




Background/Objective: Emotional intelligence is a variable which has been the subject of significantly increased research in recent years. Relationships have been shown with both physical and psychological problems. The aim of this study is to analyse the direct and indirect effect that emotional intelligence exerts over the manifestation of physical and psychological clinical symptomatology and to severe disorders such as burnout syndrome in a professional group in which social function is fundamental. Method: So that, 881 Latin-American catholic priests (Mage=45.89; SDage=11.58) were evaluated using the Trait Meta-Mood Scale-24, the Maslach Burnout Inventory-22 and the General Health Questionnaire-28. Results: Using path analysis, emotional intelligence, especially Attention and Emotional Clarity, shows a high effect on psychological and somatic issues. Conclusions: Thus, both specific disorders and general well-being are related to emotional intelligence. Providing effective emotional intelligence training sessions seems to be able to reduce possible physical and emotional disorders.
Antecedentes/Objetivo: La inteligencia emocional es una variable que ha sido objeto de un incremento notable de investigación a lo largo de los últimos años. La inteligencia emocional ha mostrado numerosas relaciones con múltiples variables psicológicas, destacando su conexión con diversos trastornos físicos y psicológicos. El objetivo del presente estudio es analizar los efectos directos e indirectos que la inteligencia emocional ejerce sobre la manifestación de sintomatología somática y psicológica, así como sobre el desarrollo de trastornos como el síndrome de burnout en un grupo de profesionales cuya labor social resulta esencial. Método: Se aplicaron las escalas Trait Meta-Mood Scale-24, Maslach Burnout Inventory-22 y General Health Questionnaire-28 a un total de 881 sacerdotes católicos latinoamericanos (Medad=45,89; DTedad=11,58). Resultados: Mediante path analysis se muestra el efecto que la inteligencia emocional, especialmente la atención y claridad emocional, ejerce sobre las alteraciones somáticas y psicológicas. Conclusiones: Tanto los trastornos específicos como el bienestar general presentan una relación clara con la inteligencia emocional. Proporcionar programas formativos efectivos que desarrollen la inteligencia emocional podría reducir la aparición de trastornos físicos y emocionales.
Emotional intelligence (EI) appeared in the scientific literature for the first time more than twenty years ago, defined as “…the ability to monitor one's own and others’ feelings and emotions, to discriminate among them and to use this information to guide one's thinking and actions” (Salovey & Mayer, 1990, p. 189). Nonetheless, it was not until years later that this concept was globally accepted, and was understood to be an important aspect in achieving personal and professional success (Goleman, 2007). Since then, both the development of different explanatory models and the research into EI have grown exponentially (Joseph & Newman, 2010). Emotional capabilities are fundamental factors in social interaction (Peña-Fernández, Andreu-Rodríguez, Barriga, & Gibbs, 2013). They are the basis of social and communicative functions and they also allow people to adapt to their development contexts (Mavroveli, Petrides, Rieffe, & Bakker, 2007).
There are professional groups in which interaction and social function are particularly relevant, such as priests. The ability of this group to understand and deal with personal emotions and, more fundamentally, those of their parishioners, is of paramount importance in the correct development of their social role (Meaghera, 2015). There is evidence that EI is significantly related to specific pro-social attitudes (Jiménez & López-Zafra, 2011), which are fundamental to the work of priests. Nonetheless, while it is true that the emotional relationships that priests establish with their parishioners are important to their work, they must also be able to understand and manage their own emotions appropriately.
Diocesan priests are exposed to difficult situations in areas such as doubts, inner conflicts, tiredness, anxiety… Sociocultural changes experienced by the Church and its priests along the last decades reflect the need to analyze these problems and possible solutions in order to promote a ministry that encourages and motivates its mission. In this regard, multiple stressors affect priests every day, such as a lack of social support, overwork, misaligned of interpersonal goals or problems of self-esteem among others (Miller-Clarkson, 2013), which increase the difficulties they have to face (e.g. Hansson, 2006; Rossetti & Rhoades, 2013). As a result of all these stressors, crises on priestly life can appears. Those crises evidence a breach of internal balance already acquired. An inappropriate lifestyle which requires a reorientation of basic schemes of life is the main reason to suffer a crisis. Even though priest can experience a broad variety of crisis, affective-sexual crisis, problems in relations with authority, triggered by labor problems, difficulties in interpersonal relationships or career and faith crisis are the most common (Miranda, 2002). Evidence about the influence of those variables on subjective well-being, mental health and engagement has been demonstrated along different contexts (e.g. Rodríguez-Fernández et al., 2016).
Although cultural heritage is one of the main reasons for vulnerability in young priests, especially along Western cultures. However, there are other relevant factors such as reduced and difficult labor insertion; lack of social recognition related to their role; isolation on their daily life; a poor inner life; too many commitments; lack of sleep; reduced leisure; and unsuitable housing (Laghi, 1992). All these factors increase the priest vulnerability to emotional and moral exhaustion, and, in general, the negative effects of stress.
Added to this, burnout syndrome is a possible consequence of experiencing these multiple stressors (Jackson-Jordan, 2013; Ventura, Salanova, & Llorens, 2015). This syndrome is characterized by physical and emotional exhaustion - provoked by constant interaction with other people; low self-esteem or reduced personal accomplishment -owing to personal or professional unsuitability to the job- and depersonalisation -a cynical, pessimistic, negative and sometimes aggressive attitude towards others (Maslach & Jackson, 1984). High levels of incidence of this syndrome have been observed in priests, meaning up to 25.39% (López Herrera et al., 2014).
Along with all the factors previously exposed, insufficient spirituality is a significant factor, both for reason related with priest's social work and because of its relationship with well-being and life satisfaction (Anand, Jones, & Gill, 2015). In this regard, intrinsic religiousness, spiritual maturity, and self-transcendence are significant predictors of better physical and emotional well-being, mental health, and positive functioning (e.g. Jim et al., 2015; Sanders et al., 2015), both along people suffering different diseases and normal population, of whom priest are part of the community.
Exhausted priests often show a poor spiritual life. The nature of their vocational orientation motivates, in many cases, feelings of high personal accomplishment, because their services as pastors and leadership in the communities where they work. However, also high scores in spirituality correlated with high scores on emotional exhaustion and depersonalization. This suggests that emotionally exhausted priests may be resorting to spirituality to face wear (Doolittle, 2007). When the activity of the priest is excessive, the balance between inner life and activity breaks, and stress occurs. Additionally, in recent decades, the spiritual identity of the priest has been affected by cultural changes. This has contributed to a perception of priestly devaluation that as a result, leads to a lack of personal fulfilment in their life and nonsense in their mission.
Factors such as the aforementioned increase the possibility to experience burnout syndrome, characterized specially by a life without meaning and emotional exhaustion leading, sometimes, to a desire to leave the priesthood. Burnout syndrome, in turn, is related to significant somatic and psychological problems such as anxiety or depressive disorders, among others (De la Fuente et al., 2015; Reizer, 2015; Toppinen-Tanner, Ahola, Koskinen, & Väänänen, 2009). In the specific case of priests, positive correlations have been found between exhaustion and depersonalisation with respect to problems of anxiety and insomnia, and negative correlations between personal realization and depressive symptomatology and social dysfunction (López Herrera et al., 2014).
The potential utility of EI in terms of predictive validity has been recently demonstrated in various fields, especially in clinical areas related to variables such as social adjustment, anxiety and depressive symptomatology or perceived health, among others (e.g. Cheung, Cheung, & Huec, 2015; Zysberg, 2014). These relationships are, specifically, about the capacity of EI when it comes to reducing symptomatology and the risk of suffering different physical or psychological disorders (Schutte & Malouff, 2011) and improves coping strategies for stress (Velasco, Fernández, Páez, & Campos, 2006). Especially relevant to this work, it seems to reduce the risk of burnout (Görgens-Ekermans & Brand, 2012; Guy & Lee, 2015) and improve physical and psychological health functioning (Tsaousis & Nikolaou, 2005).
So, bearing in mind the above, and with the aim of improving the wellbeing of a professional group that has very particular characteristics, the aim of this research is to analyze the relationship between EI and health (i.e. physical and psychological wellbeing) and a specific disorders as burnout is. Specifically, this work aims to evaluate the capacity that EI has demonstrated to prevent somatic and psychological issues on other professional groups completely different work settings such as teachers or nurses, among others (Ju, Lan, Li, & Feng, 2015; Zhu, Liu, Guo, Zhao, & Lou, 2015). In this paper a path analyses is proposed to show a detailed analysis of both direct and indirect effects of the dimensions which comprised EI, defining the burnout syndrome as a mediating variable of general health issues.
In this way, EI may be understood to be a tool to help face stressful situations and reduce the effects both of specific disorders such us burnout syndrome and general health problems for, in this case, Latin-American catholic priests. The justification for this approach is based on the fact that mental health refers to a person's capability to adjust to the world, an adjustment which must be made on three levels: individual, which is linked to the capacity to understand and control one's own emotions; with respect to others, referring to the capacity to give and receive affection; and the capacity to adapt to stress, so avoiding negative health consequences (Diener, Eunkook, Richard, & Smith, 1999; Lazarus, 1991; Schönfeld, Brailovskaia, Bieda, Chi Zhang, & Margraf, 2016).
Based on the previous literature exposed along the introduction, an effect of EI over well-being is expected, whereas personal accomplishment and physical and emotional exhaustion are expected to defined as key factors in the understanding of this relationship. This study contributes to describe the relationship between EI and psychological and somatic health. Moreover, new evidence from a professional group which, having an important social role, has been little studied up to now is provided. In order to get this goal, a large number of participants from this sphere were used.
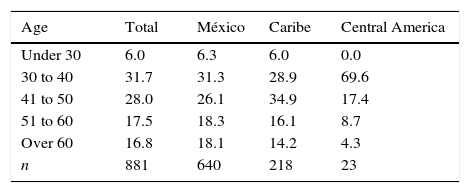
MethodParticipantsA cross-sectional study was carried out on a convenience sample of diocesans and catholic priests. Inclusion criteria were: have attended to previous courses of Human Maturity and Mental Health, and to pertain to catholic or diocesan order. On the other hand, a score indicating severe depression in the GHQ-28 was established as exclusion criterion. In this case, any of the participants was excluded from the sample based on this criterion. The sample was made up of priests from ten Mexican dioceses (n=640), five Costa Rican dioceses (n=173), one Puerto Rican diocese (n=45) as well as a group from Central American countries (i.e. Guatemala, n=4; El Salvador, n=2; Honduras, n=8; Nicaragua, n=6; and Panama n=3). Initially, the instruments were sent to a total of 912 participants, of whom 881 catholic priests participated voluntarily, representing 77.6% of the total population of priests in the geographical region formed by Mexico, Central America and the Caribbean. The mean age of the participants was 45.89 (SD=11.58). The distribution of ages, grouped into five categories based on country, is illustrated in Table 1.
InstrumentsThe Maslach Burnout Inventory (MBI-22; Maslach & Jackson, 1981), in its Spanish adaptation (Moreno, Oliver, & Aragoneses, 1991), was used to evaluate the three dimensions of burnout syndrome. Previous research has shown evidence of validity in relation to internal structure on this population, confirming the three-dimension structure of MBI-22 (López Herrera et al., 2014). Reliability of the MBI-22 was estimated for this sample using Cronbach's α coefficient for ordinal data (Elosua & Zumbo, 2008). The coefficients obtained were .85 for the Physical and emotional exhaustion dimension; .54 for Depersonalisation; and .81 for the Reduced sense of accomplishment dimension.
The General Health Questionnaire (GHQ-28; Goldberg & Williams, 1996) was administered, which, when used as a screening test, can detect early symptoms of psychological disorders in individuals who are not suffering from psychotic disorders. The questionnaire evaluates four dimensions: somatic symptoms, anxiety and insomnia, social dysfunction, and severe depression. The validity of the GHQ-28 has been studied in a range of contexts, from the general population to patients with acute clinical pathology, demonstrating adequate sensitivity (75-78%) and specificity (78-82%) in the general population (Retolaza Balsategui et al., 1993). In this sample, the instrument shows acceptable reliability, measured using Cronbach's α coefficient for ordinal data: .83 in the somatic symptom dimension; .86 for the anxiety and insomnia subscale; .90 in the social dysfunction factor; and .80 for the depression dimension.
Lastly, EI was measured using the Spanish adaptation of the Trait Meta-Mood Scale (TMMS-24; Fernández-Berrocal, Extremera, & Ramos, 2004). The scale comprises three dimensions: Attention, Clarity and Emotional Repair. The instrument has shown adequate convergent and discriminant validity (Fernández-Berrocal et al., 2004). The internal consistency of each sub-scale in this sample, estimated via Cronbach's α coefficient for ordinal data, is .90 for Attention, .91 for Clarity and .88 for Repair. It is important to note that high scores of emotional attention implies an overthink and is commonly associated with negative outcomes.
ProcedureTo gather the information, a set of stapled tests was sent to each diocese. Next to each booklet, a presentation letter with specific explanations about how to proceed to fill-up the instruments, and to do it in a lonely place without any kind of external guidance was given aimed at avoiding possible application bias. Following this instructions, each priest self-administered the test. The Ethics Committee of the hosting University granted ethical approval. The principles for conducting research contained in the Declaration of Helsinki were respected. Permissions and informed consents were collected by participating organizations. Removing names and using identifying codes that were not known by the researchers guaranteed confidentiality and anonymity.
Data analysisCanonical Correspondence Analysis (CCA; terBraak, 1986) was used to analyze the relationship between burnout syndrome and health and emotional intelligence, respectively. Using the CCA it is possible to analyze the relationship between items, which are represented graphically as vectors. The closer together the vectors are, the stronger the relationship between the evaluated items. It allows to look at both the covariation between items from different dimensions and also to see whether they are grouped in a way which agrees with the dimension they belong to in theory. Furthermore, the eigenvalue of each axis indicates the multivariate correlation of the items used in the analysis. One-way ANOVA was carried out to check differences on EI based on the region assessed (CI=95%). The effect of EI on burnout syndrome and health was analyzed using path analysis methodology. A series of goodness-of-fit statistics were used to analyze the proposed model: the ratio chi-square by degrees of freedom (χ2/df), the comparative fit index (CFI), and the root mean square error of approximation (RMSEA). Moreover two model evaluation criteria were employed to test the alternative model: the Akaike Information Criterion (AIC), and delta AIC (Δi). The AIC reflects the extent to which parameter estimates from the original sample will cross-validate in future samples (Bandalos, 1993), where the model with the smallest AIC value exhibits the greatest potential for replication. Moreover, delta AIC is a measure of each model relative to the best model. As a rule of thumb, a Δi< 2 suggests substantial evidence for the model; values between 3 and 7 indicate that the model has considerably less support; whereas a Δi> 10 indicates that the model is very unlikely (Burnham & Anderson, 2002). The maximum error of estimate at CI=95% is ±0.38. The data was analyzed using MPLUS 7 and CANOCO software.
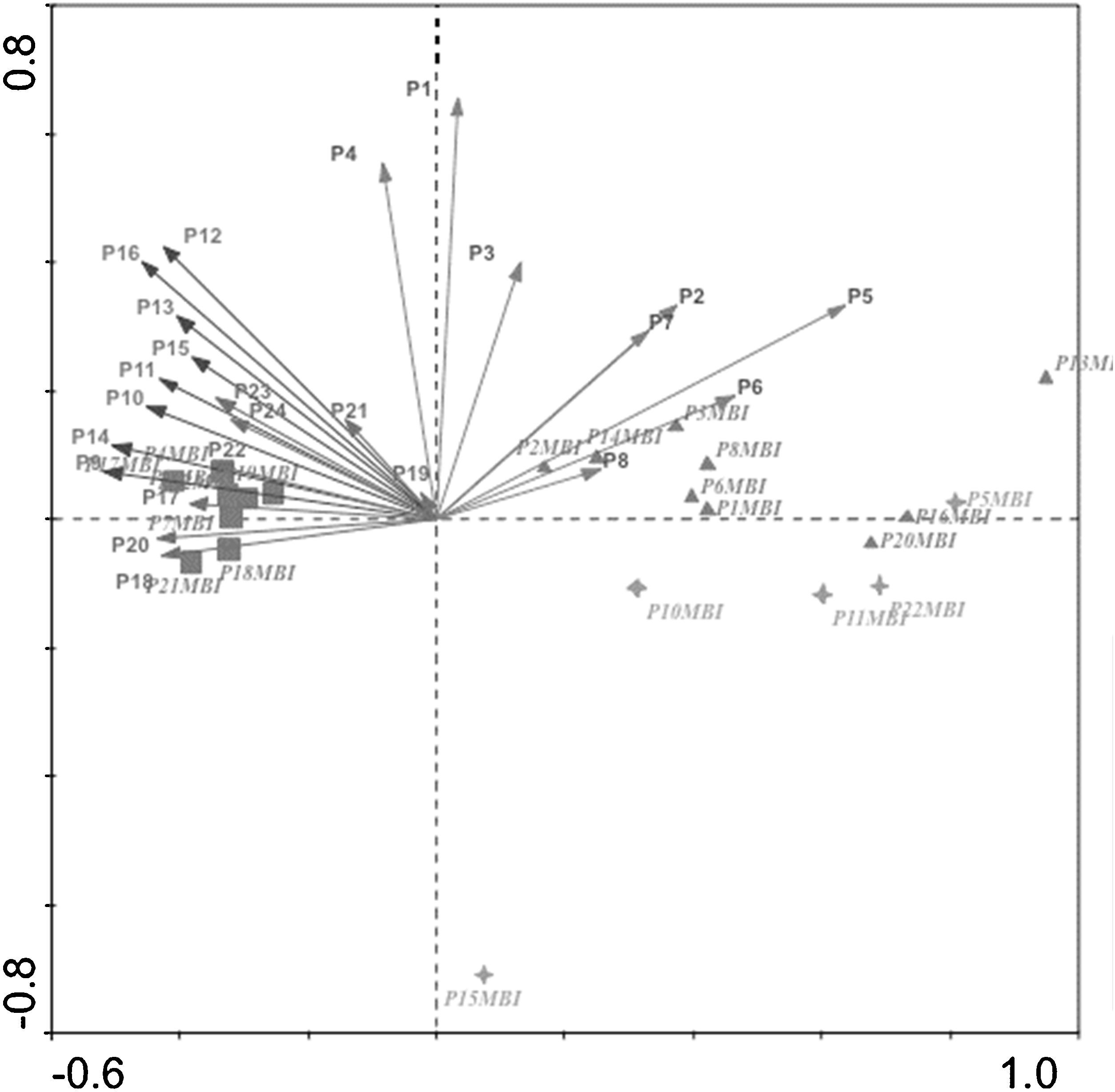
ResultsMultivariant characterization of the relationships between emotional intelligence and the level of burnoutThe relationship between EI and burnout syndrome proposed in the introduction was analyzed via CCA, combining the items from both instruments (Figure 1). Taking into account only the MBI-22, the results indicate a close association between the items of exhaustion and depersonalization dimensions. Furthermore, when analyzing the items of both instruments together, MBI-22 and TMMS-24, an increased relationship can be observed between the emotional repair and personal accomplishment dimensions on the one hand, and between emotional clarity and personal accomplishment on the other. As a counterpoint, practically no relationship was observed between depersonalisation and clarity and emotional repair, in opposite quadrants. The same pattern is repeated when the relationship between physical and emotional exhaustion and the dimensions of emotional clarity and repair are analyzed.
; P9-P16: Emotional clarity; P17-P24 (TMMS-24): Emotional repair (TMMS-24); P5MBI, P10MBI, P11MBI, P15MBI, P22MBI (Depersonalization MBI-22); P1MBI, P2MBI, P6MBI, P8MBI, P13MBI. P14MBI, P16MBI, P20MBI (Physical and Emotional exhaustion); P3MBI, P4MBI, P7MBI, P9MBI, P12MBI. P17MBI, P18MBI, P19MBI, P21MBI (Personal accomplishment).")
Canonical Correspondence Analysis between the items of the MBI-22 and the TMMS-24.
Note. P1-P8: Emotional attention (TMMS-24); P9-P16: Emotional clarity; P17-P24 (TMMS-24): Emotional repair (TMMS-24); P5MBI, P10MBI, P11MBI, P15MBI, P22MBI (Depersonalization MBI-22); P1MBI, P2MBI, P6MBI, P8MBI, P13MBI. P14MBI, P16MBI, P20MBI (Physical and Emotional exhaustion); P3MBI, P4MBI, P7MBI, P9MBI, P12MBI. P17MBI, P18MBI, P19MBI, P21MBI (Personal accomplishment).
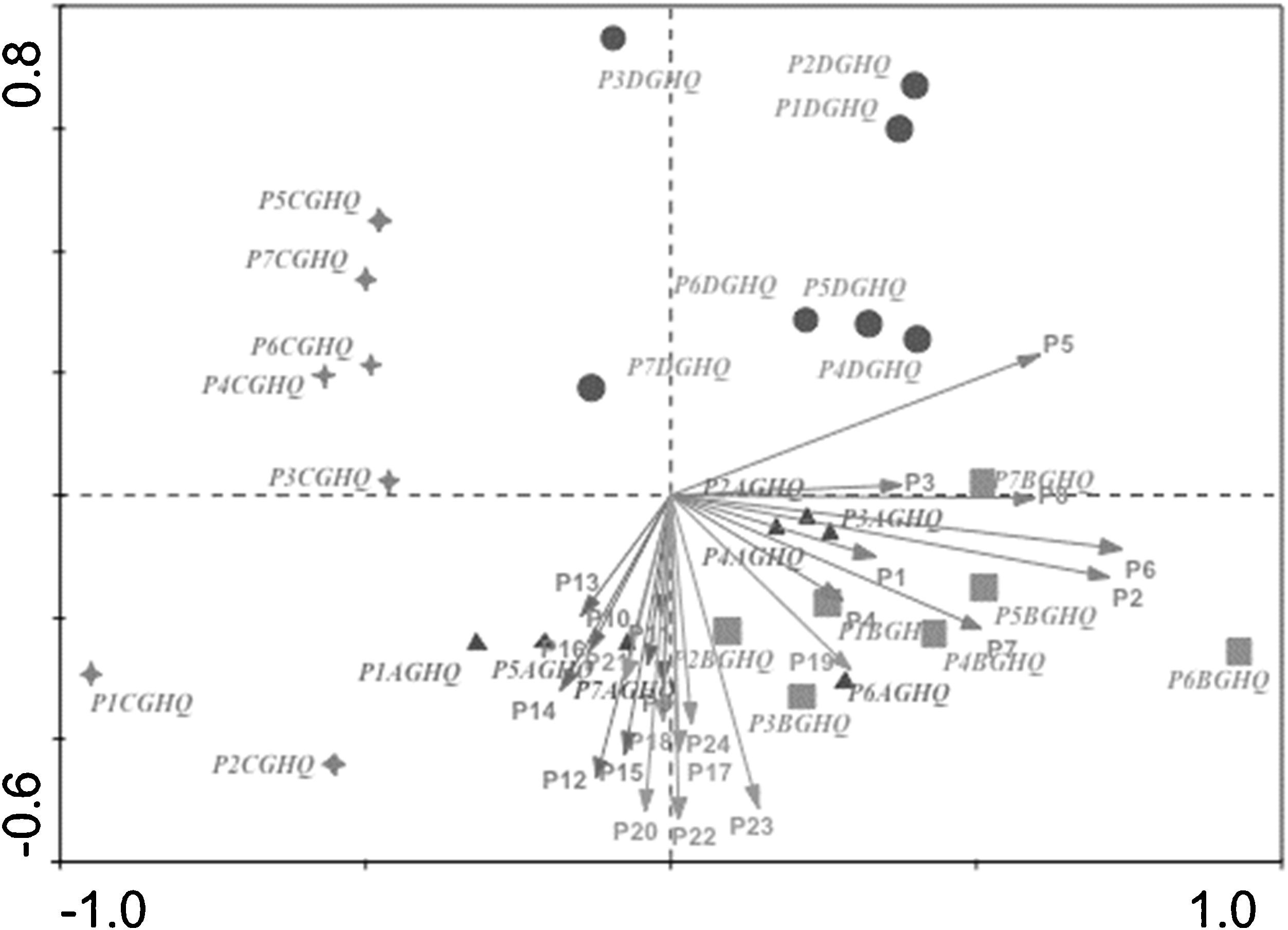
Just as with burnout, the relationship between EI and emotional and physical wellbeing was mentioned at the introduction of the study. With the aim of confirming this relationship, the CCA between the items of the TMMS-24 and the somatic and psychological symptoms under evaluation was performed (Figure 2). A generally negative relationship is seen between the clarity and emotional repair dimensions (left side of Figure 2) when it comes to somatic symptomatology showed on the right side of Figure 2. This pattern is reversed in the case of emotional attention, which stands out as having strong relationships, except in the case of social dysfunction.
; P9-P16: Emotional clarity; P17-P24 (TMMS-24): Emotional repair (TMMS-24); P1AGHQ-P7AGHQ (somatic symptom); P1BGHQ-P7BGHQ (anxiety and insomnia); P1CGHQ-P7CGHQ (social dysfunction); P1DGHQ-P7DGHQ (depression).")
Canonical Correspondence Analysis between items of the GHQ-28 and the TMMS-24.
Note. P1-P8: Emotional attention (TMMS-24); P9-P16: Emotional clarity; P17-P24 (TMMS-24): Emotional repair (TMMS-24); P1AGHQ-P7AGHQ (somatic symptom); P1BGHQ-P7BGHQ (anxiety and insomnia); P1CGHQ-P7CGHQ (social dysfunction); P1DGHQ-P7DGHQ (depression).
Firstly, no statistically significant differences were found on emotional intelligence based on the different regions assessed (p=.07). Once the relationship between EI and burnout and health of the priests was verified, and starting from the confirmed relationship between the syndrome and physical and emotional wellbeing (López Herrera et al., 2014), a path analysis was performed to evaluate both the relationships and especially, the effects between the variables. Bearing in mind the variables in the set, EI is understood to be an important variable when trying to reduce the risk of suffering diverse health problems which may affect a person, such as burnout syndrome. In addition, it can be seen how the continuation of these problems over time, linked to other contextual characteristics, can result in severe problems both psychical and psychological.
Firstly the independence model (Model0) was created which included representations of all of the relationships between the ten dimensions, evaluated using the three applied instruments. From this model any relationships with non-statistically significant standardized regression weights (p<.001) were eliminated, giving an alternative model (Model1) in which the covariance (i.e. correlations of the errors of measurement) between the dimensions of depersonalization and emotional and physical exhaustion is shown. In order to compare those models, the goodness of fit indices were analyzed (Table 2). The result of comparing both models (Table 2) shows the best indices of fit for Model1. In addition, the findings demonstrated a high probability of cross-validation because the fit statistics of the hypothesized model were substantially smaller than those of the independence model and it reports a Δi value larger than 10. Based on this result, Model1 is proposed to explain the relationship between EI, burnout and general health.
Test of fit for the proposed and alternative models.
| χ2/df | CFI | RMSEA | AIC | Δi | |
|---|---|---|---|---|---|
| Model0 | 15.07 | .882 | .127 | 50605.324 | |
| Model1 | 4.64 | .959 | .065 | 50445.968 | 159.356 |
Note: (χ2/df): chi-square by degrees of freedom, (CFI): comparative fit index, (RMSEA): root mean square error of approximation, (AIC): Akaike Information Criterion, Δi=Delta AIC
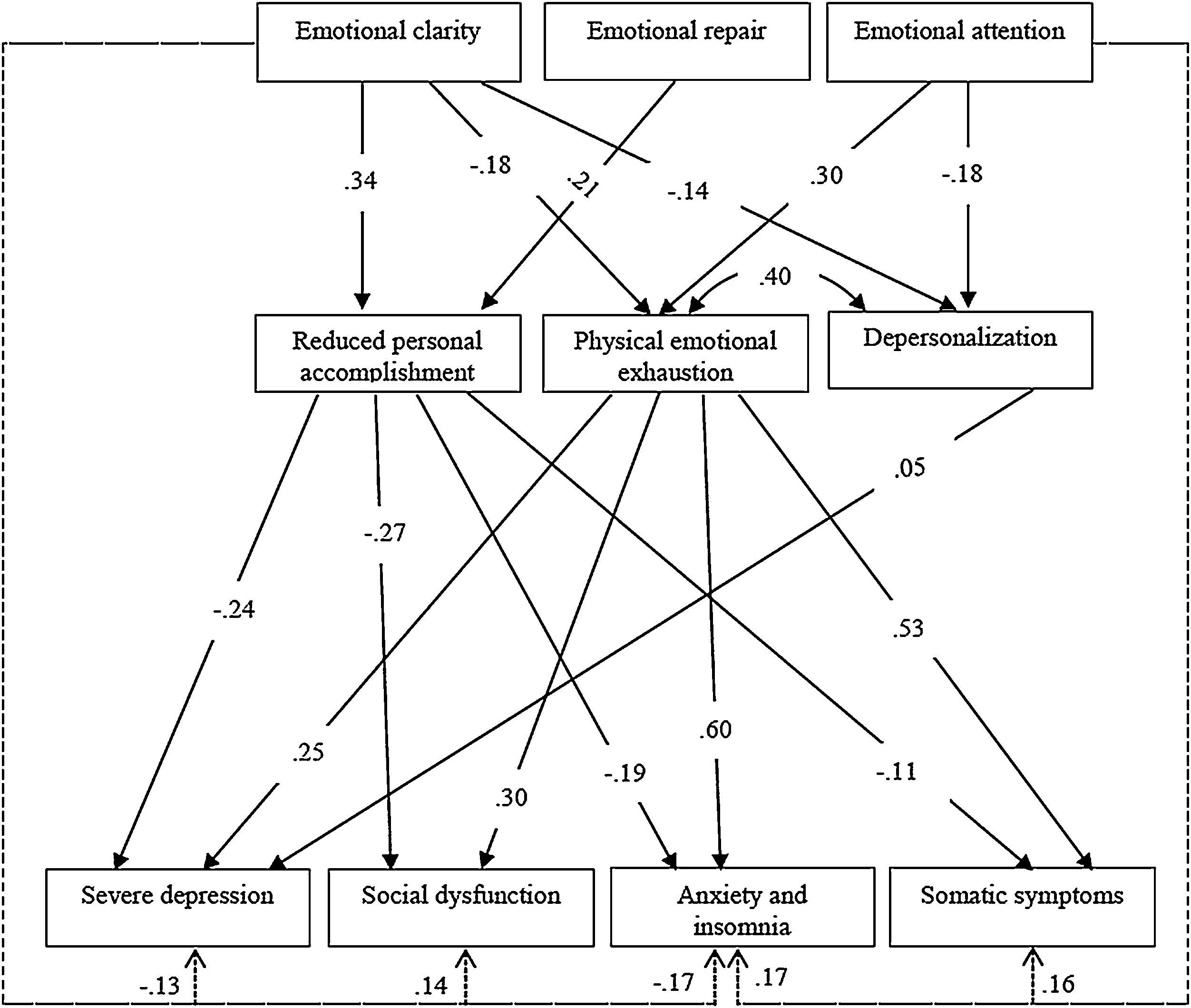
The path analysis (Figure 3) shows both the relationship between the three variables of interest and, by dotted lines, the main indirect effects that EI has on the dimensions of general health. The standardized magnitude of the direct effects is indicated by the arrows which represent that relationship. Because of the amount of information, only the highest standardized values of indirect effects are shown. Furthermore, the diagram shows the covariance between the dimensions of depersonalization and emotional and physical exhaustion. All the effects, except the one which depersonalization exerts on depression, are statistically significant. As can be seen, emotional attention and clarity exert the highest effect both over burnout and health issues. In relation to burnout, exhaustion and reduced accomplishment dimensions show the highest effect over psychological (especially anxiety and insomnia) and somatic symptoms. In addition, the model proposed allow to predict the response variable variation in general health in an acceptable way, highlighting the predictive power reached by somatic symptomatology (R2=.295) and anxiety and insomnia (R2=.395).
Discussion and Conclusions
On analyzing the relationship between EI and burnout syndrome, the results of the CCA show how, in the right-hand part of the graph (Figure 1), the items of the emotional attention dimension are divided into two blocks. This segmentation may be due to the fact that items P4, P1 and P3 refer to rational decisions related to the emotional life of the priests (e.g. P3: I often think about my feelings), whereas items P2, P5, P6, P7 and P8 reflect emotional control (e.g. P5: I let my feelings interfere with what I am thinking). This possible explanation is based on Rational Emotive Behavior Therapy (REBT; Ellis, 1962), according to which, uncontrolled emotions and unsuitable behavior are the result of a person's interpretation of specific situations, which give rise to irrational beliefs, as well as negative emotions and dysfunctional behaviors.
Those items related to thoughts derived from emotions -P2, P5, P6, P7 and P8-, have a positive correlation with the exhaustion and depersonalisation dimensions of the MBI. There is also a high covariation between the personal achievement items and the emotional repair and clarity dimensions, which is in accord with previous research (Landa, Berrios-Martos, López-Zafra, & Aguilar, 2006; Miller-Clarkson, 2013). These results suggest that priests who have high self-esteem and/or consider themselves fulfilled, tend to demonstrate higher values of EI in turn and it is precisely those priests who do not suffer from burnout. The results confirm the suggestions from authors such as Chang (2009) or Ângelo and Chambel (2015), who states that, in addition to the environmental variables that each individual experiences, there is a mix of factors related to emotions which makes a significant contribution to the syndrome's development.
On analyzing the relationship between EI and health, the highest relationships are found between emotional attention and dimensions related to depressive and somatic symptomatology and problems of anxiety and insomnia. On the contrary, both emotional clarity and emotional repair show a negative relationship with insomnia and somatic, anxiety, and depression symptomatology. Those participants who present this symptomatology tend to focus in a large part on their feelings, and demonstrate difficulties in understanding and regulating their emotional states, confirming the importance of understanding emotional experiences (Kendall et al., 2014). These results are in accord with other work and demonstrate the previously mentioned relationship between EI and health (Balluerka, Aritzeta, Gorostiaga, Gartzia, & Soroa, 2013).
While bearing in mind that the present study has a cross-sectional design, it seems reasonable to state that EI has an important role when trying to reduce the risk of suffering possible health problems, both somatic and psychological. In accord with previous research (e.g. Di Fabio & Saklofske, 2014; Higgins, Bailey, LaChapelle, Harmanc, & Hadjistavropoulos, 2015; Yin, 2015), people who understand and appropriately manage their emotions have a lower risk of suffering psychological and somatic problems inasmuch as they know how to analyze and cope with the possible effects, and avoid ending up suffering from any kind of pathology. In this case, these people will show a lower risk of suffering specific disorders such as burnout syndrome, which is especially associated with an inability to cope with long-term stressful situations (Ben-Zur & Michael, 2007; Chaves & Park, 2015).
Although it is possible to refer to the variables in a general way, analyzing the role of the dimensions which make up the model, shows which specific dimensions have more weight when it comes to explaining this health issue. This allows, in turn, the definition of which dimensions would need to be addressed to deal with an issue. Emotional attention and emotional clarity have shown the main effects both on burnout syndrome and psychological and somatic issues. These findings are in line with previous research in which clarity and emotional repair were found to be two consistent predictors for wellbeing (Landa, Pulido-Martos, & López-Zafra, 2010).
The estimation of indirect effects (Figure 3) allows the analysis of the extent to which emotional attention and emotional clarity have the largest effect on the appearance of health issues moderated by physical and emotional exhaustion. These results, regarding the importance of the emotional attention and clarity dimensions, and exhaustion in burnout, as well as the explained variance of health problems from EI, confirm the conclusions from previous research (e.g. Cheung et al., 2015; Hui-Ching et al., 2011). In short, both specific disorders such as burnout and general health were found to be related to EI, in this case, of priests. This data confirms the hypothesized role played by EI when it comes to physical and psychological wellbeing founded on previous research (Ju et al., 2015; Shariff, 2013).
Any intended intervention program must especially focus on emotional clarity and emotional attention, as they seem to be the dimensions which are most relevant in reducing or preventing burnout syndrome and improving wellbeing.
Priests are a group which are vulnerable to various emotional and somatic health issues (Nicholson, Rose, & Bobak, 2010), something which may be prevented by the development of an appropriate intervention program (Martins, Ramalho, & Morin, 2010). Therefore, given the role that EI has been shown to play in significantly reducing psychological and somatic problems (especially anxiety related symptomatology), education about emotions should be an integral part of training for the priesthood. Different papers have demonstrated that insight by itself is not an effective coping mechanism (Boals, Valentine, & Beike, 2015). So, in addition to be mindful of their situation, it is advisable to give priests skills which will allow them to develop behaviors with the aim of improving their EI, and maintaining their wellbeing (Stewart-Sicking, 2012).
Moreover, priests are a particular professional group, for whom personal fulfillment is a fundamental aspect because the vocation of their profession. In this sense, it is important to consider both the adjustment of interpersonal goals and the effect that personal accomplishment exerts on different aspects, but especially on their wellbeing (e.g. Duarte & Pinto-Gouveia, 2015). So, this is an important aspect that should be valued, both by the health of priests and its important social role. Regarding burnout syndrome, it is important to highlight the low reliability coefficient obtained in relation to depersonalization dimension (α=.54). Although the estimated value is similar to those found on previous papers (e.g. Raj & Dean, 2005), this aspect could affect to the reliability of the scores obtained and, especially important, to the decisions make based on those scores. The underpinning of the low coefficient could be the shorter length of this dimension in comparison with dimensions of exhaustion and personal accomplishment, and the lower correlations inter-items found. So, future papers focus on content validity evidence of this dimension could be useful.
The principal limitation of this study is that, despite having a large sample size, representing practically 80% of the population in this field, the nature of the study is cross-sectional. In addition to this, it is important to note that, despite the large sample size, participants were not randomly selected. Moreover, the data was collected by means of self-reporting, consequently possible mono-method bias and problems related with “faking” may be implied. So, alternative assessing methods such as vignettes could be considered (Hinz, Häuser, Glaesmer, & Brähler, 2016).
Future lines of research should involve, at the very least, a longitudinal design which would allow researchers to check both the validation of the current model and the preventive function that EI has in general health through the application of a clinical intervention program focused on EI. Also, it could be interesting to analyze if there are religious aspects of attending to emotion that might uniquely relate to symptoms assessed in this paper in comparison with general population typically studied.
Finally, to include participants from South American countries will increase the quality of the study and will enhance the results obtained, offering the possibility of comparing the established model between different regions in Latin-America.
