




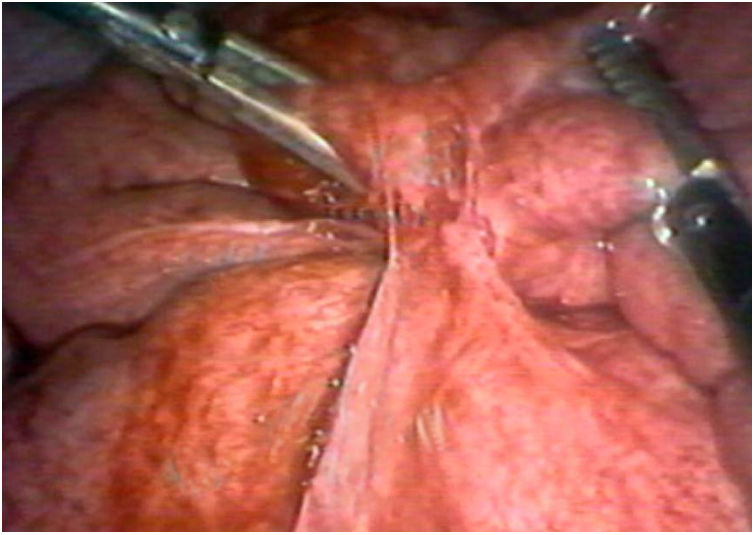
A 24-year-old woman is admitted due to pain in the hypogastrium and right iliac fossa, and vomiting of 48h of evolution. She also has yellowish and smelly vaginal discharge and fever of 38.5°C. There is no previous medical or surgical history and she acknowledges sexual relations with occasional use of barrier contraceptives. The examination shows: heart rate of 110bpm and painful abdomen in the hypogastrium-right iliac fossa, with guarding at that level. Gynaecological examination reveals pain during cervical manipulation, with evidence of the malodorous secretion from which a sample is taken for culture. The blood work shows: haemoglobin 13g/dl; normal corpuscular volume, leukocytes 16,000/mm3 (80% neutrophils), platelets 378,000/mm3, C-reactive protein 55mg/dl; urinary sediment and urine pregnancy test, negative. Simple abdominal radiography shows a generalised dilation of the small intestine. An abdominal, pelvic and vaginal ultrasound is performed that reveals a cystic lesion of heterogeneous content on the right ovary that measures 8×3cm, indicative of ovarian abscess and free fluid in the pouch of Douglas. Complicated pelvic inflammatory disease (PID) is suspected and so the patient undergoes urgent Gynaecological and General Surgery by exploratory laparoscopy, with the intraoperative finding of salpingitis and large right tubo-ovarian abscess of 10cm, with formation of fibrotic adhesions towards the ileum intestinal wall (Fig. 1). Through open surgery, a right salpingectomy, drainage of the abscess, and ileal resection of some 15cm are all performed, with release of pelvic adhesions. Treatment with broad-spectrum antibiotic therapy (intravenous ertapenem) is completed. The microbiological results of the vaginal discharge and the intraoperative sample were positive for Chlamydia trachomatis (C. trachomatis) and Neisseria gonorrhoeae, confirming the diagnosis of complicated PID with a tubo-ovarian abscess and intestinal obstruction secondary to abdominal-pelvic adhesions. The patient is discharged 10h after admission with amoxicillin-clavulanic and metronidazole.

PID is an infection of the upper female genital tract observed primarily in sexually active women. In most cases, the involvement is mild, with symptoms consisting of pelvic pain, but 25% of cases are complicated by the formation of tubo-ovarian abscesses, involvement of neighbouring pelvic organs and, in the most severe forms, intra-abdominal dissemination of the infection.1,2
It is unusual for PID to be the cause of acute intestinal obstruction. Most cases are related to the formation of adhesions in the context of the infectious process, although it has been described as due to the exclusive presence of the C. trachomatis bacteria.1–4 It is believed that the microorganisms involved in the pathogenesis of this sexually transmitted disease can spread directly from the fallopian tubes to the peritoneum, via the lymphatic or hematic route, or through diagnostic procedures.
Adhesion illness is well known and it is accepted that they usually appear 5–7 days after peritoneal damage and progressively organise as fibrous tissue. It is not uncommon for patients with PID to form adhesions responsible for chronic abdominal pain, but an acute complication like complete intestinal obstruction due to the development of early adhesions, as in our case, constitutes a rare finding.4
Generally, but not always, intestinal obstruction has been described in severe forms of PID with development of salpingitis or tubo-ovarian abscesses. Thus, obstructive complication should be suspected in any patient with PID, whether associated with salpingitis or tubo-ovarian abscesses or not, which begins with diffuse abdominal pain or vomiting, especially in women where there is no other known history that could justify it.2,4
The most specific ultrasound or radiological findings of PID include the presence of cervicitis, endometritis, salpingitis, oophoritis or tubo-ovarian abscesses. However, for the diagnosis of intestinal obstruction associated with PID, an exploratory laparotomy is usually necessary, and only in a minority of cases, such as the one described, are radiological findings sufficient to guide the diagnosis of obstruction.5 Urgent surgery also becomes the therapeutic modality of choice in complicated forms.
In conclusion, although infrequent, acute intestinal obstruction associated with PID should be considered in patients with abdominal pain and vomiting, especially when there is no other obvious cause. Early laparotomy is indicated in cases of complicated PID as a diagnostic and therapeutic modality.
Conflict of interestsAlicia Martín-Lagos Maldonado, Tania Gallart Aragón, Maria del Carmen Porcel Marin: None.
Please cite this article as: Martín-Lagos Maldonado A, Gallart Aragón T, Porcel Marin MC. Enfermedad inflamatoria pélvica: una causa inusual de obstrucción intestinal aguda. Gastroenterol Hepatol. 2019;42:549–550.
