



Background/Objective: Ageing and progressive increase in life expectancy in people with intellectual disability present significant challenges. The present study is to examine the needs that arise in the aging process of this population. To detect these needs is fundamental to ensure personal wellbeing; almost no psychometrically sound instruments have been developed. Method: A structured interview was developed and evaluated by a panel of 20 experts to obtain evidence of content validity. The interview was then applied to 1,173 people with intellectual disability. The ages ranged from 35 to 80 (M=52.27; SD=7.5). Results: The interview consisted of 93 items evaluating four areas: perceived needs, personal problems, future perspectives, and solutions required. The results demonstrated the proximity and relationship of the various needs evaluated. In addition it was observed that those with intellectual disability who were older, male and users of residential services tended to indicate more needs, problems, and required more solutions. Conclusions: The instrument has adequate evidence of validity, allowing the evaluation of specific needs of people with intellectual disability. The results advocate the design of transversal intervention policies in order to effectively meet the needs and requirements of this population.
Introducción/Objetivo: El envejecimiento y progresivo incremento de la esperanza de vida de las personas con discapacidad intelectual supone importantes retos. El presente estudio examina las necesidades relacionadas con el proceso de envejecimiento de estas personas. La detección de dichas necesidades resulta fundamental para asegurar su bienestar personal, siendo necesarios instrumentos de evaluación que muestren garantías psicométricas. Método: Se elaboró una entrevista estructurada valorada por un panel de 20 expertos para la obtención de evidencias de validez de contenido. La entrevista fue aplicada a 1.173 personas con discapacidad intelectual de entre 35 y 80 años (M=52,27; DT=7,5). Resultados: La entrevista consta de 93 ítems que evalúan cuatro áreas: necesidades percibidas, problemas personales, perspectivas de futuro y soluciones demandadas. Se muestra la proximidad e interacción de las diferentes necesidades evaluadas y la tendencia a que sean las personas con discapacidad intelectual de mayor edad, hombres y usuarios de servicios residenciales quienes refieran mayor número de necesidades y problemas, y demanden más soluciones. Conclusiones: El instrumento desarrollado muestra adecuadas evidencias de validez, permitiendo evaluar necesidades específicas de las personas con discapacidad intelectual. Los resultados abogan por el diseño de políticas de intervención transversales que permitan cubrir eficientemente las necesidades y demandas de este colectivo.
The progressive increase in life expectancy has had an effect on people with disabilities in general and those with intellectual disabilities (ID) in particular (Ng, Sandberg, & Ahlström, 2015). We find ourselves facing a social phenomenon which poses significant, unexpected challenges, and key amongst those challenges will be the political and professional response to both the new needs these older people with ID present, and the exacerbation of already existing needs (Beadle-Brown, Bigby, & Bould, 2015; Lehmann et al., 2013; McCausland, Guerin, Tyrrell, Donohoe, O’Donoghue, & Dodd, 2010; Townsend-White, Pham, & Vassos, 2012).
Schalock and Verdugo's (2012, 2013) quality of life model, which has evolved into a validated multidimensional conceptual model composed of core domains and domain indicators (i.e., personal development, self-determination, interpersonal relations, social inclusion, rights, emotional well-being, physical well-being and material well-being), has the same components for all people, has both subjective and objective components, is enhanced by self-determination, resources, purpose in life, and it is experienced when the person's needs are met (Schalock & Keith, 2016). This model includes among its premises meeting the needs of people with disabilities as a fundamental principle for personal wellbeing, highlighting the evaluation of those needs (Simões, Santos, & Biscaia, 2016). In old age these needs are accentuated, as the problems associated with the disability, which may involve significant limitations and adjustments, are added to by problems due to the ageing process itself. The changes and adjustments affect various areas. The physical disorders most often found in the population of older people with ID are related to problems of mobility, the senses and endocrine system along with cardiovascular, respiratory, joint and bone issues, problems which are more pronounced and serious than in the general older population (Haveman et al., 2011; Winter, Hermans, Evenhuis, & Echteld, 2015). Cognitive decline and mental health problems also particularly affect this group. The most commonly referred psychological problems include; the lack of ability to communicate feelings, react to stress or tolerate changes to routines, depressive feelings and the presence of dementia, especially the increased propensity to Alzheimer's in adults with Down syndrome up to 30 years earlier than in the general population (Glasson, Dye, & Bittles, 2014; Hermans & Evenhuis, 2014; McCarron et al., 2013; Winter et al., 2015). In addition, social interaction and participation decreases significantly due, amongst other things, to the difficulties of access owing to frequent existing obstacles, changes of residence, and the loss of loving ties (Judge, Walley, Anderson, & Joung, 2010). In order to properly assess and use personal outcomes, it is necessary to develop psychometrically sound measurement instruments that are based on an empirically validated quality of life model (Arias, Verdugo, Navas, & Gómez, 2013; Carbó-Carreté, Guàrdia-Olmos, & Giné, 2015).
Despite the importance of this topic, the majority of the scientific literature has centered on the group of people with ID as a whole, without dealing with the specific needs of those who are ageing (e.g., Jahoda et al., 2015). The scarce data in the published literature indicate that these older people's perceived needs are related to personal health, economic resources, health resources, social service resources, and the presence of obstacles (Aguado, Alcedo, & Fontanil, 2012; Navas, Uhlmann, & Berastegui, 2014; Ouellette-Kuntz, Martin, & McKenzie, 2015). As in the general elderly population, these needs have often been neglected and forgotten (Buys, Aird, & Miller, 2012; Hole, Stainton, & Wilson, 2013; McCausland et al., 2010), which is why it continues to be a topic that lacks empirical foundations and why there has been hardly any development of evaluation instruments aimed at this construct. In summary, according to the current research perspectives on this topic (Schalock et al., 2014), the aim when assessing these needs is to improve personal results and to increase the evidence-based practices that enhance the quality of life of people with ID. All at once, to emphasize the importance of the people with ID involvement in the design and implementation of their person-centered planning (Schalock et al., 2014).
While there are various useful instruments for the assessment of quality of life in people with ID in adulthood and in old age in the Spanish context (e.g. INICO-FEAPS scale; Verdugo et al., 2013. The San Martín scale; Verdugo, Gómez, Arias, Navas, & Schalock, 2014. And the Personal Outcomes Scale; Carbó-Carreté et al., 2015), there is only one specific instrument which can identify the profile and level of support needs in this stage of life (Support Intensity Scale, SIS; Verdugo, Arias & Ibáñez, 2007).
For these reasons, and following the latest research on ID (Stancliffe, Tichá, Larson, Hewitt, & Nord, 2014), the general aim of this current study is the development and validation of a structured interview- Interview for Needs Assessment of Ageing People with Disabilities, ENDE. This instrument will allow the collection of information about perceived needs in older people with ID, the personal problems which affect them most, the outlook for the future that they see, and the solutions that they consider most appropriate to meet their requirements. Secondly, the influence of different variables, identified as relevant in the literature, will be analysed, such as sex, age, habitual residence (living at their own homes or in residential accommodation) and assessment method (self-application or information collected by others).
MethodParticipantsThe interview was given to a convenience sample made up of 1,173 people with ID who were resident in 16 of the 17 autonomous communities in Spain. Women made up 41.6% of the sample. The age of those assessed ranged between 35 and 80 (M=52.27; SD=7.5). In terms of habitual residence, 48.70% of the participants lived in their own homes, while the remaining 51.30% lived in residential accommodation. Considering the degree of recognized disability (based on R.D. 1856/2009, December 4) 88.4% of the participants showed a degree larger than 65% while the remaining 11.6% showed a disability between 33 and 65%. In 28.7% of cases the person with ID themselves provided the information and data about their needs and requirements (self-application), because their verbal ability (i.e. understanding and verbal expression) were adequate to respond to interview items (the participants mostly showed basic skills in reading and writing). The remaining 71.3% of responses to interviews were given by families (18.7%) or professionals who knew the person with ID well (52.6%). In these cases, the requirements for responding the interview were: (a) knowing the participant for at least six months and (b) having sufficient opportunity to observe the participant for long periods of time along several situations.
InstrumentThe structured interview was created with a combination of 128 items allowing the evaluation of the following areas: perceived needs (split into six categories: personal health, economic resources, health resources, social services resources, physical and social obstacles, support measures and networks), personal problems, future outlook, institutional measures and support, and solutions needed. These items were developed by independent experts in ageing and disability according to recent recommendations in the psychometric literature (Moreno, Martínez, & Muñiz, 2015).
A study was carried out in order to refine the initial items and obtain evidence of content validity with the participation of a panel of 20 experts with significant experience in disability in both practical and academic fields. The study was performed in two phases: firstly, to evaluate suitability, all of the items were presented for the experts to assign each one to the area they thought relevant. In the second phase, the same experts judged the relevance of each item in terms of evaluating the area it had been assigned to.
ProcedureOnce the instrument met the psychometric requirements, contact was made with organizations that provide services to people with disability in the various communities in Spain, explaining the aims of the research and requesting participation. The research team communicated with those organizations who showed an interest in participating. The Ethics Committee of the hosting University granted ethical approval. The principles for conducting research contained in the Declaration of Helsinki were respected. Permissions and informed consents were collected by participating organizations or provided by family or professionals. Removing names and using identifying codes that were not known by the researchers guaranteed confidentiality and anonymity.
Data analysisValidation of the instrument was accomplished by analysing the results of the expert panel, removing those items which failed to achieve agreement from two thirds of the judges (i.e., 14 similar responses) on the appropriateness of their assignment to an area of evaluation. Then, the Content Validity Coefficient was calculated (CVC), which considers the number of participating experts, reducing possible bias in the evaluation (Pedrosa, Súarez & García-Cueto, 2013). As an index of double validation, Aiken's V coefficient was calculated (Aiken, 1980), which allows the estimation of confidence intervals independently of the shape of the underlying distribution. In addition, owing to the low variability in the experts’ responses, the cosine between the scores the judges awarded for items belonging to different areas was calculated in order to analyse consensus among their opinions.
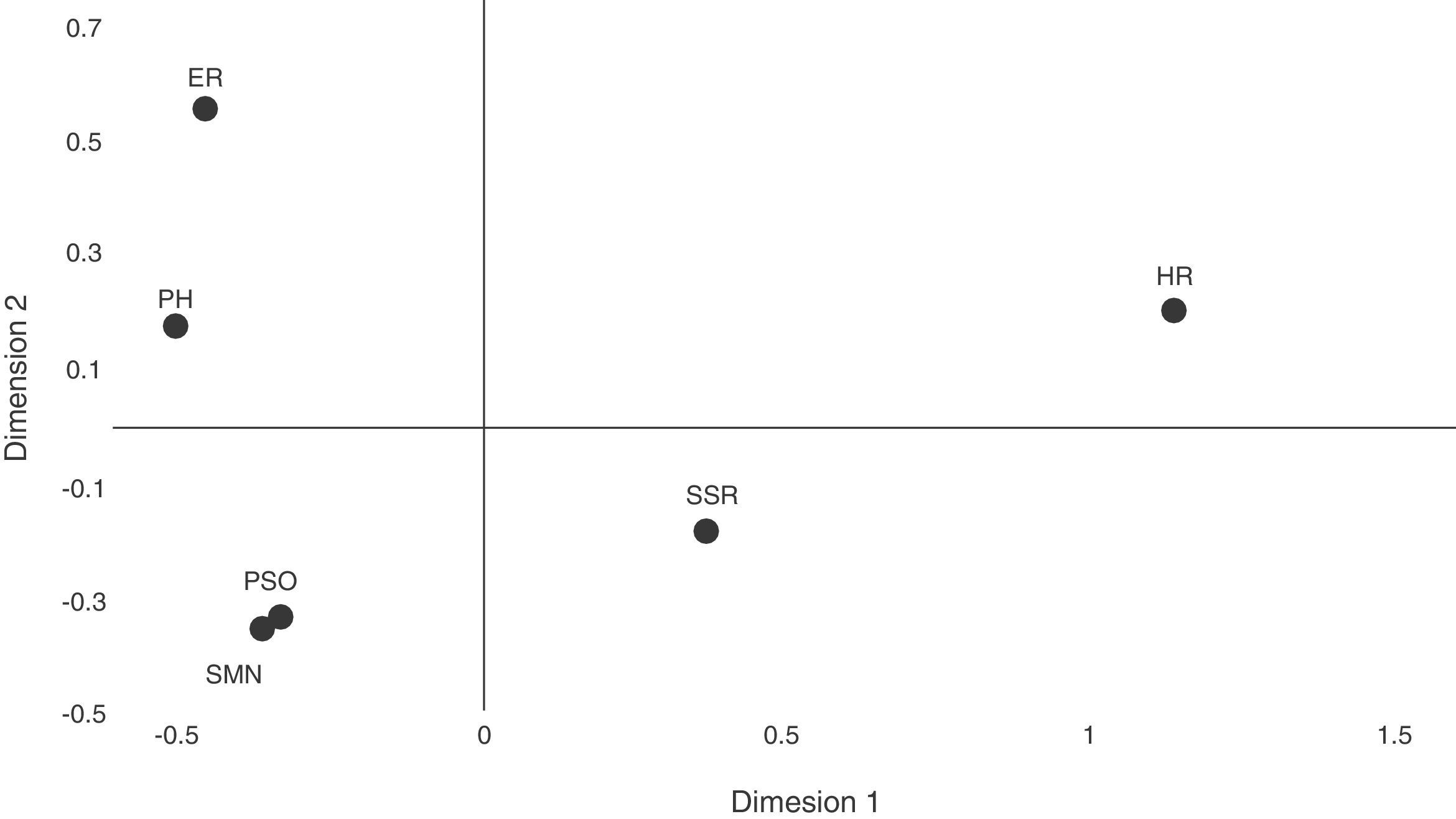
Once the final instrument had been defined (https://goo.gl/Cb0BJI), multidimensional scaling was used to graphically analyse the proximity and relationships as perceived by the participants between the various evaluated areas (Carroll, 1980). The graphical solution was limited to two dimensions for simplicity. The procedure locates each category in each of two dimensions. Large distances between categories in this two-dimensional space indicate dissimilarity between the categories (Borg & Groenen, 2005). This procedure was applied to the data belonging to the perceived needs area, using the Proxscal method to create the data proximities. The goodness of fit to the model was tested using the Stress index (Kruskal, 1964).
Finally, the fit of the data to the normal distribution was tested using the Shapiro-Wilk test. A study was performed of the differences of means for each of the areas making up the interview in terms of predictive variables: sex, age, habitual residence, and assessment method. The total score of each participant was obtained based on the number of perceived needs in each area. Owing to the violation of the assumption of normality, this study of differences of means was performed using the Mann-Whitney U statistic, the effect size was estimated using Cliff's delta (Cliff, 1993).
ResultsEvidence of content validityItems were removed from the original instrument if there was a lack of agreement on their relevance to an area. In addition, the area institutional measures and support was removed as the items in this area were mostly classified by the experts as relevant to the solutions needed area. Following that, items which had a CVC lower than .80 were eliminated, leaving a total of 93 items grouped into the four previously mentioned areas with a total CVC of .89. The areas with lower values of Aiken's V coefficient were solutions needed and social support networks. Both gave a coefficient of .85 [.75-.91; CI=95%], which indicates high representativeness with respect to the content evaluated. In all other cases the coefficients were higher. Furthermore, the values of the cosine matrix between the experts’ scores of item relevance were above .93 in all cases.
Multidimensional representation of perceived needsOnce the final version of the instrument was determined, the multidimensional scaling process was applied. The aim was to analyse the relationship between the different categories making up the area of needs as perceived by the participants and to see which are closest for them. The model gave a Stress value of<.001, indicating an excellent fit according to the criteria of Kruskal (1964).
As can be seen in Figure 1, dimension 1 defines a continuum going from those needs related to personal aspects and the immediate environment to those needs more associated with contextual, more external factors. Needs related to personal health, individual and family economic resources are on the left of the chart, more social aspects in the middle, and health resources on the right. Dimension 2 goes from needs related to service provision, such as economic and health resources, to those which are more relational, such as social services, social barriers, and social support measures and networks.
Study of differences
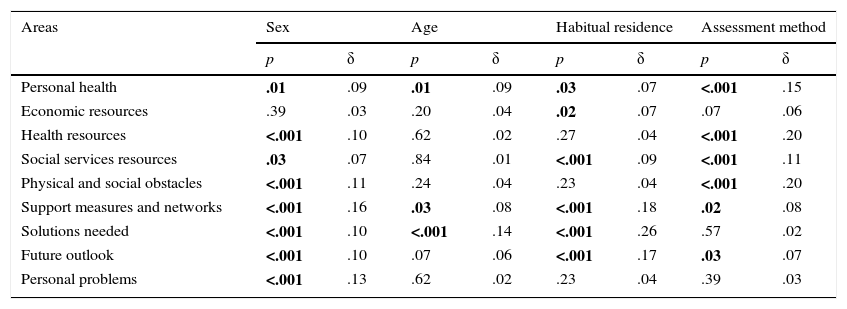
The differences in means were statistically significant in practically all areas in terms of the predictive variables (Table 1). In general, men and those participants who use residential services tended to indicate more needs, problems and solutions. In terms of the way the interview was conducted, where participants themselves answered the interview questions, they related more needs, whereas in cases where the answers were given by third parties this tendency was reversed, with the proxies giving more solutions, future perspectives, and personal problems.
Study of the difference in means in terms of predictive variables.
| Areas | Sex | Age | Habitual residence | Assessment method | ||||
|---|---|---|---|---|---|---|---|---|
| p | δ | p | δ | p | δ | p | δ | |
| Personal health | .01 | .09 | .01 | .09 | .03 | .07 | <.001 | .15 |
| Economic resources | .39 | .03 | .20 | .04 | .02 | .07 | .07 | .06 |
| Health resources | <.001 | .10 | .62 | .02 | .27 | .04 | <.001 | .20 |
| Social services resources | .03 | .07 | .84 | .01 | <.001 | .09 | <.001 | .11 |
| Physical and social obstacles | <.001 | .11 | .24 | .04 | .23 | .04 | <.001 | .20 |
| Support measures and networks | <.001 | .16 | .03 | .08 | <.001 | .18 | .02 | .08 |
| Solutions needed | <.001 | .10 | <.001 | .14 | <.001 | .26 | .57 | .02 |
| Future outlook | <.001 | .10 | .07 | .06 | <.001 | .17 | .03 | .07 |
| Personal problems | <.001 | .13 | .62 | .02 | .23 | .04 | .39 | .03 |
Note. p=associated probability; δ=Effect size (Cliff's Delta).
With respect to age, bearing in mind previous studies which indicate that as people age, their needs increase considerably (Navas et al., 2014; Ng et al., 2015), the participants were divided into two groups: those 54 and under, which grouped together adults in the early stages of ageing (67.70% of participants), and those over 54 (32.30%), in the later stages of the ageing process. The results show that the older group tended to indicate more needs, except in personal health and health services, where the pattern is reversed. Despite this, statistically significant differences were only observed in personal health, social support measures and networks, and solutions required. While bearing in mind the differences, it is worth underlining that the effect size is small in almost all cases.
DiscussionAlthough the Interview for Needs Evaluation of Ageing People with Disabilities (ENDE) can only be considered a first step towards the evaluation of this construct, it answers the growing demand for evaluation instruments with appropriate psychometric properties for people with ID (Bergström, Hochwälder, Kottorp, & Elinder, 2013; McCausland et al., 2010). It has sufficient evidence of content validity for suitability and relevance, with a CVC greater than .85 in all cases being especially notable.
The results of the multidimensional scaling of the participants perceived needs show two clearly defined dimensions which is consistent with results from previous research. Personal needs, specifically those related to health (e.g., daily individual care, and functional limitations which were the most identified) were seen to be very close to economic resources (e.g., family economic situation, economic independence). This proximity is logical given that a high level of functioning and minimisation of negative consequences are vitally important factors to these people, and individual or family solvency eases access to resources which provide significant health improvements. However, older people with ID do not have sufficient guaranteed economic rights (Navas et al., 2014), so it is no surprise that an increase in pensions was the most requested solution amongst the participants. In this continuum there was also proximity between physical and social obstacles (e.g., societal acceptance and the presence of architectural obstacles) and items concerned with social support measures and networks (e.g., where and who to live with in the future, and the future of the family). In fact, full social inclusion for these people will only happen with the elimination of prejudice and current stereotypes about them and with the eradication of myths about ageing (Bertolli et al., 2011). In that respect there is significant consensus about the principles of action needed in order for this group to have a good quality of life as they age. Such actions must be aimed at reinforcing their inclusion in the community, their self-determination, and helping them receive maximum family support (Hole et al., 2013; Lehmann et al., 2013).
Needs related to social service resources, the category with the third highest number of responses, are perceived by the participants as closest to those related to health resources. This goes from needs at an individual level, or in the immediate environment, to those needs at service provider level, both social (e.g., home help, the need for more and better social centres and residential services) and health (e.g., improvements in hospital and home care quality, more and better health centres, and access to physiotherapy). The significant shortcomings in these services, which have been well documented in the literature (e.g., Navas et al., 2014; Ouellette-Kuntz et al., 2015), impede access for older people with ID, whether to routine medical attention, or to leisure or free time activities. In addition to that there is the fragmentation between health and social services, and the absence of specific and coordinated responses. Faced with this situation, the participants demand as a matter of urgency and priority, better training for health and social service professionals in topics related to ageing in this group and increased leisure services, among many other solutions.
The results of this study show that the needs, solutions, problems and future perspectives perceived and indicated by those with ID who completed the interview are mediated by interaction with specific predictive variables. Those who live in residential environments indicate more needs in all areas of the interview than those who live in their own homes. These results support the proposal in Article 19 of the United Nations Convention on the Rights of Persons with Disability (United Nations, 2006). According to that article the most effective model for ageing people with ID is one which fits support and services to the reality of the person, where they live, without the creation of specialised segregated services away from the place where the person grew up or has lived for many years. The problem lies in the lack of policies which facilitate these objectives (Bigby, Bowers, & Webber, 2010). In terms of age and sex, the data indicate that, in general men and older people perceive and indicate more needs, solutions, and problems. There are very few studies in terms of sex which have covered the specific topic of needs and the results are usually rather inconsistent (Aguado et al., 2012). In contrast there is empirical support regarding the increase in needs with advancing age, especially due to the presence of the high comorbidity of disorders (Haveman et al., 2011; McCausland et al., 2010; Navas et al., 2014). Finally, the differences in terms of interview completion show that older people with ID indicate more needs in all areas while families and professionals give more solutions (e.g., help for daily personal care and increased family help), more personal problems (e.g., health problems and difficulty in making decisions), and future perspectives (e.g., living with a good quality of life and personal autonomy). These differences might be due to the fact that the proxies see the need for more support in this stage of life in which people face the dual difficulties of ageing and disability. In fact, both intervention programmes and policies about the needs of this group should be transversal and cover micro- to macro-social aspects, as the results of the multidimensional scaling indicate.
In summary, and in line with some other authors (e.g., Buys et al., 2012), the information collected by this instrument may be of great use not only to professionals in providing appropriate support to older people with ID, but also to their families and, of course to the older people with ID themselves by having data about needs and solutions that facilitate and promote an active lifestyle in this stage of life. Despite the adequate psychometric properties of this interview, this study does have some limitations. The main limitation is that, although the number of participants was high and from diverse origins (from practically all of the autonomous communities in Spain), they were evaluated using a convenience sample, limiting the evaluation to those who agreed to participate in the study. In addition, although the interview allowed two methods of completion, a high percentage of the answers were given by third persons, so work remains in looking more closely at people's own perspectives through self-reporting and removing possible obstacles in the process, such as those related to limitations in communication and comprehension (Balboni, Coscarelli, Giuntia, & Schalock, 2014; Koch et al., 2015; Simões et al., 2016; Stancliffe et al., 2014). Despite this, the main challenge must be to provide the opportunity to people with ID to participate in their own assessment for exercising their right of self-determination (Verdugo et al., 2015).
Future lines of research should aim to develop similar instruments which can be adjusted to the peculiarities and special needs that certain subgroups, such as ageing people with ID, can present. The results of these standardised evaluations can guide approaches to modernise policies and professional practice most effectively for the promotion of healthy, active ageing for this group of people.
FundingThis study was supported in part with funding (SV-15-GRUPUO-GID) from Plan for Science, Technology and Innovation 2013-2017 of Asturias (Spain).The authors would like to thank the organizations, people with intellectual disability, professionals, and families for completing the interview
