



This study was designed with a dual goal: (1) to compare the change in the scores of depressive symptoms by means of the implementation of three intervention programs in comparison to a control group: a) based on Epstein's TARGET (ET), b) without TARGET strategies (NET), and c) under conditions of active exercise (AE); and (2) to analyze whether the Self-determination Index (SDI) predicts the reduction of depressive symptoms. The participants (N=106; 68 females and 38 males), aged between 18-30 years, were randomly assigned to one of the groups. Each treatment lasted 8 weeks (3hours/week). Of the ET participants, 59.26% showed a therapeutic response, defined as a 50% reduction in the reference score, versus 25.93% for the NET, 19.23% for the AE, and 3.84% for the control group. After six months, the ET group increased their percentage of therapeutic response by slightly more than 10%, which did not occur in the other groups. SDI predicted lower levels of depressive symptoms, and our findings indicate that TARGET strategies can have a direct effect on depressive symptoms at the time of intervention and an indirect effect at a later stage due to their impact on future levels of physical activity.
Este estudio fue diseñado con doble objetivo: (1) comparar el cambio de las puntuaciones de síntomas depresivos mediante la implementación de tres programas de intervención: a) basado en el TARGET de Epstein (ET), b) sin estrategias del TARGET (NET) y c) bajo condiciones de ejercicio activo (AE), así como, d) un grupo-control; y (2) analizar si el Índice de Autodeterminación (SDI) predice la reducción de síntomas depresivos. Los participantes (N=106; 68 mujeres y 38 varones), con edades entre 18-30 años, fueron asignados al azar a uno de los grupos. Cada tratamiento duró 8 semanas (3 horas/semana). El 59,26% de los participantes en el grupo ET tuvo una respuesta terapéutica, definida como una reducción del 50% en la puntuación de referencia, frente al 25,93%, 19,23% y 3,84% para los grupos NET, AE y control, respectivamente. Seis meses después, el grupo ET aumentó el porcentaje de respuesta terapéutica más del 10%, lo que no ocurrió en los otros grupos. El SDI predijo niveles más bajos de síntomas depresivos. Las estrategias del TARGET pueden tener un efecto directo sobre los síntomas depresivos durante la intervención y un efecto indirecto posterior debido a su impacto sobre los niveles futuros de actividad física.
Depression is an all too frequent mental disorder, with more than 350 million people of all ages suffering from this disorder and predictions indicating that it will become the second leading cause of disability worldwide by 2020 (World Health Organization [WHO], 2012). Although there is evidence to support the clinical efficacy of approaches such as pharmacological, somatic and/or psychological treatments for treating depression, these approaches have several limitations (Pérez-Wehbe, Perestelo-Pérez, Bethencourt-Pérez, Cuéllar-Pompa, & Peñate-Castro, 2014). An alternative approach to treating mental health disorders is physical activity (PA) and exercise. Although the quantity of PA varies between the studies reviewed, the evidence suggests that even low doses of PA can protect against depression (e.g., Bauman et al., 2012; Josefsson, Lindwall, & Archer, 2014; Teychenne, Ball, & Salmon, 2008). Most of the interventions have focused on various types of aerobic PA, such as cycling, running or walking, but other forms of PA (such as training with weights, yoga, or stretches) have been less explored (Mammen & Faulkner, 2013). However, no widely-acknowledged evidence is available which endorses specific PA programs that are effective against depression (Pomp, Fleig, Schwarzer, & Lippke, 2013). Moreover, only a few studies have analyzed the association between depressive symptoms and the type of PA within social contexts, such as participation in team sports (Sabiston et al., 2013), and no study that we are aware of has yet explored the effect of interactions with the teacher and/or with classmates in PA therapy sessions.
Analysis of the influence of the social relations that are generated (or can be generated) in PA upon depressive symptoms is of great relevance, because common symptoms of depression include isolation and avoidance of social interaction-related activities (Seime & Vickers, 2006). Another symptom of depression is a lack of motivation to undertake activities that previously gave pleasure. For this reason, recent research highlights the possible beneficial role of the theory of motivation in order to expand, inform and enrich therapeutic approaches and interventions in clinical practice (McBride et al., 2010). A new analytical factor, ‘autonomous motivation for therapy’ (defined as the degree to which patients experience participation in therapy as a freely chosen option), has also become known as another powerful factor which can predict treatment outcome (Patrick & Williams, 2012).
Within this context, the self-determination theory (SDT) has emerged as a relevant contemporary approach to the design of interventions and PA programs and to better understand the processes leading to sustained motivation. A sub-theory within the SDT framework, ‘the theory of basic needs’ (Deci & Ryan, 2000), argues that satisfaction of the basic psychological needs of competence, autonomy and relatedness promotes greater autonomous motivation, which in turn leads to more positive outcomes. Indeed, there is considerable evidence of the impact of autonomous motivation on participation in PA (Teixeira, Carraça, Markland, Silva, & Ryan, 2012), as well as on changing health-related behaviors (Ng et al., 2012). From the viewpoint of the theory of basic needs, contextual factors are considered critical to promote the processes and outcomes of motivation. In particular, it is assumed that positive interactions with significant others (which tend to promote and support greater autonomy and satisfaction with social-relationships, thus increasing the perception of self-competence) should have a positive and healthy effect on people (Ng et al., 2012). In a recent study, Duda et al. (2014) compared two interventions to promote exercise: 1) a standard provision; and 2) an SDT-based intervention (autonomy support), showed that changes in self-determined motivation were negatively associated with depressive symptoms.
The incidence of contextual factors in sports (more specifically, Epstein's TARGET strategies) (Epstein, 1988) on the psychological mediators, such as types of motivation and behavioral consequences, have recently been evaluated by Cecchini, Fernandez-Río, Méndez-Giménez, Cecchini and Martins (2014). The results showed that contextual factors had a significant effect on an athlete's psychological need for self-satisfaction, self-determined motivation, as well as persistence and effort. Another study also analyzed the impact of Epstein's TARGET on PA in adolescents (Cecchini, Fernandez-Rio, & Méndez-Giménez, 2014), and the findings supported the efficacy of increasing an adolescent's intent to perform PA, as well as the time dedicated to PA in their free time.
With respect to the above findings, it is likely that the motivational climate constructed by the teacher (or ‘coach’) in PA sessions can also have a beneficial effect on participants’ depressive symptoms. In fact, the manner in which motivation is offered affects the way in which people pursue physical health goals (Gallagher et al., 2012). The term TARGET (Epstein, 1988) is an acronym for: Task (design of activities); Authority (location of decision-making); Recognition (way of distributing rewards, such as praise); Grouping (selection criteria of the workgroups); Evaluation (performance standards that are considered important); and Time (learning rhythm). Various investigations have analyzed the effects of TARGET on athletes and physical education students’ attitudes, knowledge, and behaviors (e.g. Braithwaite, Spray, & Warburton, 2011), and some of these studies have related motivational climate to anxiety (Cecchini et al., 2001).
Accordingly, to determine the importance of motivational climate, we compared the results of an intervention based on Epstein's TARGET with those obtained using other types of PA. Using the scores of depressive symptoms as an outcome measure (Choi, Patten, Gillin, Kaplan, & Pierce, 1997), the goals of the present study were the following: 1) to verify whether a PA intervention program based on Epstein's TARGET strategies (ET) generates a significantly higher reduction in depressive symptoms scores than a PA intervention program without implementing the TARGET strategies (NET), or than individual physical exercise (AE), as well as placebo physical exercise; and 2) to determine whether SDI predicts a significant reduction of depressive symptoms. If this is so, it could be a relevant finding with respect to addressing and reducing depressive symptoms, as it would not only confirm the importance of performing PA, but also, it would especially show that doing PA in a motivationally suitable context is crucial.
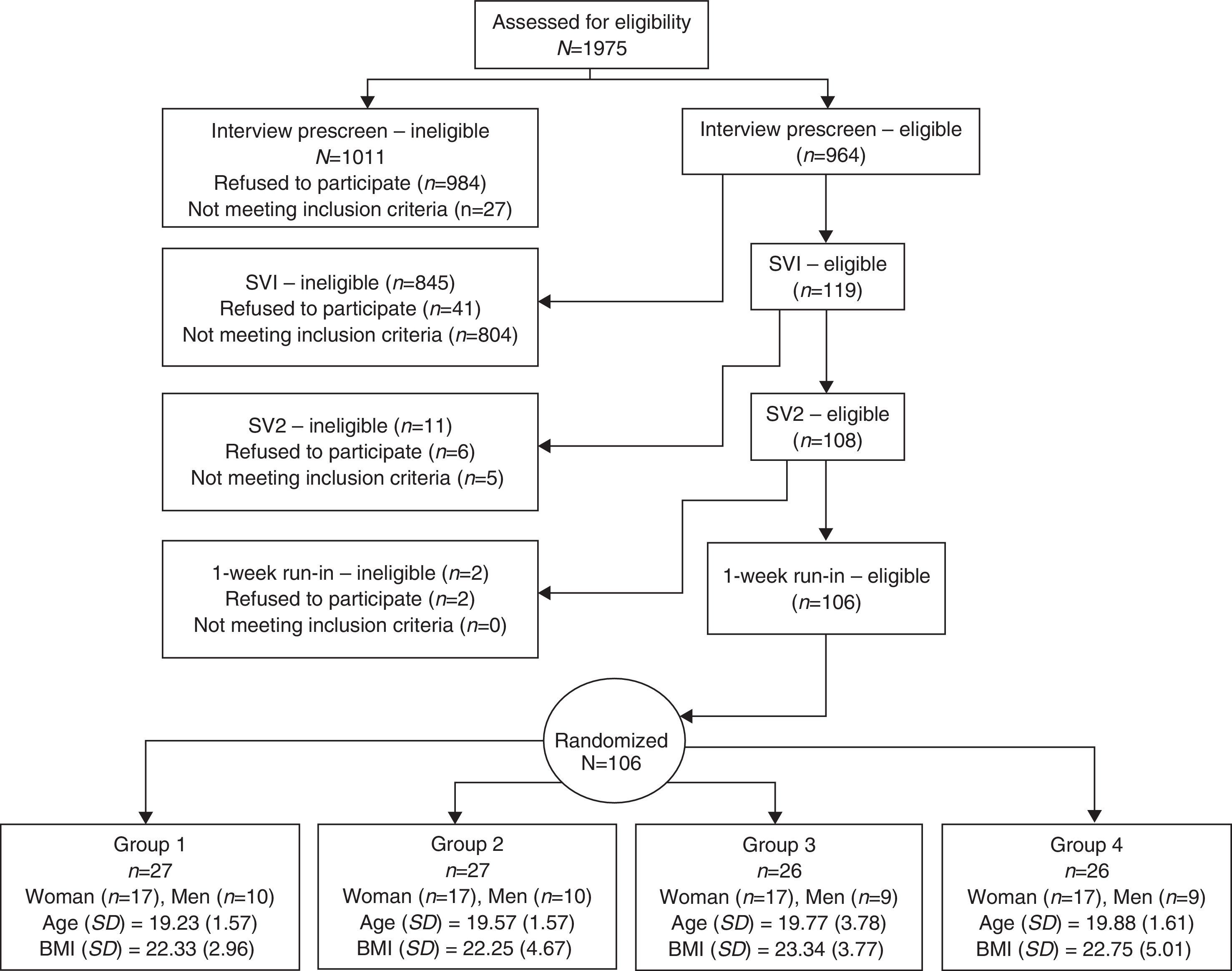
MethodParticipantsThe study's participants were drawn from a cohort of university students from a city in northern Spain. After a selection process beginning with preliminary interviews of 1,975 college students (1,179 women and 796 men), the final sample was made up of 106 subjects (68 females and 38 males) aged between 18 and 30 years, each of whom had scored between 29 and 34 on the adapted self-report depression scale established by Kandel and Davies (1982).
Participants with a score of 29 or higher on this scale were classified as having significant depressive symptoms (Choi et al., 1997). Other inclusion criteria were: (a) being sedentary (defined as vigorous exercise less than three times per week for at least 20minutes a day); (b) not receiving any treatment for depression; and (c) giving their written informed consent. The exclusion criteria were the following: (a) consumption of more than 21 alcoholic beverages per week, (b) hospitalization for a psychiatric disorder in the past 5 years, (c) current participation in other clinical trials, (d) drug use, (e) inability to participate due to medical prescription, and (f) for the females, planned or current pregnancy.
Selection processParticipants were selected by means of a prior interview and two screening visits (SV1, SV2). The preliminary interviews were administered by the authors, with the aim of recruiting a wide-enough sample size for the study. Prospective participants were informed of the types of activities to be carried out upon being accepted to take part in the study, the exclusion criteria, and the potential benefits with respect to participation (including credits granting). Screening visits were intended to assess depressive symptoms and sedentariness (SV1), and to verify that they could perform physical exercise safely (SV2). After SV2, 108 participants were selected assessment of their capacity to adhere to regular physical exercise (1-week), and also to assess their self-determined motivation (Figure 1). This process lasted for six months. A restricted randomization design was used, which was based on three blocks (gender, age, and BMI) aimed at reaching a balance between group-size and other physical characteristics. The participants gave their written informed consent, and the study was conducted in accordance with The Helsinki Declaration of the World Medical Association (2008), with final approval for the study obtained from the Ethical Committee of the University.
Instruments
Depressive symptoms. An adaptation of the six-item self-report scale defined by Kandel and Davies (1982) was used in the present study. This scale assesses six depressive symptoms experienced during the past 12 months (Choi et al., 1997). The responses to the items are added, providing a depressive symptomatology score ranging from 6 to 24 points. These scores were adapted by 10 points to produce a new range between 16 and 34 points (Choi et al., 1997). Response to treatment is defined as a reduction of depressive symptoms in general by at least 50% of the initial scores on the depressive mood scale (Brunoni, Lopes, Kaptchuk, & Fregni, 2009). The Cronbach alpha obtained was .72. While there are more powerful assessment tools to evaluate this component, given its psychometric properties and the fact that the depression scale administered offers a brief and general detection measure, this instrument was chosen for two key reasons: a) it allows identification of participants with depression symptoms easily; b) it has been used in previous studies which were also focused on the relationship between physical activity and depressive symptoms, thus making it possible to carry out additional broad-scoped comparisons (e.g., Sabiston et al., 2013).
Self-determined motivation. The Situational Motivation Scale (SIMS), as defined by Guay, Vallerand and Blanchard (2000), is a measure of situational (or state) motivation towards a chosen activity. This self-report inventory consists of four items for each subscale and was designed to measure intrinsic motivation, identified regulation, external regulation, and amotivation. Participants respond to the stem, “Why are you currently involved in this activity?” Each item is rated on a 7-point Likert scale, ranging from 1 (not at all in agreement) to 7 (completely in agreement). As the subscales of the SIMS assess types of motivation on a self-determination continuum, a self-determination index (SDI) can be calculated. In this study, SDI is computed by multiplying the score of each SIMS subscale by a factor that represents its position on the construct of the self-determination continuum: SDI=2 * intrinsic motivation+identified regulation - external regulation - 2 * amotivation) (Guay et al., 2000). The following Cronbach alphas were obtained: intrinsic motivation=.94; identified regulation=.88; external regulation=.78; and amotivation=.78.
Physical activity. The International Physical Activity Questionnaire (IPAQ) was developed as an instrument for cross-national control of PA and physical inactivity. The IPAQ has reasonable measurement properties for screening the population levels of PA between ages 18-65 years in diverse settings (Craig et al., 2003). In the present study, we used the short version, which provides information about time spent on moderate to vigorous physical activity (MVPA). The MVPA indicator is expressed in metabolic equivalents (METs) - minutes/week of MVPA (i.e. METs-MVPA). The IPAQ has reasonable properties to control the levels of PA. The IPAQ in Spanish was obtained from the website: www.ipaq.ki.se.
DesignWe used an experimental design in which participants were randomly divided into four groups (ET, NET, AE, & Control). The authors of the present manuscript selected participants and assigned the sample randomization sequence, which was implemented by way of sequentially numbered opaque sealed envelopes. The four groups were independent, and each individual group was prevented from knowing the existence of the remaining groups. For this purpose, intervention was carried out on different days. All groups were equivalent, thus they did not show statistically significant differences in age, gender or BMI (Figure 1).
For 8 weeks (24 one-hour sessions), Group ET engaged in an intervention program based on Epstein's TARGET strategies taught by a physical education teacher trained to that effect. During the same time interval, Group NET carried out their usual programmed training sessions without implementing Epstein's TARGET strategies. Also during the above time frame, Group AE carried out the same scheduled PA sessions, but without the intervention of a physical education teacher. Lastly, the control group carried out placebo physical exercise, defined as 3 days a week of stretching and flexibility exercises for 60minutes per session. The participants were randomly assigned to the experimental groups or control placebo exercise group. In this sense, the absence of attrition rates is explained by a study-credit awarded to students for their participation, and adherence of the participants motivated by benefits program.
ProcedureThe intervention program designed for the ET experimental group was adapted from the model developed by successive authors (Cecchini et al., 2001; Duda & Balaguer, 2007) to generate a task-involving motivational climate within the six TARGET dimensions described below:
Task. The instructor used open or predominantly perceptive tasks that were presented globally, in the form of problem-situations. At all times, teachers attempted to provoke interest in PA, using varied, amusing, and motivating proposals.
Authority. The instructor took into account the university students’ interests, and the students participated actively in the decisions. This type of learning is largely determined by the student's perception of causative locus, choice, and free will.
Reward. Individual progress was rewarded or recognized by the instructor. They made sure that all the subjects were treated equally, regardless of their initial level, and that they all had the same expectations in relation to personal success.
Groupings. Small, cooperative, flexible, and heterogeneous groups were established. Learning, personal improvement, teamwork, and a class climate promoting positive social interactions were encouraged.
Assessment. The achievement of individual and collective goals was evaluated as a function of personal improvement criteria.
Time. Lastly, the students were allowed to participate in the decision-making process related to learning rhythm and the time assigned to each task.
Two teachers supervised the ET and NET groups in this study, however, the AE and placebo groups did not require teacher-participation. Each teacher was randomly assigned to either the ET or NET experimental group (Montero & León, 2007), and each one remained with their assigned group. The participant instructors had at least 5 years of prior teaching experience and also agreed to attend a specific seminar to train in TARGET strategies before starting the implementation phase. The seminar consisted of 20hours of theory and 10hours of practical training, and included pre-designed lessons, which were subsequently analyzed and discussed. While carrying out the intervention program, the instructor had to attend a weekly meeting with the research group. One teaching session from each participant group was recorded each week in order to check the fidelity of the process. For this purpose, a list of interventions coded for each group was established. Researchers and teachers did the coding independently of each other. Recordings were checked by the research group in order to guarantee that the sessions proceeded according to the established program. Ultimately, a combination of training seminars, pre-designed sessions, and analysis of videos to provide adequate training was used (Braithwaite et al., 2011). In addition, the progression of the experiment was closely monitored by the study's chief investigators.
Data analysisAll the data were analyzed using the SPSS 19.0 program (IBM, Chicago, IL). In all three experimental groups, PA was of moderate-to-vigorous intensity and was monitored by the research group in each and every session so that it would be adequately balanced (e.g. schedules and development of the sessions). For this purpose, the activities were classified as a function of their intensity, and this was multiplied by the duration of the activity. Student's t-tests and paired t-tests were used. Hedges’ g was selected as a measure of the effect size to provide an estimation of the effect due to the size of the samples. The calculations of the power of the sample size were based on G * Power, 3.1. In the analysis of clinical efficacy, the assessment of the effects of the treatment on depressive symptom scores and SDI was based on generalized estimation equations (GEEs) for repeated measures. The model was adjusted to allow for participants’ age, gender, and body mass index (BMI). In the six months between post-test 1 and post-test 2, the participants were allowed to practice PA in their spare time if they wished to. Participants were classified in two groups: (A) those who performed PA, at least moderately, following the criteria established in the International Physical Activity Questionnaire (IPAQ); and (B) those who had not met the minimal criteria of moderate PA. Assessment of the effects on the depressive symptom scores (post-2) and SDI was based on GEEs for repeated measures.
None of the questionnaires had more than 8% missing data, so none were eliminated; 10 questionnaires had less than 8% missing data and were therefore randomly imputed with values derived from a multiple regression in which the scores of three items from the same series of indicators (that is, the items that measure the same construct) were used as predictor variables (Byrne, 2008).
ResultsPreliminary analysesOf the 1975 preselected participants, 5.36% were randomly assigned to the treatment. All those who began treatment finished it and attended at least 22 sessions (91.7% of the total treatment). Most of the randomly assigned participants were female (64.16%). Before the intervention, no significant pretest group differences were observed in depressive symptoms (p=.98) or in the SDI (p=.16).
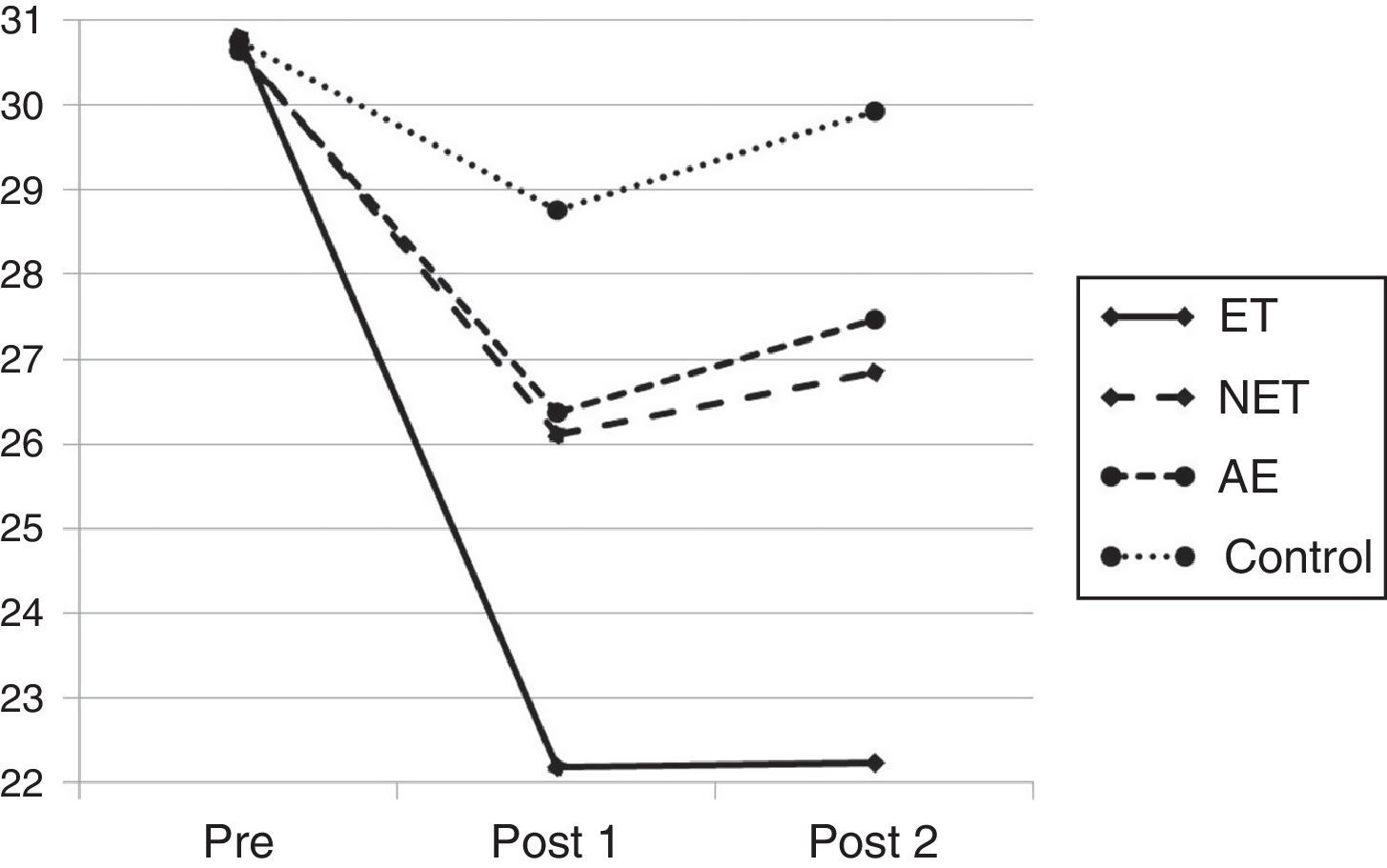
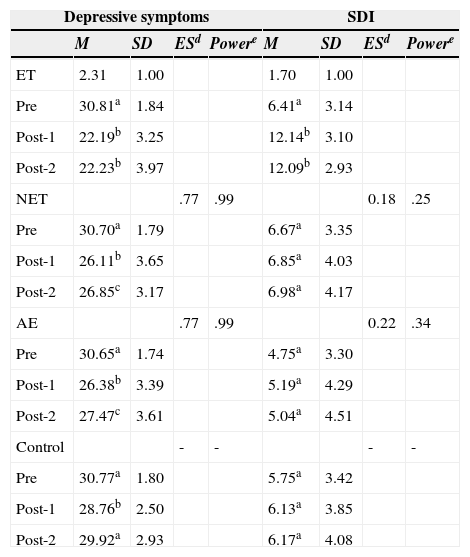
Pre-post intervention differencesSignificant improvements in depressive symptoms were observed between pre-test and post-test 1 in all the groups (ET, NET, and AE, p<.001; control, p<.01) and between pre and post-2 in the experimental groups (ET, NET, and AE, p<.001; control, p>0.1). In the ET group, significant changes were also observed in the SDI between pre-post-1 and pre-post-2 (p<.001). In addition, no significant differences between post-1 and post-2 were observed in the ET group, but they were found in the remaining groups (Table 1).
Means, standard deviation, effect size and sample size power in the pre, post-1 and post-2 phases for the three treatment groups and the control group.
| Depressive symptoms | SDI | |||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | ESd | Powere | M | SD | ESd | Powere | |
| ET | 2.31 | 1.00 | 1.70 | 1.00 | ||||
| Pre | 30.81a | 1.84 | 6.41a | 3.14 | ||||
| Post-1 | 22.19b | 3.25 | 12.14b | 3.10 | ||||
| Post-2 | 22.23b | 3.97 | 12.09b | 2.93 | ||||
| NET | .77 | .99 | 0.18 | .25 | ||||
| Pre | 30.70a | 1.79 | 6.67a | 3.35 | ||||
| Post-1 | 26.11b | 3.65 | 6.85a | 4.03 | ||||
| Post-2 | 26.85c | 3.17 | 6.98a | 4.17 | ||||
| AE | .77 | .99 | 0.22 | .34 | ||||
| Pre | 30.65a | 1.74 | 4.75a | 3.30 | ||||
| Post-1 | 26.38b | 3.39 | 5.19a | 4.29 | ||||
| Post-2 | 27.47c | 3.61 | 5.04a | 4.51 | ||||
| Control | - | - | - | - | ||||
| Pre | 30.77a | 1.80 | 5.75a | 3.42 | ||||
| Post-1 | 28.76b | 2.50 | 6.13a | 3.85 | ||||
| Post-2 | 29.92a | 2.93 | 6.17a | 4.08 | ||||
Note: ET=TARGET-based intervention program, NET=intervention program without implementation of TARGET strategies, AE=program under conditions of active exercise.
abcp<.05
dES, Hedges g was selected as the measure of effect size to provide an estimate of effect due to sample sizes.
dPower, Sample size power calculations are based on G*Power 3.1.
Likewise, statistically significant differences were observed in depressive symptoms at post-1 and post-2 between the ET group and the rest of the groups (p<.001). All groups showed reductions in symptoms during the 8 weeks of treatment. Six months later (at Post-2), only the ET group remained stable (Figure 2). No significant differences were observed between the NET and AE groups either at post-1 (p=.78) or at post-2 (p=.52), but differences were found between these two groups and the control group, both at post-1 (NET, p<.01; AE, p<.01), and at post-2 (NET, p<.01; AE, p<.05). Regarding the SDI, significant differences were observed at post-1 and post-2 between the ET groups and the rest of the groups (p<.001). No significant differences were observed between the rest of the groups either at post-1 or at post-2 (Table 1).
Analysis of clinical efficacy
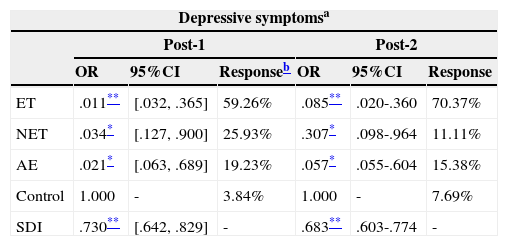
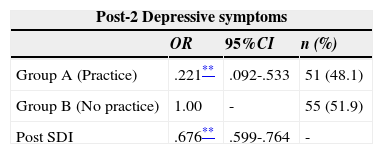
Table 2 shows the GEE for repeated measures at post-1 and post-2 in depressive symptoms. More than 59% of the ET group showed at least a 50% reduction of their initial score at the beginning of the study, and their response to treatment had improved by a further 10% six months later. The responses of the NET and AE groups were similar to each other. The SDI predicted depressive symptoms (post-1 and post-2). Age (post-1, p=.99, post-2, p=.74), gender (post-1, p=.94, post-2, p=.10), and BMI (post-1, p=.26, post-2, p=.12) were not significant.
Z analysis-scores at 8 weeks (Post 1) and six months later (Post 2).
| Depressive symptomsa | ||||||
|---|---|---|---|---|---|---|
| Post-1 | Post-2 | |||||
| OR | 95%CI | Responseb | OR | 95%CI | Response | |
| ET | .011** | [.032, .365] | 59.26% | .085** | .020-.360 | 70.37% |
| NET | .034* | [.127, .900] | 25.93% | .307* | .098-.964 | 11.11% |
| AE | .021* | [.063, .689] | 19.23% | .057* | .055-.604 | 15.38% |
| Control | 1.000 | - | 3.84% | 1.000 | - | 7.69% |
| SDI | .730** | [.642, .829] | - | .683** | .603-.774 | - |
Note: ET=TARGET-based intervention program, NET=intervention program without implementation of TARGET strategies, AE=program under conditions of active exercise.
As shown in Table 3, participants who practiced moderate to vigorous PA (post-2) were less prone to have depressive symptoms than those who did not. Most of these participants belonged to the ET group (n=17), followed by the NET group (n=13), AE (n=12), and control (n=9), p<.001. The SDI also predicted lower levels of depressive symptoms. Age (p=.65), gender (p=.57) and BMI (p=.06) were not significant.
Discussion/conclusionsThe main finding of this study is that the positive effects of PA on depressive symptoms can increase in incidence significantly if PA takes place in a suitable motivational context. Firstly, it was observed that the intervention program based on Epstein's TARGET strategies (Epstein, 1988) is an efficacious treatment for university students who have notable depressive symptoms. Fifty-nine percent of the participants in the ET treatment conditions showed a therapeutic response to the treatment [defined as a 50% reduction of the baseline score of depressive symptoms (post-1)]. Secondly, in prior studies reporting a significant effect of PA on depression or on depressive symptoms, the effect sizes have ranged from .05 to 1.75 (Teychenne et al., 2008). Thus, the present intervention program (based upon Epstein's TARGET strategies - applied by a physical education teacher) showed a comparatively very high effect size (1.70), which was far higher than in the NET and AE treatments.
Statistically significant differences were also observed in the SDI between the ET treatment group and the other groups. This is consistent with previous research that has examined the effects of TARGET on the SDI in other contexts (Cecchini, Fernandez-Río, & Méndez-Giménez, 2014). For the past 15 years, a growing body of research testing the applicability of the SDT in health contexts has emerged (Patrick & Williams, 2012). Globally, the results of these studies have shown the necessary role of support and autonomous self-regulation in a variety of physical and mental health outcomes, such as depression (Ryan, Patrick, Deci, & Williams, 2008). In this study, the SDI was a significant and negative predictor of depressive symptoms in university students; consistent with those observed by Duda et al. (2014).
The true importance of any treatment lies in its long-term effects. Six months after completing the intervention, some of the ET treatment participants had improved their outcomes even further. The percentage of participants scoring ≤ 50% of their initial (baseline) score in depressive symptoms following the 8-week ET treatment had increased by 10% at the six month follow-up. We believe that the explanation can be found in the number of participants who independently decided to continue the practice of moderate or vigorous PA at least three days a week in their free time. Prior studies found that the SDI predicts the future intention to continue to practice PA (Cecchini, Fernández-Río, & Méndez-Giménez, 2014), and this is what seems to have happened in the ET treatment condition, in which 63% of the participants chose to continue actively practicing PA. In fact, at post-2, the SDI was again a significant predictor of low levels of depressive symptoms.
TARGET strategies can have a direct effect on depressive symptoms at the time of the intervention, and an indirect effect after completion because of their impact on future levels of PA. The direct effect occurs during the intervention and can be explained by its incidence on the levels of self-determined motivation associated with weekly PA (Gourlan, Trouilloud, & Sarrazin, 2013), which translates into a decrease of depressive symptoms at post-1. The indirect effect is long-term, and occurs after the intervention because the increase of the SDI at post-1 predicts higher levels of PA at post-2 and, consequently, an additional decrease of depressive symptoms. On the whole, the group that was provided with Epstein's TARGET strategies reached a clinical efficacy of around 70% after a follow-up period of six months. It is exceedingly difficult to find similar efficacy rates in the literature. Well-established treatments for depression, such as the “Coping with Depression Course” of Lewinsohn, Antonuccio, Steinmetz and Teri (1984), “Cognitive Therapy” by Beck (1991), and “Interpersonal Psychotherapy” by Klerman and Weissman (1993), all have difficulties reaching these levels of effectiveness. We believe that the reasons behind these results are related to the junction among physical exercise, external support, and autonomous self-regulation skills. Previous research (e.g., Dunn, Trivedi, Kampert, Clark, & Chambliss, 2007), which used the Hamilton Rating Scale for Depression, and included treatments based on aerobic physical exercise exclusively, showed a clinical efficacy of 31% (three days per week, during 12 weeks), and 64% (five days per week, during 12 weeks). In the first case, results are similar to those found in the NET group (i.e., 25.93% of efficacy; three days per week, during 8 weeks). In the second case, however, the efficacy in the ET group was slightly lower after a period of six months.
Previous studies have related the TARGET strategies to the increase in the students’ perceptions of skill and effort, competence, and motor skills (Martin, Rudisill, & Hastie, 2009), which can lead to an increase of PA in their free time. In their review of studies on motivational climate, Braithwaite et al. (2011) reported that TARGET-based interventions had significant effects on some indicators of health and physical fitness, such as heart rate, cardiovascular capacity, frequency of exercise, and nutritional behaviors.
The present study questions that the incidence of PA on depressive symptoms only depends on dosage and intensity. Motivational climate is a key issue, as it can be used to break the isolation by promoting social interaction in the depressive population (Seime & Vickers, 2006). The practice of PA should be carried out in a pleasant and amusing environment in order to promote social relations. The effects of PA can be greatly enhanced by those added effects which can be derived from the pleasure of its practice in an integrative social context.
A recent theoretical framework has attempted to conceptualize and relate PA and mood, and it has been suggested that moderate-intensity exercise is associated with more positive outcomes because it is related to the pleasure of practicing, whereas vigorous intensities are associated with a negative affect, or dislike (Lind, Joens-Matre, & Ekkekakis, 2005). In this study, we propose that mood is more closely related to the motivational climate than to the intensity of practice. In fact, people who are more motivated also make a greater effort and these improvements are due, at least in part, to the mutual support and social relationships provided when participating in PA with other people (Méndez-Giménez, Cecchini, & Fernández-Río, 2014).
Due to the factors that have been outlined above, interventions in PA to alleviate depressive symptoms should: (a) propose varied and flexible tasks that pose personal challenge and promote active participation; (b) create an appropriate training environment to meet individual and collective demands; (c) foster participation in the decision-making process; (d) help participants to assume the responsibility of their own personal development by teaching self-management and self-control skills; (e) recognize individual progress, effort and improvement; (f) ensure equal opportunities; (h) use flexible and cooperative groupings; (i) promote helping others; (j) emphasize creative solutions to training problems; (k) develop assessment criteria based on effort, improvement, persistence, and progress towards individual goals; (l) acknowledge that participants do not train, learn, or develop at the same speed; (m) provide enough time before moving on to the next stage in the development of competences; (n) try to spend the same time with all the participants; (o) help participants to establish long-term training programs (Duda & Balaguer, 2007).
Certain potential methodological problems and limitations of the present investigation should also be mentioned. Firstly, the sample was small. Secondly, only students who reached a score of 29 or more and who were characterized by having notable symptoms of depression were selected, and therefore, the results might only be generalizable to these specific students. Thirdly, the average follow-up period was only six months. Fourthly, the study was based on self-report measures, which may include errors of judgment, difficulties and incorrect interpretation of the questions, and the possibility of socially desirable answers. Finally, it is necessary to conduct further research, using more specific measurement instruments, and with greater clinical utility.
FundingThis study has been conducted thanks to the I+D+I research grant # DEP2012-31997 funded by the Ministerio de Economía y Competitividad of Spain.
