TOC appeared satisfactory regarding the goal of the MR management service. Proper service level (less than 1% of lost MR) reached since 2009. Apart from all these achievements, the working and safety conditions of the hospital personnel have also significantly improved. What's more, at the same time, better organization allowed the hospital to reduce personnel, completely eliminate the participation of external companies for the storage internal activities, and increase productivity.
Beyond its application in MR management, whose future depends on digitalization and the extinction of the physical format, the main contribution of this research work is to illustrate TOC application to a previously unexplored field (Young, 2005). This study shows that TOC can be very helpful when processes are circular and that some agents, in the search for their own optimum, may negatively affect the entire service. In particular, TOC improvement tools (especially FFS) have shown themselves to be highly useful in this context. It is also pointed out how the goal and necessary conditions can be defined in the case of a specific service within a public, non-profitmaking healthcare organization (Aguilar-Escobar, Garrido-Vega, & Godino-Gallego, 2013). Finally, the fulfillment was shown of OPT rules that predict, in the case of bottlenecks, their influence on the final results, thereby rendering the actions in non-bottleneck phases useless.
The main barriers faced during the application of TOC to MR management include: the difficulties in incorporating the changes in the culture of the organization in order to make it sufficiently rigorous regarding the new MR management process, and the establishment of the importance that MR has on the whole process of healthcare. This also implied an improvement in the attitudes of the workers of the MR Logistical Service to be more efficient and oriented towards servicing Medical Units and so, contribute towards the patients’ healthcare. Another important obstacle was the retention of MR by some Medical Units that failed to have confidence in the MR Logistical Service. As can be seen, the main barriers are related to cultural and/or attitude factors. The infrastructural and economic barriers were not relevant in this case due to the minor economic impact. This situation could be similar in other medical contexts with significant constraints, such as the aforementioned central sterile services department, and in other situations, such as that of the emergency department, and surgical processes.
Suggestions to overcome these barriers include: First, attain a clear mandate from the CEO in order to be authorized to do whatever necessary to solve the problem. Second, analyze the whole process carefully in order to find the actual constraints and to clarify the location of the problems. Third, learn from the experience of others. Fourth, act vigorously and quickly to achieve success as soon as possible; this will enable you to win the confidence of the professionals. Fifth, explain your project to all the people implied (managers, professionals, workers, etc.) to gain their support. Sixth, make no major technological or infrastructural changes before the manual changes have shown their full potential. And seventh, be persistent in the changes and pay attention to new constraints which will surely appear in the process.
Apart from those limitations of this research work originated by the chosen research methodology (case study), we want to remark that a more detailed analysis of the results of applying TOC could be carried out by studying other applicable performance measures.
Moreover, another possible limitation of this research work, as mentioned in Section 2.2, lies in the first signatory researcher's participation as the economic-administrative director and, therefore, as head of the clinical record logistics during most of the period under study (April 2008-September 2010), which may make the analysis appear somewhat biased. Nevertheless, we have striven to counteract this with the participation of two researchers unrelated to the case and by rigorously applying the research methodology. Furthermore, this circumstance allowed us to manage more and better data and to carry out a deeper analysis than other similar studies.
The authors wish to acknowledge Virgen Macarena Hospital's managers and Medical Records Logistics Service personnel, for their kind help in the production of this study.

