



In recent decades, the prevalence of childhood obesity has increased, with the major implications for public health. However, the factors that contribute to obesity in children are still poorly understood. The present study aimed to investigate the role of parental reflective functioning (PRF) in childhood obesity.
MethodIn a cross-sectional design, 120 sets of parents of 60 children (n = 30 with obesity, age range 6–11) were recruited by local paediatricians. Parents completed the Parental Reflective Functioning Questionnaire. Children's and parents’ weight (assessed by BMI), as well as their socio-economic status (SES), were assessed to explore the contribution of PRF in the prediction of children's weight, controlling for parents’ weight and SES.
Resultst-test showed significant differences with medium effect sizes in BMI, SES and PRF between parents of children with and without obesity. The best model resulted from hierarchical multiple regression analyses and showed that mothers’ PRF predicted children's BMI above and beyond the prediction by parents’ BMI and SES.
ConclusionsLow maternal PRF could be an important target for intervention strategies, highlighting the need to consider parental responses to children's emotions in the treatment of childhood obesity, particularly in parents with low SES and high BMI.
En las últimas décadas la prevalencia de la obesidad infantil ha aumentad, teniendo implicaciones relevantes por la salud pública, pero hay todavía poca comprensión de los factores que contribuyen a la misma. La finalidad del estudio es investigar el papel de la función reflectiva parental (PRF) en la obesidad infantil.
MétodoEn un estudio transversal, 120 parejas de padres de 60 niños (30 con obesidad, con edades entre 6 y 11 años) fueron reclutados por pediatras locales. Los padres tuvieron que rellenar el Parental Reflective Functioning Questionnaire. El peso de los niños y de los padres (BMI), así como el estado socio-económico (SES) fueron evaluados para explorar la contribución del PRF a la predicción del peso de los niños, en relación al peso parental y al SES.
ResultadosEl t-test ha mostrado diferencias significativa entre padres de niños con y sin obesidad en BMI, SES y PRF. El mejor modelo resultado de los análisis de regresión múltiple jerárquica ha mostrado que el PRF materno puede predecir el BMI de los niños más que el BMI paterno y el SES.
ConclusionesUn PRF materno bajo podría representar una diana importante para estrategias de intervención.
Over the last 40 years, the prevalence of childhood obesity has increased globally, which has major implications for public health, as obesity predisposes individuals to many chronic diseases (Lin, Strong, Tsai, Lin, & Fung, 2018). Childhood obesity is the result of complex interactions among genetics and environmental and psychological factors (Ang, Wee, Pohm, & Ismail, 2013). Overall, although genetic factors play an important role in the transmission of overweight and obesity from parents to their children, Waterland (2008) highlighted how the rapid increase in the prevalence of obesity suggests the involvement of other mechanisms. For these reasons, there is a need to study potential environmental and psychological mechanisms involved in the onset of childhood obesity (Bergmann et al., 2016).
The family environment plays a crucial role in the development of childhood obesity, and familial patterns in weight status are well established. Among the stronger predictors of children's weight, numerous studies have demonstrated that maternal obesity is an important risk factor for the development of childhood obesity (Angoorani et al., 2018; Ejtahed et al., 2018). Between parents, several studies have reported that maternal weight is more strongly associated with children's weight than is paternal weight (Linabery et al., 2013). Another well-known risk factor for childhood obesity is socio-economic status (SES). In general, children from low socio-economic families in industrialized countries are at higher risk of being obese (Lissner et al., 2016). However, the results of a longitudinal survey examining the impact of family income on childhood weight status among children in the United States suggested that although family income was lower among children who were obese, it might act primarily as a proxy for other unobserved characteristics that determine the child's weight status; thus, SES may not have a direct role in causing obesity (Chia, 2013).
In studies on environmental determinants, a significant relationship between parenting and childhood obesity has been found, highlighting that parenting affects children's eating and weight (Gicevic et al., 2016). Given the importance of affective processes in eating behaviour, the issue of parents’ dysregulated emotional responses has recently received increasing support in studies on parents of children with obesity (e.g. Aparicio, Canals, Arija, De Henauw, & Michels, 2016; Mazzeschi et al., 2014). Although the idea has been previously introduced that children's obesity is connected to a mother's failure to provide a regular, persistent and appropriate response to the child's needs and to her tendency to react improperly by protecting and feeding him/her to excess (Bruch, 1941), little is still known about how responses to children's emotions are related to eating in the parenting context.
The few empirical studies focusing on the relationship between parenting, emotional regulation and childhood obesity, overall seem to suggest that parents’ inability to regulate negative emotions and distress is at the root of developing maladaptive emotional regulation strategies in the child, such as turning to food that becomes itself a regulator (Aparicio et al., 2016; Bost et al., 2014; Escandón-Nagel, Peró, Grau, Soriano, & Feixas, 2018; Fiese, Hammons, & Grigsby-Toussaint, 2012; Frankel et al., 2012; Hughes, Power, O’Connor, & Fisher, 2015).
The capacity for parental reflective functioning (PRF)—defined as parents’ capacity to comprehend the developing mind of their child, to reflect upon it and to keep the inner life of the child in mind—may shed some light on the understanding of how parents may shape the regulation of energy intake in children. PRF concerns the parents’ specific capacity to mentalize and reflect upon their actual and evolving relationship with their children. PRF is considered to be more specific to the parent-child relationship than is the parents’ general capacity to reflect on mental states. The parents’ capacity to keep in mind a representation of their child as having his/her own feelings, desires and intentions is postulated to lie at the root of sensitive caregiving by enhancing parents’ ability to imagine and try to understand the experience of their infant. PRF is intimately tied to the parents’ capacity to respond adaptively to children's needs, particularly in the moments involving heightened emotion, and is therefore supposed to be central to the formation of the child's specific mode of affect regulation (Fonagy, Gergely, Jurist, & Target, 2002; Grienenberger, Kelly, & Slade, 2005). A recent review on empirical studies investigating PRF give support to the notion that weaker parental mentalization is connected with weaker child emotion regulation capacity (Camoirano, 2017).
Recently, a new measure to assess parents’ capacity for mentalization has been validated. The Parental Reflective Functioning Questionnaire (PRFQ; Luyten, Mayes, Nijssens, & Fonagy, 2017) is a brief and multidimensional assessment tool with items that aim to capture three key aspects of PRF: (a) repudiation or defence against mentalization (Pre-Mentalizing modes), that concerns an inability to enter the subjective world of the child (e.g. “My child sometimes gets sick to keep me from doing what I want to do”); (b) the inability to recognize that mental states are not transparent (Certainty about Mental States), which deals with the lack of recognition of the impossibility to exactly know what is going on in the child's mind (e.g. “I always know why my child acts the way he or she does”); (c) interest in the child's thoughts and feelings and a genuine curiosity about the son's states of mind that underlie his/her behaviour (Interest and Curiosity in mental states) (e.g. “I am often curious to find out how my child feels”).
Studies that have assessed PRF using the PRFQ have shown that a parent's capacity to mentalize may be a critical factor in tolerating an infant's distress, enhancing more positive discipline strategies, and perceiving less parenting stress (Nijssens, Bleys, Casalin, Vliegen, & Luyten, 2018; Rostad & Whitaker, 2016; Rutherford, Maupin, Landi, Potenza, & Mayes, 2016; Rutherford et al., 2018). As the parental capacity to give meaning to children's behaviour shapes the parents’ affective and behavioural reactions to the child, these studies suggest that parents with higher parental mentalization experience less helplessness, are less emotionally reactive to children's behaviour and are more able to regulate children's arousal (Luyten et al., 2017).
Based on these findings, PRF could contribute to the empirical exploration of the mechanisms underlying children's risk of obesity in the parenting context. Few empirical research studies have addressed this issue. Lower levels of reflective functioning have been found in subjects with eating disorders and in their mothers (Rothschild, Levy-Shiff, Fridman-Balaban, Gur, & Stein, 2010; Tasca, 2019; Ward et al., 2001). One study has investigated the effect of mothers’ general reflective functioning capacity (not PRF) on children's weight, identifying an indirect effect mediated by the quality of the mother-child attachment relationship (Keitel-Korndörfer et al., 2016).
The aim of the present study was to investigate the role of both parents’ PRF in childhood obesity. We supposed that the lack of parents’ capacity to respond adaptively to children's needs, that is, low PRF, would be a factor that contributes to childhood obesity. Specifically, as previous research have shown that parents’ weight and familial SES are important risk factors for childhood obesity, we hypothesized that low PRF might be a factor that contributes to childhood obesity beyond parents’ BMI and familial SES. We investigated the relative role of fathers versus mothers, as, despite studies suggesting that the two parents have different relationships with their children, there is little evidence to date exploring differences between mothers and fathers in studies on childhood obesity (Davison et al., 2016).
MethodParticipants and procedureThe study was conducted in compliance with the ethical standards for research outlined in the Ethical Principles of Psychologists and Code of Conduct of the American Psychological Association (2010). Ethical approval was obtained from the Bio-Ethical Committee for Research at the University of Perugia.
Data were collected in two paediatric clinics of Perugia from November 2016 to October 2017. After the consent of paediatricians and with their help, flyers were distributed by researcher inviting the parents who met the inclusion criteria to participate in a study about how they feel and think about their children. No incentives were given, and it was emphasized that participation to the study was voluntary and that parents could withdraw in any moment. Confidentiality was ensured by the replacement of personal information with a numeric code and all data were stored at the University's offices; only the research team have access to the data.
Parents and their children were enrolled through convenience sampling. The inclusion criteria were: (a) both mothers and fathers agreed to participate; (b) parents having good knowledge and fluency of the Italian language and (c) paediatricians’ report of any youth developmental delay or mental retardation or secondary overweight due to endocrinological diseases.
Data were collected after both fathers and mothers signed informed consent forms to participate in the study. All the parents completed, at the same time, but separately, at the paediatricians’ offices a socio-demographic questionnaire and validated self-report measures; moreover, anthropometric measures were assessed in all participants. Children's measurements were assessed by the paediatrician, while parents’ measurements were self-reported.
One hundred and twenty children and their parents were invited in total, however attrition occurred among 16 families (13%) reportedly due to lack of time or interest.
Of the 104 families recruited, 14 were excluded from the study because did not fully complete the questionnaires. No one requested to withdraw from the study. Among the remaining 90 children, 30 were clinically obese (BMI z-score Mn = 1.82 SD = 0.82) and has been selected to composed the first group; the other 30 normal weight children (BMI z-score Mn = −0.21 SD = 0.63), has been selected matching with the first group by parents’ age to dial the second group. Therefore, the final sample was composed by 120 Caucasian parents (60 mothers and 60 fathers) and by their 60 children (50% males) between 6 and 11 years of age both included (Mn = 8.92, SD = 1.58). The average age of mothers was 42.96 (SD = 3.58) and the average age of fathers was 44.70 years (SD = 4.02). Families’ socio-economic status (SES), measured according to Hollingshead Four Factor Index of Socioeconomic Status (Mueller & Parcel, 1981), was mid-level (Mn = 41.39; SD = 7.12).
InstrumentsAnthropometric measuresChildren's height and body weight were assessed by paediatricians using standard techniques (Habicht, 1974) to calculate BMI and classifying children's BMI into categories according to the WHO classifications (2007) considering their gender and age.
Self-report measuresThe Hollingshead Four Factor Index of Socioeconomic Status (Mueller & Parcel, 1981). A measure of social status of individuals based on four domains: marital status, retired/employed status, level of education, and type of employment.
Emotional Overeating Questionnaire (EOQ; Masheb & Grilo, 2006). To control for whether there were differences between parents of children with and without obesity, parents’ emotional eating was assessed with the EOQ. It is a brief self-report instrument composed of six items assessing overeating in response to emotions; it is often used as a screening instrument to reveal maladaptive eating styles in adults. Parents responded to the item using a 7-point Likert scale ranging from 0 (never) to 6 (all days). The original questionnaire showed a high internal consistency with α = .85.
Parental Reflective Functioning Questionnaire (PRFQ; Luyten et al., 2017): Composed of 18 items divided into three subscales that assess PRF. A 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree) is used to score each item. The first, the Pre-Mentalizing (PM) subscale, is composed of items designed to capture non-mentalizing modes, higher scores indicate more nonmentalizing stance. The second, the Certainty about Mental States (CMS) subscale, is made up of items designed to reveal the inability to recognize that mental states are not transparent, higher scores indicate more difficulties to recognize that children's feelings, thoughts, and intentions are not always readily apparent. The third, the Interest and Curiosity (IC) subscale, assesses the interest and curiosity a parent has in their child's mental states, higher scores indicate more capacity to mentalize about their infants mental states. The internal consistency (Cronbach's alpha) for each subscale was .70, .82, and .75 respectively (Luyten et al., 2017). The Italian version showed good internal consistency in both mothers and fathers (Pazzagli, Delvecchio, Raspa, Mazzeschi, & Luyten, 2018).
Data analysisFirst, children's BMI scores were transformed into BMI z-scores using the program developed by the Centers for Disease Control and Prevention. The program specifies the measurement procedures, reference population, and age- and sex-specific cut-off points of an internationally accepted definition of child overweight and obesity. Second, descriptive statistics of the samples were calculated in terms of means and standard deviations or frequencies and percentages. Third, to assess the differences between child's BMI categories (normal weight vs. obese) concerning the measured variables, a number of independent sample t-test was performed. Child's BMI category (normal weight vs. obese) was inserted as an independent variable, whereas parents’ BMI, SES, EOQ scores and PRFQ scores were used as dependent variables. Effect size was measured using Cohen's d, in which benchmarks are small (d ≥ .2), medium (d ≥ .5), and large (d ≥ .8) (Cohen, 1988). Fourth, based on the aforementioned studies, as well as the significant differences shown by t-test(s), hierarchical multiple regression was performed to investigate the role of parents’ BMI, SES and PRF on child's BMI. Because t-test(s) showed no differences in parents’ EOQ scores between the two groups, parents’ EOQ scores were not inserted as a variable in the hierarchical multiple regression. Instead, even though mother's BMI was not significantly different between the two groups (p ≥ .05), it was inserted in regression model because previous studies indicated that it has a crucial role on child's weigth, even more important than father's BMI. Also, it was necessary to control its effect in the relation between child's BMI and the other variables (i.e., father's BMI, SES, PRFQ). Finally, although p-value related to mothers’ BMI was not significant, effect size was almost medium. Therefore, parents’ BMI and SES were inserted first, given that their association with child's BMI has been previously demonstrated. PRFQ variables were inserted last, because they were taken into account for the first time. Our interest was to determine whether these newly added variables showed a significant improvement in R2, namely in explaining variance of child's BMI. Five different models were run. Mother's BMI was the first variable entered (Model 1), followed by father's BMI (Model 2), then SES (Model 3), the significant subscales on mothers’ PRFQ assessments (Model 4) and the significant subscales on fathers’ PRFQ assessments (Model 5). With regard to child's BMI, in order to utilize a continuous dependent variable gender and age weighted, child's BMI z-score was used in regression analysis. It was inserted as the dependent variable. The Akaike information criterion (AIC) of the five models, as well as ANOVA among them, were calculated to find the best model (as indicated by significant variation in ΔR2 and the lowest AIC). The R package (R Development Core Team 2012) and PASW Statistics 18 (SPSS Inc., 2009) were used for the analyses.
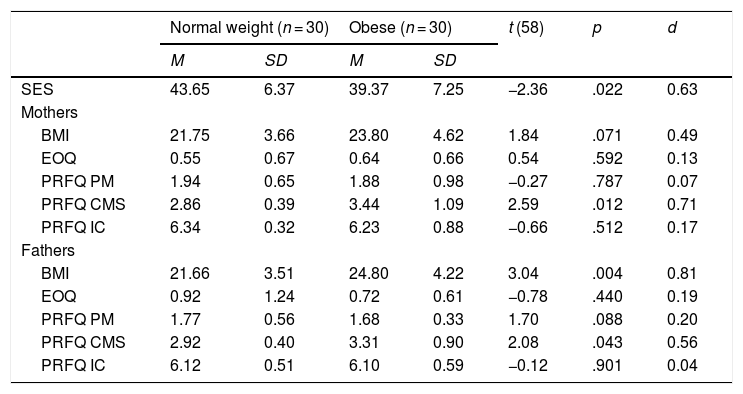
ResultsAs shown in Table 1, overall, significant differences with medium-large effect sizes were found between the two groups on parents’ BMI, familial SES and the CMS subscale of the PRFQ. No differences in EOQ scores or in the PM and IC subscales of the PRFQ were found.
t-test between groups of parents of children with and without obesity.
| Normal weight (n = 30) | Obese (n = 30) | t (58) | p | d | |||
|---|---|---|---|---|---|---|---|
| M | SD | M | SD | ||||
| SES | 43.65 | 6.37 | 39.37 | 7.25 | −2.36 | .022 | 0.63 |
| Mothers | |||||||
| BMI | 21.75 | 3.66 | 23.80 | 4.62 | 1.84 | .071 | 0.49 |
| EOQ | 0.55 | 0.67 | 0.64 | 0.66 | 0.54 | .592 | 0.13 |
| PRFQ PM | 1.94 | 0.65 | 1.88 | 0.98 | −0.27 | .787 | 0.07 |
| PRFQ CMS | 2.86 | 0.39 | 3.44 | 1.09 | 2.59 | .012 | 0.71 |
| PRFQ IC | 6.34 | 0.32 | 6.23 | 0.88 | −0.66 | .512 | 0.17 |
| Fathers | |||||||
| BMI | 21.66 | 3.51 | 24.80 | 4.22 | 3.04 | .004 | 0.81 |
| EOQ | 0.92 | 1.24 | 0.72 | 0.61 | −0.78 | .440 | 0.19 |
| PRFQ PM | 1.77 | 0.56 | 1.68 | 0.33 | 1.70 | .088 | 0.20 |
| PRFQ CMS | 2.92 | 0.40 | 3.31 | 0.90 | 2.08 | .043 | 0.56 |
| PRFQ IC | 6.12 | 0.51 | 6.10 | 0.59 | −0.12 | .901 | 0.04 |
Note. SES: Socio Economic Status; BMI: Body Mass Index; EOQ: Emotional Overeating; PRFQ PM: Pre Mentalizing; PRFQ CMS: Certainty about Mental States; PRFQ IC: Interest and Curiosity.
p <.05 significant difference. d: ≥ .2 small effect size; ≥ .5 medium effect size; ≥ .8 large effect size.
More specifically, the BMI of fathers and mothers of children with obesity was higher than that of parents of normal weight children. Although p-value referred to mothers’ BMI was not significant, effect size was almost medium. Familial SES and the CMS subscale of the PRFQ among parents of children with obesity were higher than those of parents of normal-weight children.
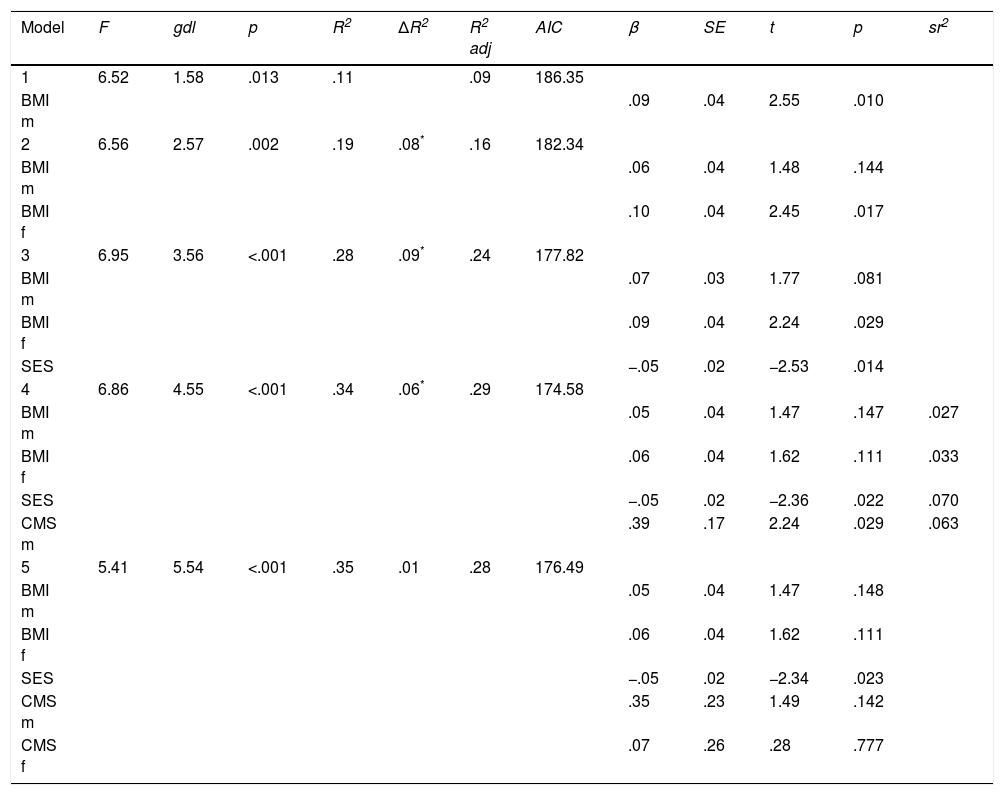
Table 2 shows the results of the five hierarchical models. Hierarchical multiple regression suggested that Model 4 was the best model because it showed a lower AIC than did other models (namely, the best trade-off between the goodness of fit of the model and the simplicity of the model), as well as a significant variation in R2(ΔR2) from Model 3 (namely, a significant increase in the variance of children's BMI explained by Model 4). Model 4 was significant (F(4,55) = 6.86, p < .001) and explained over 34% of the variance (R2 = .345) in children's BMI z-score. Although mothers’ BMI was a significant predictor of children's weight in Model 1, fathers’ BMI was a stronger predictor in Model 2. The higher the parents’ BMI, the higher the children's BMI z-score. Model 3 confirmed the relationship between BMI and SES. The higher the SES is, the lower the child's BMI z-score. In Model 4, mothers’ PRF became a significant predictor of children's weight, above and beyond the role of parents’ BMI and SES. Children's weight increased approximately .3 z-score for each unit increase in mothers' CMS. SES predicted a decrease of -.05 z-score in children's weight. Model 5, which included fathers’ PRF, did not add a significant increase in explained variance in children's BMI z-scores.
Hierarchical multiple regression-model summary, AICs and ANOVA results of five models, coefficients.
| Model | F | gdl | p | R2 | ΔR2 | R2 adj | AIC | β | SE | t | p | sr2 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 6.52 | 1.58 | .013 | .11 | .09 | 186.35 | ||||||
| BMI m | .09 | .04 | 2.55 | .010 | ||||||||
| 2 | 6.56 | 2.57 | .002 | .19 | .08* | .16 | 182.34 | |||||
| BMI m | .06 | .04 | 1.48 | .144 | ||||||||
| BMI f | .10 | .04 | 2.45 | .017 | ||||||||
| 3 | 6.95 | 3.56 | <.001 | .28 | .09* | .24 | 177.82 | |||||
| BMI m | .07 | .03 | 1.77 | .081 | ||||||||
| BMI f | .09 | .04 | 2.24 | .029 | ||||||||
| SES | −.05 | .02 | −2.53 | .014 | ||||||||
| 4 | 6.86 | 4.55 | <.001 | .34 | .06* | .29 | 174.58 | |||||
| BMI m | .05 | .04 | 1.47 | .147 | .027 | |||||||
| BMI f | .06 | .04 | 1.62 | .111 | .033 | |||||||
| SES | −.05 | .02 | −2.36 | .022 | .070 | |||||||
| CMS m | .39 | .17 | 2.24 | .029 | .063 | |||||||
| 5 | 5.41 | 5.54 | <.001 | .35 | .01 | .28 | 176.49 | |||||
| BMI m | .05 | .04 | 1.47 | .148 | ||||||||
| BMI f | .06 | .04 | 1.62 | .111 | ||||||||
| SES | −.05 | .02 | −2.34 | .023 | ||||||||
| CMS m | .35 | .23 | 1.49 | .142 | ||||||||
| CMS f | .07 | .26 | .28 | .777 |
Note. Predictors: BMI m: Mother's Body Mass Index; BMI f: Father's Body Mass Index; SES: Socio Economic Status; CMS m: Mother's Certainty about Mental States; CMS f: Father's Certainty about Mental States. Dependent variable: Child's Body Mass Index z-score.
The present research aimed to explore whether childhood obesity was influenced in part by low PRF. A comparison of mothers and fathers of children with and without obesity showed that parents of children with obesity had higher BMI, lower SES and lower PRF than those of normal-weight children. Moreover, among the different hierarchical models run, the model that included parents’ weight and SES and mothers’ PRF was the best, as it was significant and explained over 34% of the variation in children's weight.
With regard to parents’ weight, these data confirm those of previous studies showing that higher parents’ weight predicted higher children's weight (Ejtahed et al., 2018; Linabery et al., 2013). In contrast to earlier research, paternal weight was a stronger predictor of children's weight than was maternal weight. It must be taken into account that few studies consider the key role played by both parents, as attention has been primarily given to maternal factors, and fathers are unequivocally underrepresented in studies on parenting and childhood obesity (Davison et al., 2016). Therefore, future studies should further explore the role of both parents’ weight as risk factors in childhood obesity. However, in our research, the significant difference in parents’ weight could not be caused by their emotional eating, as no difference emerged between the parents of the two groups.
With regard to familial SES, our results confirmed those of previous studies showing that children from low socio-economic families in industrialized countries are at higher risk of being obese (Lissner et al., 2016). In general, while children from all SES groups are considered vulnerable to the development of obesity, children whose parents have low SES appear to have a higher than average risk.
Referring PRF, parents’ CMS subscale scores were higher in the children with obesity group than that of normal-weight group. No differences in the PM and IC subscales of the PRFQ were found. Furthermore, mothers’ CMS was significantly related to children's BMI, above and beyond parents’ BMI and SES.
The CMS subscale assesses parents’ inability to recognize that children's mental states are not transparent, and it has been shown in parental accounts of their children's behaviours and attitudes that go far beyond the data; these accounts are characterized by undue certainty about the mental states of the child and are often distorted, intrusive and sometimes paranoid (Luyten et al., 2017).
Therefore, a greater maternal inability to recognize the opaqueness of children's mental states predicted greater children's weight. It seemed that mothers’ inability to understand that they have a limited ability to truly know what is in their children's minds and to tolerate the uncertainty of not knowing why their children are behaving in a certain way, which involves mothers’ awareness that their children's mental state is separate from her (Ordway, Sadler, Dixon, & Slade, 2014), constitutes a risk factor in the onset of childhood obesity.
The absence of a relationship between the interest and curiosity, and non-mentalizing subscales is also of interest suggesting that these modes of parental mentalization may be differentially related to, or independent from, the risk of onset of obesity in childhood. It may be that these dimensions of mentalization are less relevant to the specific characteristics of parenting in childhood obesity than the dimension of certainty about mental states. Parents of children with and without obesity seem not to differ both in their capacity to keep their child in mind (Interest and curiosity), and in difficulties to identify and understand their children mental states (Pre-mentalizing modes). A previous study found out that pre-mentalizing was associated with low levels of maternal emotional availability, except to maternal intrusiveness, while high level of certainty seemed to be associated with intrusiveness, as the parent assumed to know everything about their child's mental states (Luyten et al., 2017); hence, in the present study the specific combination of PRFQ subscales seemed to suggest that mothers of children with obesity show not general difficulties in emotional availability, but greater intrusiveness and difficulties in understanding that they have a limited ability to truly know what there is in their child's mind. Interestingly, this finding seems to be also consistent with clinical observations of the attitudes of mothers of children with obesity to be overprotective and to superimpose their own needs on those of their child, leading to a mismatch in the interaction between the dyad and difficulties in children's ability to learn to distinguish hunger from other internal or affective states (Bruch, 1941).
As the CMS subscale measures the extent to which the parent is unable to recognize that children's feelings, thoughts, and intentions are not always readily apparent, high certainty could consequently affect mothers’ capacity to mirror children's mental states and, therefore, to regulate his/her affects (Luyten et al., 2017). Because parents impact children's ability to learn to self-regulate and develop strategies for managing increasing levels of arousal, such as negative affects and stress responses, and because PRF is considered to serve as a modulating function once the parent-child relationship has been dysregulated, acting as a buffer against breakdowns in affect regulation during times of stress (Grienenberger et al., 2005), our results seemed to substantiate the issue of mothers’ dysregulated emotional response in childhood obesity. Future studies should investigate the supposed mediation role played by mothers’ emotion regulation strategies in the relationship between high maternal certainty and high child weight.
To date, only one study has investigated the potential role played by maternal reflective function in childhood obesity. In contrast to the hypotheses based on the literature, Keitel-Korndörfer et al. (2016) found that the general reflective functioning of 60 mothers with and without obese children aged 18 to 55 months was not directly associated with the child's weight; rather, general reflective functioning indirectly affected the child's BMI percentile via the level of security in the mother-child relationship. The research differed from our exploratory study in several respects. First, the sample selection criteria were mothers’ weight and not children's weight. Second, the sample was composed of pre-schoolers, in contrast to our sample composed of children in early middle childhood, a developmental period in which regulation issues are salient in both emotional and eating domains (Harrist, Hubbs-Tait, Topham, Shriver, & Page, 2013). Finally, maternal general capacity, rather than her PRF, was assessed to reflect on mental states. More recently, studies have paid greater attention to reflective functioning as being relationship-specific, suggesting that the capacity to reflect on a specific relationship with a significant other could differ from more general reflective processes (Sharp & Fonagy, 2008).
Overall, our findings showed that the combination of high maternal CMS, high parental BMI and low familial SES represents a risk factor for childhood obesity. It seemed that to grow up in a socio-economically disadvantaged environment in an industrialized country, with parents overly focused on eating and with mothers being too certain of what was in their children's minds, constituted an environment where children have a higher risk of becoming obese. Future research on childhood obesity is needed to better comprehend these issues.
With regard to the dissimilarities between mothers and fathers that emerged in our study, children's weight was affected mainly by maternal PRF and paternal weight. Differences in PRF capabilities related to parental gender have already arisen in a previous study (Pajulo et al., 2018; Pazzagli et al., 2018) and may be the manifestation of a difference between mothers and fathers with respect to how they engage in reflective interactions with their children (Arnott & Meins, 2007). This finding is also consistent with that of a previous study on youngsters with obesity that showed more maternal than paternal influence on children's emotion regulation (Vandewalle, Moens, & Braet, 2014). It seemed that in this socio-economically disadvantaged environment, mothers’ lack of capacity to give meaning to children's behaviour and to regulate negative emotions and distress had a strong influence on children's weight. In contrast, fathers played a more crucial role than mothers in constructing their children's health behaviours, as their weight was a stronger predictor of children's weight.
The study is exploratory in nature, and the findings need to be replicated before firm conclusions can be drawn. Future research should confirm the observed effects of PRF on childhood obesity and the supposedly mediating role of maternal emotion regulation strategies on the relationship between PRF and children's weight with a larger sample. The current study had other limitations, including the fact that only self-report measures were used. The use of observational methods would be more desirable, and these approaches should be integrated into future studies. As the study is cross-sectional in nature, it does not allow inferring causal relationship. It would be fruitful for future research to utilize longitudinal data to more definitely predict associations between the selected variables. Furthermore, the study aimed to focus on the role of PRF beyond parents’ weight and familial SES, but many other factors of the family environment might influence children’ obesity. More clarification is needed regarding the risk factors associated with childhood obesity and the relationships among different predictors of children's weight. To our knowledge, this is the first study aiming to explore the contribution of PRF to the prediction of children's weight above and beyond the contribution of mothers’ and fathers’ weight and SES. The results suggested that low maternal PRF could be an important contributing factor to children's weight, thus highlighting the need to take into account parental responses to children's emotions in the assessment and treatment of childhood obesity. As a deeper understanding of the multi-factorial contributors to obesity is of utmost importance to aid in the development of effective interventions aimed at reducing the rates of global obesity, the current study provides preliminary support for the perspective that childhood obesity prevention and treatment programmes expand beyond a focus on children's behavioural regulation, and also encompass the role of PRF in childhood obesity. As noted by Harrist et al. (2013), interventions that target emotion regulation strategies could be a useful new approach and would have the potential to impact eating behaviours and prevent weight issues among children.
