



There is increasing evidence that positive life changes, such as posttraumatic growth (PTG), can result from the experience of coping with cancer. However, no interventions have been specifically designed to facilitate the development of PTG in cancer. In this article, we describe and assess the results of Positive Psychotherapy for Cancer (PPC) survivors. It aims to facilitate PTG as a way of achieving significant reductions in the symptoms of emotional distress and posttraumatic stress. In addition, the corroboration of this PTG facilitation is assessed using interpersonal indicators. Method: We allocated 126 consecutive survivors of cancer with high levels of emotional distress and who were seeking psychological support to either an experimental group (PPC) or a waiting list group. Results: The PPC group obtained significantly better results after treatment than the control group, showing reduced distress, decreased posttraumatic symptoms, and increased PTG. The benefits were maintained at 3 and 12 months’ follow-up. Participants’ PTG was correlated to the PTG that their significant others attributed to them, corroborating PTG facilitation. Conclusions: PPC appears to promote significant long-term PTG and can reduce emotional distress and posttraumatic stress in cancer survivors. In addition, PTG facilitation induced by PPC is corroborated by significant others.
La evidencia científica muestra la importante presencia de cambios vitales positivos, como el crecimiento postraumático (CPT), tras afrontar un cáncer. Sin embargo, ninguna intervención ha sido específicamente diseñada para facilitar el CPT en pacientes con cáncer. En este artículo, se describen y evalúan los resultados de la Psicoterapia Positiva dirigida a supervivientes de Cáncer (PPC), diseñada para facilitar el CPT como vía para reducir el malestar emocional y estrés postraumático. Utilizamos indicadores interpersonales para validar la autenticidad del CPT. Método: Ciento veintiséis supervivientes de cáncer con elevados niveles de malestar emocional fueron consecutivamente asignados al grupo experimental (PPC) o al grupo de lista de espera. Resultados: El grupo de PPC obtuvo significativamente mejores resultados después del tratamiento que el grupo control, mostrando una reducción del malestar psicológico, de los síntomas de estrés postraumático y un incremento del CPT. Los beneficios se mantuvieron a los 3 y 12 meses. El CPT fue corroborado por los seres queridos de los participantes. Conclusiones: La PPC parece promover de forma significativa el CPT y reduce el malestar emocional y el estrés postraumático en supervivientes de cáncer. Además, la facilitación de CPT inducido por la PPC es corroborada por los seres queridos.
Severe illnesses like cancer are adverse life experiences that have a high psychological impact. Many investigations have explored the negative psychological consequences of cancer, which include fatigue, distress, depression, and posttraumatic stress (Haberkorn et al., 2013; Sheppard, Llanos, Hurtado-de-Mendoza, Tailor, & Adams-Campbell, 2013). In fact, 35%–38% of patients develop distress when diagnosed with cancer (Carlson, Waller, & Mitchell, 2012). There is also a considerable body of evidence associating this distress with poorer quality of life, less adherence to cancer treatments, and worse overall survival, as well as poorer self-care and a less healthy lifestyle (Antoni, 2012; Spiegel, 2012).
In addition to distress, a cancer diagnosis can trigger positive life changes in survivors (Ochoa, Castejon, Sumalla, & Blanco, 2013; Sawyer, Ayers, & Field, 2010; Sumalla, Ochoa, & Blanco, 2009). These positive changes have been conceptualized as posttraumatic growth (PTG) in the literature. PTG refers to positive cognitive and behavioral changes after adversity and trauma. According to the influential model of Tedeschi and Calhoun (1996), positive changes can be observed in several domains: a) self-concept (e.g., new valuation of one's own strength and resilience); b) appreciation of new possibilities in life; c) social relationships (e.g., feeling emotionally closer to others, especially family and friends); d) life philosophies (e.g., reordering of values and priorities); and e) spiritually (e.g., increased participation in religious activities).
The results of meta-analyses show that those patients with cancer who experience PTG tend to adapt to their illness more successfully, reporting better subjective physical and mental health, lower symptoms of distress and posttraumatic stress, as well as healthier behaviors and higher adherence to oncological treatments (Helgeson, Reynolds, & Tomich, 2006; Sawyer et al., 2010).
Traditionally, the focus of psychotherapy in cancer has been on stress reduction and on restoring the emotional state prior to illness. However, over the last two decades, psychology has placed greater emphasis on the positive aspects of human functioning, such as positive emotions, personal meanings, growth and strengths, which has led to the proposal of a number of successful positive psychology interventions in cancer to enhance quality of life and reduce distress (Casellas-Grau, Font, & Vives, 2014). A recent meta-analysis showed that those psychological treatments, which tend to reduce the most cancer participants’ depressive symptoms were, in turn, the ones which resulted in greater benefits on their quality of life (De la Torre-Luque, Gambara, López, & Cruzado, 2016). Moreover, positive psychology interventions showed their important effects in increasing affect (Woodworth, O’Brien-Malone, Diamond, & Schüz, 2016).
In this study, we applied a program of Positive Psychotherapy for Cancer (PPC) survivors that was developed through extensive research and a review of the literature on trauma and PTG (Ochoa et al., 2013; Sumalla et al., 2009; Vázquez, Pérez-Sales, & Ochoa, 2014). The basic aim of PPC is to facilitate PTG in cancer survivors, and it was designed to complement and enhance traditional psychological treatments, such as stress management (Antoni, 2003). Therefore, PPC focuses closely on a patient's positive resources, such as positive emotions, strengths, and personal meanings (Ochoa et al., 2010; Rashid & Seligman, 2013) because its assumption is that individuals have an inherent desire for growth, fulfillment, and happiness, rather than merely seeking to avoid misery, worry, or anxiety. A substantial portion of suffering, emotional distress, and psychopathology in cancer is related to the enormous and urgent need to make positive life changes (growth), which arises after the total or partial awareness of their mortality (Ochoa & Casellas-Grau, 2015). Then, an important part of a cancer survivor's suffering could be related to the frustration of this need of growth after the threat to life. As a recent meta-analysis explores (Roepke, 2014), the facilitation of PTG could therefore provide an important psychotherapeutic framework when seeking to reduce high and sustained levels of distress and posttraumatic stress after oncological treatment.
In their organismic valuing theory of adaptation to threatening events, Joseph and Linley (2006) explain how emotional distress and PTG could be integrated in the same framework of human experience. They distinguish two main processes in the adaptation to threatening events: assimilation and accommodation. Assimilation focuses on managing the stressful event and trying to make it consistent with their basic beliefs to keep them from changing. The presence of severe distress or posttraumatic stress points to the need for elaboration of the traumatic event that is causing the individual to question their vision of themselves, the world, and others. The maintenance of posttraumatic stress and emotional distress can be broadly used as indicators of a difficult or dysfunctional assimilation. In contrast, accommodation represents the changes that the person makes to their basic beliefs when seeking to incorporate an intense and difficult experience. When promoting PTG, we are facilitating this process to reduce distress and posttraumatic stress in response to the traumatic information trigger (i.e., the cancer experience).
A relevant debate for therapies focused on facilitating PTG concerns the “real” or “illusory” nature of PTG in cancer (Sumalla et al., 2009; Widows, Jacobsen, Booth-Jones, & Fields, 2005). The models that emphasize the illusory nature of the PTG processes identify assimilation as the operative mechanism (Joseph & Linley, 2006; Sumalla et al., 2009) and question the presence of positive identity changes; thus, they argue that PTG is merely a coping strategy. It is claimed that this strategy or “positive illusion” aims to counteract or protect the individual from the distress caused by calling into question the coherence, sense, and self-esteem of the subject's identity, as a result of the illness (Taylor, Kemeny, Reed, Bower, & Gruenwald, 2000). Two interpersonal indicators have been used to corroborate the authenticity of PTG that are based on the information given by patients’ significant others regarding the cancer patient's PTG (Ochoa et al., 2013). One indicator is the “relational” or “vicarious” PTG reported by significant others (usually partners) in themselves after the experience of their loved one's illness. The other interpersonal indicator is the “transmitted” or “corroborated” PTG where significant others report whether the cancer survivor has demonstrated PTG (Moore et al., 2011). Thus, if significant others show vicarious growth or can corroborate the patient's growth, the authenticity of the cancer survivor's growth is improved (Moore et al., 2011; Ochoa et al., 2013).
In view of these considerations and the lack of specific data in this area, we aimed to evaluate the effects of PPC on posttraumatic stress and distress reduction through PTG facilitation among cancer survivors compared to a waiting list (control) group. The study also assessed the authenticity of PTG facilitation by PPC, using interpersonal indicators.
MethodsParticipantsOne hundred and fifty-eight women with diverse cancer diagnoses were recruited between April 2008 and October 2013. Participants were referred by medical oncologists or nurses to the psycho-oncology unit of a comprehensive cancer center (the Duran i Reynals Hospital) if they presented emotional distress at the end of their primary oncological treatment. Distress thermometers were used and patients with scores ≥ 5 were referred to the psycho-oncology unit. In a southern European cancer sample, this cut-off point was found to be appropriate for detecting general psychosocial morbidity (Gil, Grassi, Travado, Tomamichel, & Gonzalez, 2005). Participants meeting the following inclusion criteria were then invited to participate: (a) age 18–70 years old; (b) presence of a single primary cancer; (c) primary oncological treatment (surgery, chemotherapy, or radiotherapy) completed; (d) presence of significant clinical distress, with a global score of 10 or more on the HADS (The Hospital Anxiety and Depression Scale); and (e) ability to understand and read Spanish. We excluded patients if they reported any prior cancer, any prior or current severe mental disorders (hospitalization or formal diagnosis of psychosis, suicidality, or substance dependence), or any major concurrent medical disease seriously affecting their cognitive performance (e.g., neurologic disorders). Participants were assessed at baseline (T0), immediately after PPC treatment (T1), and at 3 months (T2) and 12 months (T3) after treatment. The study was carried out according to the latest version of the Declaration of Helsinki. Approval was given by the ethics committee of our hospital and all participants gave written informed consent.
InstrumentsWe used validated questionnaires to assess mood (distress), posttraumatic stress, PTG, and extreme life events.
Mood. The Hospital Anxiety and Depression Scale (HADS) measures anxiety and depression in people with physical illness (Zigmond & Snaith, 1983), and has been widely used to assess mood in patients with cancer. There are seven items for both anxiety and depression, with total scores ranging from 0 to 21. Costa-Requena, Pérez Martin, Salamero Baro, and Gil Moncayo (2009) validated the tool in a Spanish sample of oncology outpatients, with their results showing good internal reliability for each subscale (Cronbach's alphas of .82 and .84 for the anxiety and depression subscales, respectively). In the current sample, similar Cronbach's alphas were obtained (.79 for the anxiety scale and .84 for the depression scale).
Posttraumatic Stress. The Posttraumatic Stress Disorder Checklist-Civilian version (PCL-C; Weathers, Litz, Huska, & Keane, 1994) is a 17-item self-rating questionnaire. It uses a five-point Likert scale ranging from 1 (not at all) to 5 (extremely) that covers all of the diagnostic criteria for posttraumatic stress disorder in the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. The questionnaire yields both a total score and three subscale scores based on re-experiencing, avoidance/numbing, and hyperarousal. In the current sample, PCL-C obtained proper values of reliability (.91 for total score, .85 for the hyperarousal/re-experiencing subscale, .80 for numbing, and .72 for avoidance subscale). These values were similar to the Spanish version of the PCL-C, which also has a good total score reliability of .90, and coefficients of .87, .78, and .69 for the hyperarousal/re-experiencing, numbing, and avoidance subscores (Costa-Requena & Gil, 2010).
PTG. The Posttraumatic Growth Inventory (PTGI; Tedeschi & Calhoun, 1996) focuses on the assessment of positive changes experienced after trauma. The 21-item PTGI yields a total score and five subscale scores, as follows: new possibilities (5 items), relating to others (7 items), personal strengths (4 items), appreciation of life (3 items), and spirituality (2 items). Items are rated on a 6-point Likert scales, ranging from 0 (did not experience this change) to 5 (experienced this change strongly). In this study, the Spanish version of PTGI was used, showing good reliability index (.91) in our sample, similar to the one obtained by Costa-Requena and Gil (2010) of .95. To assess the authenticity of PTG facilitation we evaluated two interpersonal indicators: “corroborated PTG” and “vicarious PTG” in relatives. A modified version of the PTGI was therefore also given to significant others (86.7% couples, 6.7% brothers, 6.7% sons) to enquiry about their perception of PTG in patients (i.e., corroborated PTG). Significant others were also asked about their own PTG due to the cancer diagnosis of their loved one (i.e., vicarious PTG). The instructions were modified to ask significant others about their own PTG and their opinion of patient's PTG. To ensure that dyads did not discuss PTGI, a pre-paid sealed envelope was sent to significant others. Patients completed the questionnaires in the hospital. In both cases, the instructions explicitly asked informants to fill in questionnaire individually without discussing it with their dyads.
Extreme Life Events. The Extreme Life Events Inventory (Pérez-Sales et al., 2012) collects information about the number and the impact (threat and influence on one's lifetime trajectory) of 34 extreme life experiences, mostly related to trauma, loss, and crisis. Prior to the cancer experience, participants could have had other extreme vital experiences, which could affect the PTG reports before PPC treatment. In this study, the number of prior extreme events that decisively influenced the life trajectory was used to control for the effects of PTG facilitation on stress reduction in the PPC (M = 1.32; SD = 1.29).
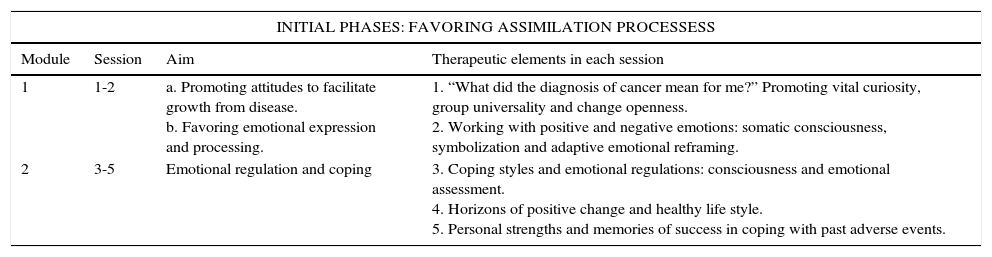
InterventionPPC aimed to facilitate PTG through psychotherapeutic methods that have been associated with the development of positive life changes after cancer (see Table 1). The program consisted of 12 weekly sessions of 90–120minutes in length. Each group comprised 8–12 patients confirmed as being disease-free after completing their primary cancer treatment. Sessions were spread across four modules, each of which had different lengths and aims (see Table 1). The general objective for the first two modules was the assimilation of the cancer experience, while the final two modules focused on encouraging accommodation and personal transformation (growth) from the illness experience. The manualized program and guide is available in Spanish (Ochoa et al., 2010) and English (Ochoa & Casellas-Grau, 2015).
Positive Psychotherapy for cancer description.
| INITIAL PHASES: FAVORING ASSIMILATION PROCESSESS | |||
|---|---|---|---|
| Module | Session | Aim | Therapeutic elements in each session |
| 1 | 1-2 | a. Promoting attitudes to facilitate growth from disease. b. Favoring emotional expression and processing. | 1. “What did the diagnosis of cancer mean for me?” Promoting vital curiosity, group universality and change openness. 2. Working with positive and negative emotions: somatic consciousness, symbolization and adaptive emotional reframing. |
| 2 | 3-5 | Emotional regulation and coping | 3. Coping styles and emotional regulations: consciousness and emotional assessment. 4. Horizons of positive change and healthy life style. 5. Personal strengths and memories of success in coping with past adverse events. |
| INTERMISSION AND FINAL PHASES: FAVORING ACCOMODATION PROCESSES | |||
|---|---|---|---|
| 3 | 6-9 | PTG facilitation | 6. Giving meaning to the experience. Work with recent and remote positive memoirs. 7. Giving meaning to the experience. Personal realization guidelines and hope-based interventions 8. Relational growth: Promoting and awaking interest towards significant others and working with positive models against adversity 9. Relational growth: Gratitude and forgiveness-based interventions. |
| 4 | 10-12 | a. Existential and spiritual aspects b. Group conclusion | 10. Foreseeing recurrence, increase of mortality and transience consciousness, and dealing with emotional anesthesia 11. Transcendence and regret as a constructive way 12. Farewell letter and review of the group experience |
Consecutive participants based on time of recruitment were allocated to the PPC or waiting-list control group depending on the availability of the PPC intervention. When PPC was not available in the short term (more than two weeks), participants were allocated to a waiting list group for three months (the same period as the active PPC treatment). After that, for ethical reasons, they were assigned to receive usual psycho-oncological individual attention (treatment as usual, TAU) without waiting for the 12-month follow-up in the PPC group to finish. Therefore, the waiting-list group assessments were not included as part of the intervention group and the 3- and 12 month time-points were only assessed for the patients who participated in the PPC group. TAU in psycho-oncology departments generally comprises non-systematic individual sessions focused in emotional support and psychoeducation. The four clinical psychologists who conducted the therapy were supervised by two experts in the application of PPC to assess its fidelity to the manual (Ochoa et al., 2010). Treatment integrity (or fidelity) was assessed directly by these two supervisors via monitors or via videotaping randomly and without notifying the therapist, in 25% of the group intervention sessions. We also assessed integrity by measuring therapist adherence as well as competence in an ad-hoc questionnaire adapted and summarized from the Cognitive Therapy Scale Revised (Blackburn et al., 2001). The ad-hoc questionnaire assessed: agenda (sequence of the 4 modules and their tasks), conceptual integration, appropriate positive feedback, application of positive change methods and homework tasks. The two supervisors scored the same groups independently. We calculated interrater supervisor's agreement using the T index, which allows the evaluation of rater agreement along ordinal scales. Agreement was defined as identical scores on an item on a 4-point scale. The overall T index was .89 (Perepletchikova, Treat & Kazdkin, 2007).
Statistical analysisStatistical analysis was performed using IBM SPSS for Windows, Version 21.0 (IBM Corp., Armonk, NY, USA). Differences between participants and non-participants were examined by Student t tests and χ2. Multivariate analyses of variance involving repeated measures were performed on an intention to treat analysis (ITT) basis to analyze changes of the intervention over time. Therefore, analysis of variance were performed to study the psychological changes between groups at T0 and T1 as well as the stability of the effects of the PPC at follow-up, and the reported effect size is partial η2. To examine the corroboration of PTG, intraclass correlation and simple linear regression were used, as appropriate reporting, respectively, ICC and lineal regression coefficients (B), as well as 95% confidence intervals. In addition, to analyze intrapersonal variables of PTG corroboration, simple regression analysis was performed. Finally, predictive analysis was performed to assess the role of PTG facilitation in reducing posttraumatic stress symptoms after PPC, reporting linear regression coefficients (B) and 95% confidence intervals. Statistical significance was assumed at a p <.05.
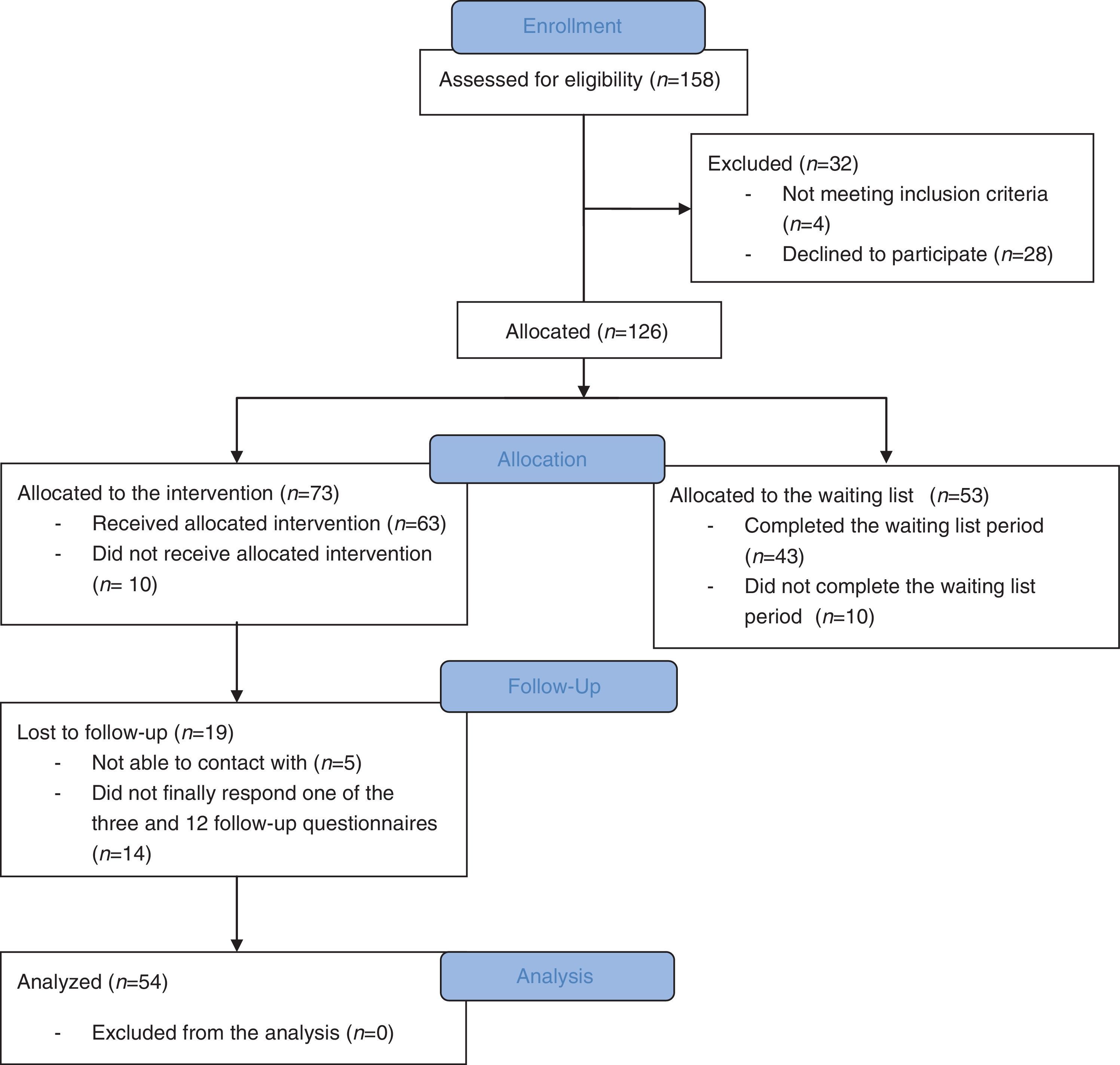
ResultsStudy groupFigure 1 shows a flowchart of the numbers of participants recruited and allocated to each group, followed-up, and analyzed. Of the 158 patients recruited, 28 refused to participate because of health issues (n = 6), lack of time (n = 9), and lack of interest (n = 13). In addition, four women did not meet the inclusion criteria. The remaining 126 subjects were then allocated to either the control group (n = 53) or the PPC group (n = 73).
Sample characteristics
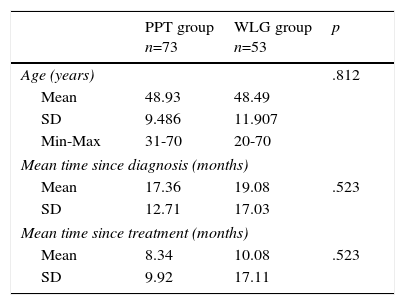
Sociodemographic and medical characteristics are presented in Table 2 for both treatment and control groups. No significant differences were found between groups at baseline (T0), specifically in the PCL, HADS, and PTGI. There were no significant differences between those who declined to participate and those in the control group.
Comparison of samples’ sociodemographical and medical characteristics between PPT and WLG groups.
| PPT group n=73 | WLG group n=53 | p | |
|---|---|---|---|
| Age (years) | .812 | ||
| Mean | 48.93 | 48.49 | |
| SD | 9.486 | 11.907 | |
| Min-Max | 31-70 | 20-70 | |
| Mean time since diagnosis (months) | |||
| Mean | 17.36 | 19.08 | .523 |
| SD | 12.71 | 17.03 | |
| Mean time since treatment (months) | |||
| Mean | 8.34 | 10.08 | .523 |
| SD | 9.92 | 17.11 | |
| PPT group % n=73 | WLG group % n=53 | p | |
|---|---|---|---|
| Marital status | .220 | ||
| Married/partnered | 75.3 | 86.8 | |
| Separated/divorced | 15.2 | 3.8 | |
| Never married | 6.8 | 7.5 | |
| Widowed | 2.7 | 1.9 | |
| Educational level | .615 | ||
| High school or less | 53.4 | 48.1 | |
| Some college | 30.2 | 38.5 | |
| University studies | 16.4 | 13.4 | |
| Working status | .783 | ||
| Employed | 11.0 | 13.2 | |
| Unemployed | 89.0 | 86.8 | |
| Children | .977 | ||
| Yes | 79.5 | 79.2 | |
| No | 20.5 | 20.8 | |
| Cancer site | .340 | ||
| Breast | 83.6 | 96.2 | |
| Uterine corpus | 4.1 | .00 | |
| Hodgkins lymphoma | 1.4 | 1.9 | |
| Non-hodgkins lymphoma | 1.4 | 1.9 | |
| Colon | 2.7 | .00 | |
| Myelogeneous leukemia | 2.7 | .00 | |
| Ovary/Fallopian tube | 2.7 | .00 | |
| Rectum | 1.4 | .00 | |
| Psychotropic medication | .872 | ||
| None | 53.4 | 64.2 | |
| Anxiolytic | 26.0 | 7.5 | |
| Antidepressant | 5.5 | 11.3 | |
| Anxiolytic+Antidepressant | 11.0 | 13.2 | |
| Hypnotic | 4.1 | 3.8 | |
| Cancer stage | .731 | ||
| 0 | 2.9 | .00 | |
| I | 40.6 | 45.3 | |
| II | 34.8 | 30.2 | |
| III | 17.4 | 18.8 | |
| IV | 4.3 | 5.7 | |
| Cancer surgery | .520 | ||
| Yes | 89.0 | 92.5 | |
| No | 11.0 | 7.5 | |
| Cancer treatment | |||
| Chemotherapy | 79.5 | 79.2 | .977 |
| Radiotherapy | 72.6 | 84.9 | .101 |
Note. Between-groups characteristics were compared using chi square-based tests, except for age, time since diagnosis, and treatment differences which were analyzed using t-tests.
A two-way mixed multivariate analysis of variance was performed on an ITT basis. Missing responses from 9 (14.2%) participants in PPC group and 10 (18.8%) participants in WL group were imputed as the last observation carried forward. Results revealed a statistically significant interaction between group (PPC vs waiting list) and time (T0 vs T1), F(5,83) = 5.44, p <.001, partial η2 = .25. Specifically, compared to the waiting list group, the strongest reduction of PCL and HADS scores in the PPC group indicate less negative mood and stress in T1 among those participants receiving PPC compared to those in the waiting list. The effect size value of the partial η2, suggest that the PPC program contributes remarkably to a positive psychological functioning. On the other hand, although PPC group showed greater increases than the WL group in PTGI pre-post scores, no statistically significant interactions were detected in any of its subscales.
In much the same way, univariate tests also indicated statistically significant interactions between group and time on every PCL subscale (Intrusions, F(1,87) = 8.16, p =.005, partial η2 = .09; Avoidance, F(1,87) = 11.46, p =.001, partial η2 = .12; Hyperarousal, F(1,87) = 17.78, p <.001, partial η2 = .17) and every HADS subscale (Anxiety, F(1,87) = 11.49, p =.001, partial η2 = .12; Depression, F(1,87) = 12.07, p =.001, partial η2 = .12).
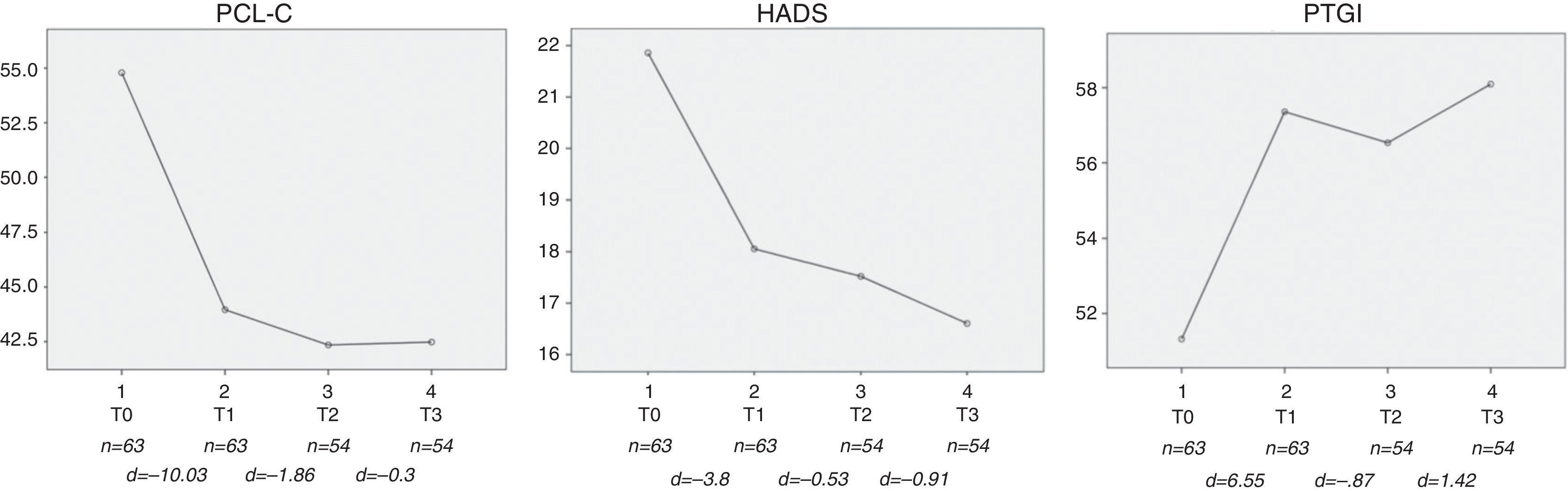
Stability of the effects of the PPC at follow-upIn order to study the evolution of the positive functioning in those participants allocated to PPC program, multivariate repeated measures analysis of variance of the total PCL, HADS and PTGI scores was performed on an ITT basis. Missing responses from 9 (14.2%) participants in PPC group and 10 (18.8%) were imputed as the last observation carried forward. The observed multivariate F test value was statistically significant, F(9,62) = 10.49, p <.001, partial η2 =.60. The univariate tests showed a significant variation over time of the scores of PCL, F(3,210) = 38.04, p <.001, partial η2 =.35; HADS, F(3,210) = 17.92, p <.001, partial η2 =.20; and PTGI, F(3,210) = 6.31, p =.001, partial η2 =.08 in line with the expected contribution to the positive psychological functioning, that is, PCL and HADS scores decreasing over time, and PTGI scores increasing (see Figure 2).
, post-intervention (T1), 3 months follow-up (T2), and 12 months follow-up (T3). d= between-stage differences. PCL-C: posttraumatic stress; HADS: mood; PTGI: positivechanges experienced after trauma.")
Contrasts showed a statistically significant lineal component for PCL, F(1,70) = 62.47, p <.001, HADS, F(1,70) = 44.21, p <.001, and PTGI, F(1,70) = 9.56, p =.003. Interestingly, a quadratic component was also significant for PCL, F(1,70) = 28.39, p <.001, for HADS, F(1,70) = 4.61, p =.036, and for PTGI, F(1,70) = 3.95, p = .050, which according to Figure 2 suggest a major change from pre-intervention (T0) to post-intervention (T1), and a stabilization of the scores on the follow-up (T1 to T3).
Authenticity of PTG facilitationResults from the intraclass correlation (ICC) index indicated agreement between patient's and caregiver's PTGI results (ICC = .663; 95% CI = .481–.782; p <.001), corroborating that PTG occurred in the patient. After the PPC program, the ICC even increased slightly (ICC = .712; 95% CI = .459–.846; p <.001). Linear regression showed that before the PPC program, there was a significant relationship between the PTGI scores of significant others and patients (B = .33; p = .042; 95% CI = .12–.65). However, the relationship became statistically not significant (B = .28; p = .115; 95% CI = –.07–.64) after completing the PPC program, with patients reporting higher PTGI scores than significant others. Therefore, the influence of a patient's PTG on their partners’ PTG was only significant before the PPC program.
Predictive role of PTG facilitation on post-traumatic stress reduction after PPCPTG facilitation was calculated using the increase of PTGI (pre-post PPC treatment). The predictive role of PTG facilitation on stress reduction after the PPC was explored through a linear regression predictive analysis, which resulted in .25 (95% CI = .10–.41; p = .052) when controlling for the number of prior extreme threatening life events reported by each individual.
DiscussionA high rate (50%–90%) of those who have experienced oncological disease report positive life changes (e.g. PTG), even without psychological intervention (Sawyer et al., 2010; Sumalla et al., 2009). Although these positive life changes are associated with better adjustment to disease (Helgeson et al., 2006; Morrill et al., 2006; Sawyer et al., 2010), the power of psychological treatment to facilitate PTG and increase the potential better adjustment to illness by reducing emotional distress or posttraumatic stress (Roepke, 2014) is poorly understood. Cognitive-behavioral stress management (Antoni, 2003) was the first therapy which has shown the potential of psychological therapies to promote growth in cancer patients measured with a cancer-specific benefit-finding inventory (Antoni et al., 2006; Penedo et al., 2006). However, this therapy was designed to focus on and target stress management, which only increases growth as a side effect. In this present study, our primary aim was therefore to test the hypothesis whether PPC, that was specifically designed to facilitate PTG in patients with cancer, could promote stress reduction.
Our results showed that PTG could be facilitated by the PPC program, and that increases in PTG were associated with decreases in emotional distress and posttraumatic stress. PPC group compared with WL group showed an increase in PTG from pre-intervention (T0) to post-intervention (T1), that was maintained at 3 and 12 months of follow-up, but this increase was not statistically significant. However, PTG facilitation predicted a decrease in posttraumatic stress after the PPC, when controlling for the number of prior extreme threatening vital events.
With regard to the evolution of PCL and HADS scores, results suggested a major change from pre-intervention (T0) to post-intervention (T1), and a stabilization of the scores on the follow-up (T1 to T3). A meta-analysis (Helgeson et al., 2006), clarified the relationship between stress and growth, observing that high levels of growth and emotional distress could coexist in the initial phases of cancer, but that growth was associated with a decrease in emotional distress in later phases of survivorship. After acute treatment, it seems that PTG results from an accommodation to the oncological experience, and that this has a therapeutic value through the associated stress reduction, as show our results.
Those psychological therapies that focus on stress management have shown the greatest therapeutic impact on distressed patients who are immersed in coping with the initial cancer stressors of diagnosis and treatment (Antoni, 2003; Penedo et al., 2006). However, our results suggest that facilitating PTG through the PPC program could be suitable for stress reduction in patients who show high levels of stress or distress after completing oncological treatment. The facilitation of PTG in these situations could serve as a way of providing meaning, of processing distress, and trying to accommodate prior views to disturbing disease-related questioning. Reliably, psychological treatments in cancer may need to be time-oriented. In the initial phases, during diagnose and primary oncological treatments, could be suitable stress management therapies more focused in managing the threat of initial stressors (surgical intervention, chemotherapy and radiotherapy). After primary oncological treatments, it could be more suitable a PTG facilitation therapy, where patients begins to accommodate the experience and are open to consider vital changes. In fact, there is an association between high levels of posttraumatic stress and loss of quality of life in cancer survivor patients (Haberkorn et al., 2013), which could be buffered by PTG (Morrill et al., 2006) after oncological treatments.
We also aimed to assess the authenticity of PTG induced by the PPC program. We found that PTG in patients was corroborated by their significant others before and after PPC, with pre-treatment correlations similar to those obtained in comparable studies (Moore et al., 2011; Shakespeare-Finch & Barrington, 2012). However, this is probably the first study in which significant others also corroborated the induced PTG after psychological treatment, thereby strengthening the correlation between self-reported and corroborated PTG and providing relational authenticity to the results.
On the other hand, when comparing PTG between patients and significant others seems that the increase in PTG observed among cancer patients after the PPC program does not explain the changes in PTG among significant others, even when significant others could perceive and corroborate the patients’ PTG. These results can be understood given the lack of psychological treatment offered to significant others. As some studies show, the PTG induced during cancer diagnosis and treatment can generate positive change and PTG in significant others. However, this probably only occurs through vicarious growth, when they get involved in the initial emotional impact and the patient's needs (Ochoa et al., 2013); this would be more difficult during survivorship where we run PPC. Indeed, many survivors have commented on this lack of attention, empathy, and harmony after oncological treatment: “they (significant others) believe that everything is fine now (after treatment), but I do not feel like that” (Ochoa et al., 2010). Therefore, when significant others do not receive any psychological treatment and do not perceive the ongoing threat that remains in cancer survivors, vicarious growth could be prevented from emerging in them after the PPC. This hypothesis that significant others need to participate in psychological treatment to facilitate PTG was reinforced in a recent study (Heinrichs et al., 2011), in which the authors used couples, group-based psychological treatment for cancer survivors and their partners. They showed that PTG increased in both partners and cancer survivors after treatment.
The findings from the current study should be evaluated in the context of the study's methodological limitations. First, the control group was not ideal because, besides the ethical problem of waiting for treatment, the expectation of waiting could have influenced the results. Moreover, the waiting-list group only went three months without follow-up and it would have been preferable compared PPC with traditional active treatments with empirical support. The main limitation of this study is the absence of a randomized assignation of participants to study conditions. So, although PPC appears to promote long term PTG, its efficacy requires validation with a randomized control group with longer follow-ups. Finally, as it happens in multicomponent psychological treatment programs, in our study it is not possible to discern which elements of the program are those with greater or less psychotherapeutic impact.
In summary, this study has shown the positive effects of facilitating PTG among cancer survivors through a PPC program compared with a control group. To our knowledge, this is the first study to show that a treatment focused on PTG could achieve significant and maintained reductions in both posttraumatic stress and emotional distress. The facilitation of PTG seems to be optimal in reducing distress and stress reactions over time in cancer survivors. This facilitation is corroborated by significant others.
FundingThis manuscript was supported by grants from Instituto de Salud Carlos III (FIS PI15/01278) and confunded by FEDER funds/ European Regional Development Fund (ERDF)- a way to build Europe-” // FONDOS FEDER “una manera de hacer Europa”.
Grup de recerca consolidat: Recerca en serveis sanitaris en càncer. 2014SGR0635
