




Mesenteric cysts are uncommon intra-abdominal lesions. They account for approximately one out of every 100,000 hospital admissions in adults and one out of every 20,000 hospital admissions in children, with nearly 60% of cases developing before the age of five.1
They may be located in any part of the mesentery, from the duodenum to the rectum, but they are most commonly located in the mesentery of the small bowel, in particular the ileum.2 There is no clear evidence as to their aetiology; hence, they have been attributed to various causes (congenital, neoplastic, acquired or idiopathic). The most recent classification is based on their origin depending on histological and immunohistochemical findings: lymphatic, mesothelial, urogenital, enteric, dermoid or pseudocystic.3
There are three main forms of clinical presentation. The asymptomatic form is the most common and is incidentally diagnosed in complementary tests and surgical procedures. The indolent form predominates in adults; the most common symptoms are abdominal pain (80%), distension and an abdominal mass (30%–50%). The complicated form (rupture, infection, obstruction, etc.)1 predominates in children.
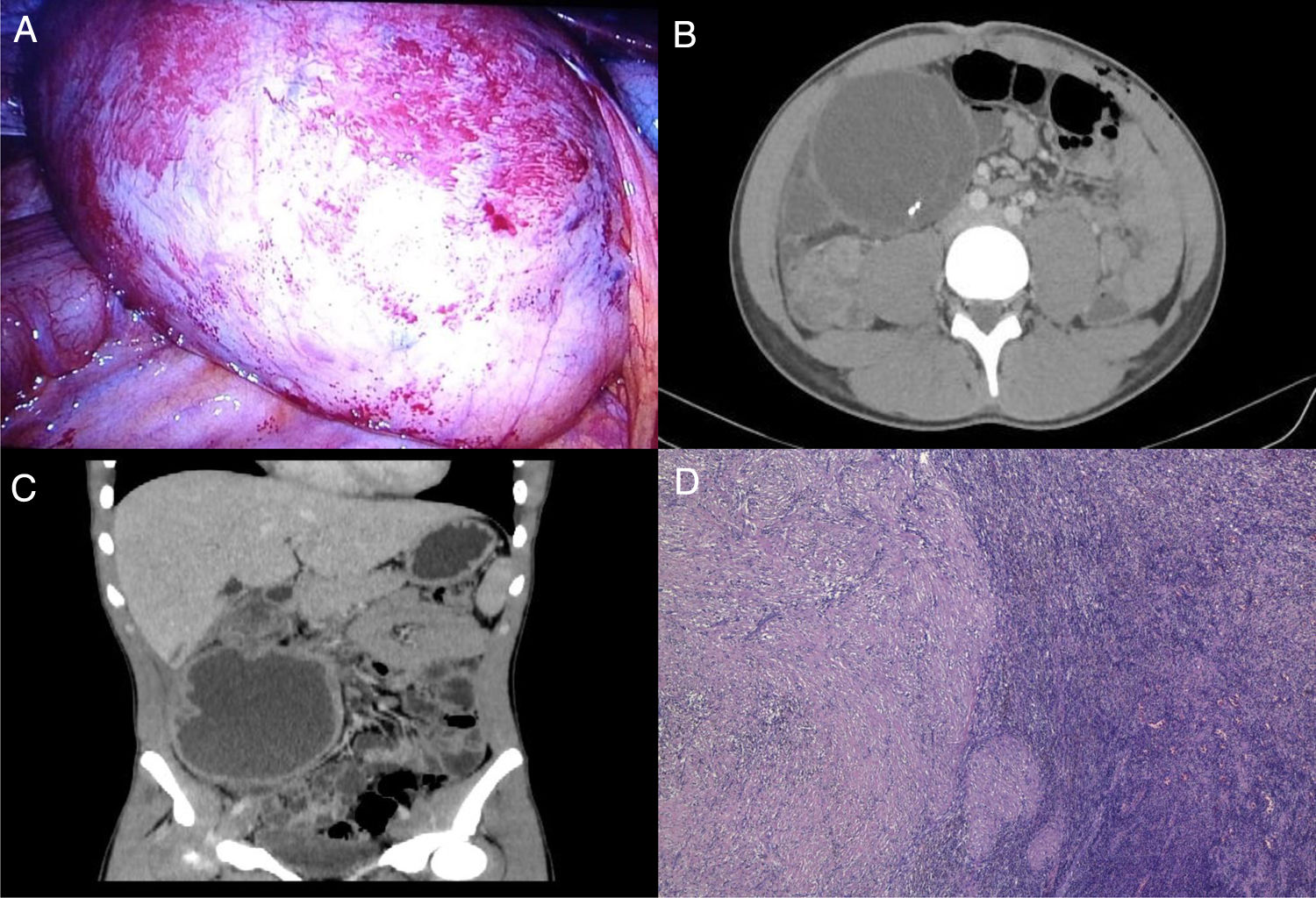
We report the case of a 19-year-old patient with no history of note who visited the emergency department with abdominal pain for the past three days that followed a course consistent with acute appendicitis. Emergency surgery was indicated, yielding the incidental finding of a large mesenteric cyst (Fig. 1A). Laparoscopic appendectomy was performed; the pathology results indicated that the caecal appendix had no histological abnormalities. In the postoperative period, the study was completed with an abdominal computed tomography (CT) scan, revealing a cystic mass measuring 7.7 cm × 10.3 cm × 3 cm in the right flank suggestive of a benign mesenteric tumour (Fig. 1B).
 Incidental finding of a mesenteric cyst during laparoscopic surgery for suspected acute appendicitis. (B) Cystic tumour measuring 7.7 cm × 10.3 cm × 3 cm of apparent mesenteric origin in the right flank. (C) Known cystic mass, with increased wall thickness, suggestive of a complicated cystic lymphangioma. (D) Histology slice viewed under a microscope of the concentric cyst wall with inflammatory infiltrate.")
(A) Incidental finding of a mesenteric cyst during laparoscopic surgery for suspected acute appendicitis. (B) Cystic tumour measuring 7.7 cm × 10.3 cm × 3 cm of apparent mesenteric origin in the right flank. (C) Known cystic mass, with increased wall thickness, suggestive of a complicated cystic lymphangioma. (D) Histology slice viewed under a microscope of the concentric cyst wall with inflammatory infiltrate.
The patient was discharged without incident, then readmitted after 15 days with abdominal pain and persistent fever. A repeat CT scan showed the known mass with complications (Fig. 1C). Percutaneous drainage was performed and a sample of fluid was taken for culture. In the microbiological results, enteric Salmonella, subspecies I, serogroup B, was isolated. The patient did not have diarrhoea, nor did he remember any recent prior episodes thereof. His only notable comment was that he had taken a trip to Morocco a month earlier. Given these findings, a stool culture was ordered and came back positive for the same type of bacteria. The strains were serotyped; both were found to belong to the Typhimurium serotype. Following clinical improvement and ultrasound, the patient was discharged.
One month later, an elective procedure consisting of laparoscopic removal of the mesenteric cyst was performed. A decrease in size and a significant pericystic inflammatory reaction were observed. On the second day, the patient underwent further surgery for suspected bowel perforation, wherein purulent peritonitis and perforation of the transverse colon were detected. Profuse lavage of the abdominal cavity plus primary wound closure were performed laparoscopically. The patient subsequently followed a favourable clinical course. Salmonella was not isolated in the cultures obtained from the resected cyst or in a second stool culture.
The pathology study showed a cystic formation made up of multiple concentric layers, with perforated, abscessed panmural inflammation (Fig. 1D). The immunohistochemistry study was positive for smooth muscle actin and desmin and confirmed a concentric muscle layer, with no traces of epithelial or mesothelial lining observed. These findings were suggestive of an intestinal duplication cyst.
Mesenteric cysts are rare and of varying aetiology. Regardless of their presentation, surgery is the treatment of choice in order to avoid malignant transformation and prevent complications. Cyst aspiration as a sole treatment is not recommended due to high associated rates of recurrence.3
Infection of a mesenteric cyst is a rare complication with few cases reported in the medical literature. The mechanism is usually unknown and may correspond to lymphatic, haematogenous or contiguous spread.4
With the exception of Salmonella typhi, which is responsible for typhoid fever and whose only reservoir is humans, non-typhoidal Salmonella serotypes are found in the intestinal flora of various animal species and are transmitted to humans through contaminated food. Gastroenteritis is the main clinical sign; extraintestinal infections are rare.5
In conclusion, we have reported a rare case of a mesenteric cyst infected with Salmonella typhimurium; we suspected contiguous spread, given its enteric origin, but were unable to rule out lymphatic and haematogenous spread from gastroenteritis. We wish to highlight the importance of proper diagnosis and treatment of this disease, given its rarity.
The authors would like to thank Alicia Blasco and Sandra Vicente (Radiology Department and Pathology Department, respectively, Hospital Royo Villanova [Royo Villanova Hospital]) for their help in selecting images. They would also like to thank Dr Pilar Egido (Microbiology Department, Hospital Miguel Servet [Miguel Servet Hospital]) for her help with serotyping the microbiological samples.
Please cite this article as: Nogués A, Aldea MJ, Cros B, Talal I, Yánez C, Blas JL. Quiste mesentérico infectado por Salmonella typhimurium. Gastroenterol Hepatol. 2022;45:135–136.

Gastroenterología y Hepatología (English Edition) sigue las recomendaciones para la preparación, presentación y publicación de trabajos académicos en revistas biomédicas