




The presence of signet ring cells in the gastrointestinal tract is usually associated with signet ring cell carcinoma, an aggressive, generally gastric disease with poor prognosis, often metastatic. However, that is not always the case. We present the case of a man who had a colonoscopy in the context of lower intestinal symptoms. A number of polypectomies were performed and signet ring cells were discovered in one of them.
There are several different circumstances which can lead to change of epithelial cells to signet ring-type cells, with ischaemia being the most common. It is a process in which the epithelial cells accumulate mucin in their cytoplasm and, consequently, their nucleus moves to the periphery, being left rejected and adopting this characteristic shape. This change is harmless and rare, but it can lead to diagnostic errors due to being confused with the above tumour. The main risk is found in small biopsies, as an incorrect interpretation of these cells can lead to surgery and/or unnecessary treatments.1,2
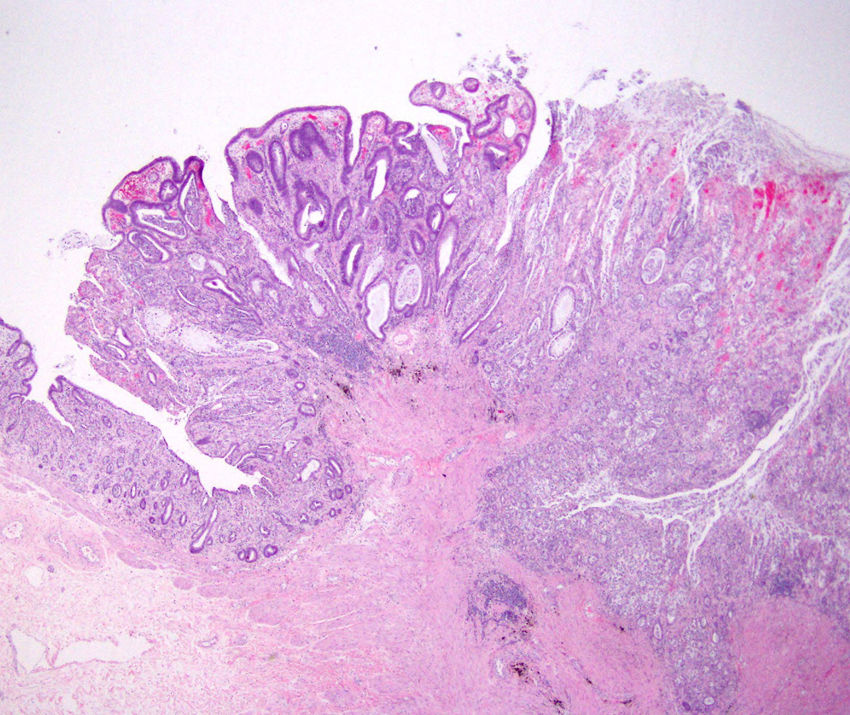
The colonoscopy showed the presence of nine polypoid lesions whose common histological diagnosis was tubular adenomas with mild dysplasia. It stood out that the largest of them (12mm, pedunculated and eroded on the surface) had desquamated signet ring cells inside the glands, in an area close to the ulcerated zone (Fig. 1). Although the examination proceeded without incident, four days later the patient died of multiple organ failure secondary to sepsis of urological origin. Otherwise, the follow-up of this cell change would not have been necessary as it constitutes a benign finding.
. On the left-hand side of the image, colon mucosa can be recognised, with no histological lesions, the central part shows adenomatous transformation and in the right area we can see the presence of signet ring cells occupying the gland lumen.")
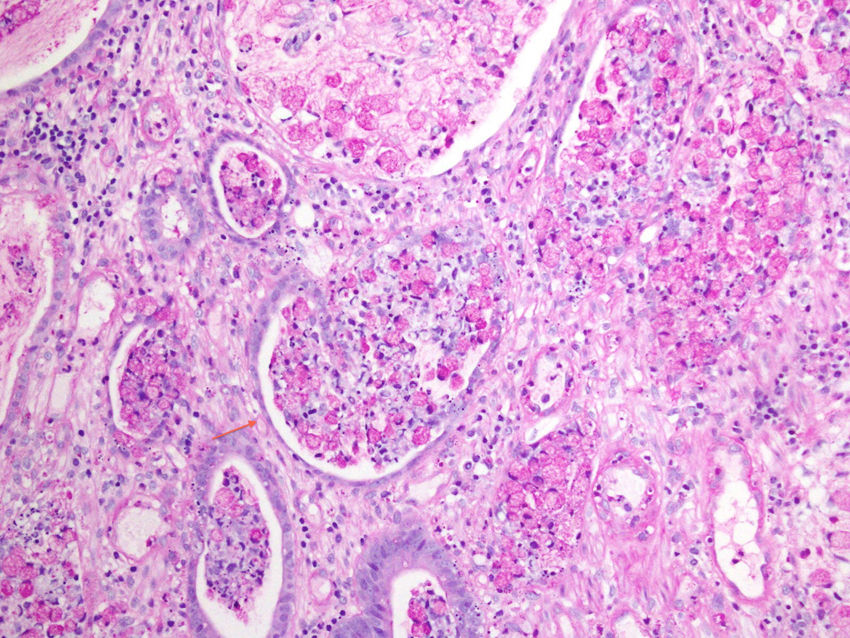
The signet ring cells found were arranged forming nodular collections within the gland lumen (sometimes accompanied by mucin lakes) in the area near the ulcer.3 They did not have cytological atypia, hyperchromasia or disproportion of the nuclear/cytoplasmic ratio. The main characteristics that allowed us to differentiate them as benign were their exclusive presence in the mucosa maintaining the glandular pattern and the absence of an infiltrative pattern. These findings were confirmed by additional histochemical and immunohistochemical techniques. The signet ring cells were positive for pan-keratin and E-cadherin1,2 (Fig. 2).
. The non-neoplastic signet ring cells have cytoplasmic staining for periodic acid-Schiff with diastase (PAS-D). All of them are inside gland lumen. The arrow indicates the basement membrane that delimits them.")
This shape change has been described mainly in the gallbladder and gastrointestinal tract, but also in other organs with epithelial lining such as the cervix and prostate, and its incidence is increasing, creating a significant challenge in terms of diagnosis.1,2 The gastrointestinal disorders with which this condition is most commonly associated are ulcerated adenomatous polyps, ischaemic ileitis, Peutz-Jeghers syndrome and pseudomembranous colitis.1,2 It has also been described in ulcerative colitis, erosive gastropathy, ulcerated mucosal areas of the gallbladder and cystic fibrosis.2
The pathophysiology is not fully understood, but ulceration and fibrinoid exudation have been found in all the cases reported. In mucin-producing mucous membranes such as the one that covers the gastrointestinal tract, the main cause of this transformation is ischaemia, which results in detachment and loss of cohesiveness of the epithelial cells. In such situations where ulceration occurs secondary to ischaemia, in a twisted polyp for example, the consequence is the detachment of the epithelial cells which “balloon”, adopting this shape. Meanwhile, in other processes such as pseudomembranous colitis, it seems to be a consequence of inflammation.1,2
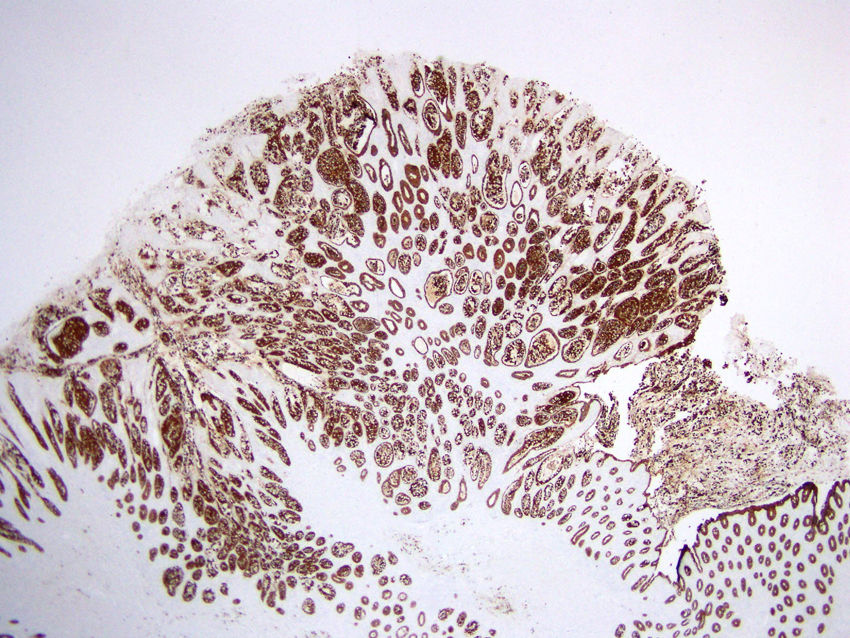
The immunohistochemical studies that help differentiate these two conditions are essentially keratin, E-cadherin, p53 and Ki-67. A benign transformation is generally positive for E-cadherin and pan-cytokeratin, being negative for p53 and having a low Ki-67 proliferation index, while signet ring cell adenocarcinomas are positive for p53 and negative or slightly positive for E-cadherin. We can also use techniques that delimit the basement membrane (PAS-D, reticulin, etc.) to ensure ourselves of the absence of infiltration1–3 (Fig. 3).
. The absence of an infiltrative pattern is demonstrated by pan-keratin staining. All the epithelial cells (signet ring cells and mucosecretory glandular epithelium) are positive and are delimited by the basement membrane.")
It is important to consider the possibility that the cells may be benign when we find this non-neoplastic change of signet ring lesions in the gastrointestinal tract. For that, we can refer to the morphological and immunohistochemical characteristics described above. Correct identification is important, as the prognosis is completely different. This change in shape does not require any follow-up, with the patient's treatment depending on their underlying disease.
Please cite this article as: Zabalza San Martín L, Amat Villegas I. Células no neoplásicas tipo anillo de sello en un adenoma tubular colónico. Gastroenterol Hepatol. 2019;42:348–349.
