



Previous studies of traditional and modern value orientations in individuals found mediated predictive relationships of these values on particular mental disorders. The aim of this study with samples from three countries (Germany, Russia, and China) is to extend findings on mental health (MH) and value orientations to broader MH indicators and two types of mediators, i.e. social support and resilience in accordance to a theory of values and modernization/postmodernization. The multisite study was conducted in the three countries. A path-model with traditional values predicting MH mediated by social support, and modern values predicting MH mediated by resilience was tested in all three countries. As expected, value orientations were for the most part strongest in China, followed by Russia and Germany. Structural equation modeling supported the assumption of mediated prediction of MH by value orientations by and large. The traditional value benevolence predicts social support whereas the modern value self-direction predicts resilience. Value orientations are a sensitive tool to empirically describe cross-cultural differences. The findings indicate that personal value orientations are meaningful predictors of MH. The analysis of personal values shows promise in linking public health, cross-cultural and modernization issues.
Estudios previos sobre orientaciones de valores tradicionales y modernos encontraron relaciones predictivas mediadas con trastornos mentales particulares. El objetivo de este estudio con muestras procedentes de tres países (Alemania, Rusia y China) es ampliar los resultados indicadores más amplios de salud mental (SM) y dos tipos de mediadores (apoyo social y resiliencia), de acuerdo a la teoría de los valores y la modernización/postmodernización. Se probó en los tres países un path-model con valores tradicionales prediciendo la SM mediada por el apoyo social y valores modernos prediciendo la SM mediada por la resiliencia. Como era de esperar, las orientaciones de valores eran en su mayor parte más fuertes en China, seguido por Rusia y Alemania. Modelos de ecuaciones estructurales apoyaron la hipótesis de la predicción de la SM mediada por las orientaciones de valores en general. La benevolencia de valores tradicionales predice el apoyo social, mientras que el valor autodirección moderna predice la resiliencia. Las orientaciones de valores constituyen una herramienta sensible para describir empíricamente las diferencias interculturales. Los resultados indican que las orientaciones de valores personales son predictores significativos de la SM. El análisis de los valores personales se muestra prometedor en la salud pública transcultural y cuestiones de modernización.
Basic value orientations recently received increasing interest in studying occupational health issues (e.g., Diaz Bretones & Gonzalez, 2011; Wang, Lu, & Lu, 2014), health consequences of migrants (Vecchione, Caprara, Schoen, Castro, & Schwartz, 2012) or mental health in military service (Zimmermann et al., 2014). Basic or cultural values refer to things that individuals believe are worth desiring in life and thus guide their behavior. According to Rokeach (1973), value orientations include cognitive, affective, and behavioral components; value orientations are cognitions of the desirable that foster emotions and motivate behavior. In the present study, value orientations are examined using Schwartz's model (1992), which was developed based on the work of Rokeach. Schwartz views value orientations as the criteria people use to select and justify actions and to evaluate people and events. Value orientations thus serve as one's own guidance of behavior and the evaluation of behavior of others.
Maercker et al. (2009) proposed to group the ten single value orientations by Schwartz into traditional (security, conformity, tradition, benevolence, universalism) versus modern (self-direction, stimulation, hedonism, achievement, power) values and to introduce both as basic cultural value orientations in mental health research. Traditional cultural values stress collectivism, submissive self-restriction, preservation of traditional practices, protection, and stability. Modern cultural values represent motivations to pursue personal success and dominance over others or gratification for oneself. For trauma and stress-related disorders it has been shown that modern values are protective against posttraumatic stress via mediating social sharing processes, while traditional values increase this stress via the same mediation pathway (Maercker et al., 2009). This contradicted the popular long-standing assumption that traditional values are better for health preservation while modern values derogate health (cf. Graham, 2010; Kleinman & Good, 1985). However, a subsequent study suggested that these effect patterns are partly affected when other types of health outcome and particular age groups of adults are concerned (Müller, Forstmeier, Wagner, & Maercker, 2011).
The present large-scale multi-national survey of student mental health and its predictors allows broadening the scope towards broader indicators of mental health, namely positive mental health and depression. At the same time, the survey study allows the study of broader health-promoting factors of social support and resilience as potential mediators of the cultural value—mental health relationship. It is part of a larger research program investigating predictors, transcultural aspects and time course of mental health in a series of cross-sectional and longitudinal studies (BOOM research program; Margraf & Schneider, 2014).
Based on theories of social belongingness by Baumeister (2005) and the role of autonomy in resilience (Richardson, 2002), as well as own previous findings (Maercker et al., 2009) we hypothesize a prediction model in which traditional values mainly take effect on mental health via social support while modern values do so via the individuals’ capacity for resilience.
According to Baumeister (2005), all human beings are in need of a certain minimum quantity of regular, satisfying social interactions. He argues that traditional human culture is compelled and conditioned by pressure to belong and that this belongingness is relevant for the promotion of psychological wellbeing. This has been supported in various lines of research (e.g., depression in children, caregivers of demented individuals, psychoeducational health interventions) (for a review see Kawachi & Berkman, 2001). However, it has been shown that from the actor's perspective, social ties may also entail psychological costs in the sense of indebtedness and obligation (Cohen, 2004).
Resilience is still a relatively recent construct in psychology with slightly divergent definitions. In some of these definitions it is congruently viewed as a construct, which includes variables like temperament and personality, in addition to specific skills (e.g. active problem-solving) that allow individuals to cope well with life stress (Richardson, 2002). Following this, resilience refers to the motivational forces of a person and his/her creation of experiences that foster activation and utilization of own forces that drive toward self-actualization and to reintegrate from disruptions. The conceptual closeness of resilience (in these definitions) to autonomy motivation leads us to assume that modern values (e.g. self-direction, achievement, hedonism) are predictors of resilience.
So far, we have not discussed if different magnitudes or patterns of traditional or modern values are assumed to have differential impacts on mental health. Common knowledge suggests that there are differences in value orientations across cultures or nations. A theoretical framework capturing this assumption is Inglehart's model of value persistence and modernization/postmodernization (Inglehart, 1997; Inglehart & Baker, 2000). This model distinguishes different states of industrialization (concerning modernization) or the rise of the service and knowledge sector (concerning post modernization) in society. Inglehart (1997) proposes that traditional values are sustained during these processes or even strengthened while modern values are specific to modern and postmodern societies. This persistence of traditional values despite economic and political changes is a part of the cultural heritage of a given society. The model also argues that the differences between the values held by members of different traditions in a given society are much smaller than are cross-national differences (Inglehart & Baker, 2000, p. 18). Thus, a consequence of this theory is that rapidly changing societies, like modern-day China, show both highest traditional and modern values.
The current study aims to investigate in a Chinese, Russian, and German sample of University students the following assumptions: (1) According to Inglehart's values theory, traditional values should be most pronounced in China, followed by Russia in contrast to lower representation in Germany; (2) A path-model with traditional values predicting mental health mediated by social support, and modern values predicting mental health mediated by resilience is valid in all three countries.
MethodParticipantsQuestionnaires were administered in different ways in the three countries. Data from students of universities in China (Capital Normal University Beijing, Hebei United University, Nanjing University), Germany (Ruhr-University Bochum) and Russia (Lomonossov University Moscow, University of Voronesh, University of Orenburg) were gathered by the collaborating Departments of Psychology specifically for the BOOM research program. In Germany, the University of Bochum set up an online portal for their students that included the questionnaires. Data from this online investigation were available for N=1.105 persons. In Russia, paper-and-pencil questionnaires were applied at the three collaborating universities to N=3.743 students. In the three Chinese sites, from the N=9,019 students, 59% participated in grouping-online sessions that gathered in computer labs and were supervised by 1-2 research investigators and 41% participated in paper-pencil (41%) testing. All questionnaires were administered in the native languages using either available publishes versions or the customary translation-backtranslation method.
Since the data were anonymized from the very beginning of data collection, no statement by an institutional board/ethics committee was required for/in Russia and China. The study in total and in specific its German part was approved by the ethics committee of the Faculty of Psychology at Ruhr-University on May 12, 2011. Approval to administer the questionnaires was granted by the Faculty of Psychology at Ruhr-University Bochum on May 12, 2011 and renewed on October 2012. The approvals for the German site were communicated to the participating Chinese and Russian Universities who acknowledged these approvals. The Chinese and Russian samples included University students below age 18. Chinese and Russian laws grant officially inscribed University students of all ages the rights to decide for themselves about study-related issues including participation in studies.
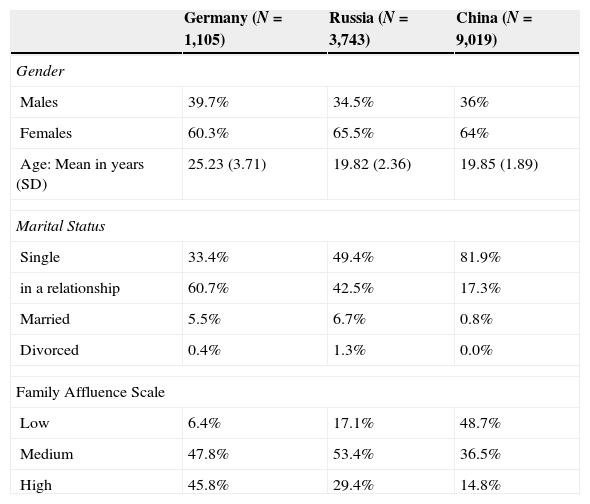
Table 1 shows the demographic characteristics. While gender ratios are not different between the samples, mean age was (F=2949.07; df=2; p<.001) with the German participants being older than the Chinese or Russians. Other differences were marital status and the affluence of parent's family.
Demographic features of the three samples.
| Germany (N=1,105) | Russia (N=3,743) | China (N=9,019) | |
|---|---|---|---|
| Gender | |||
| Males | 39.7% | 34.5% | 36% |
| Females | 60.3% | 65.5% | 64% |
| Age: Mean in years (SD) | 25.23 (3.71) | 19.82 (2.36) | 19.85 (1.89) |
| Marital Status | |||
| Single | 33.4% | 49.4% | 81.9% |
| in a relationship | 60.7% | 42.5% | 17.3% |
| Married | 5.5% | 6.7% | 0.8% |
| Divorced | 0.4% | 1.3% | 0.0% |
| Family Affluence Scale | |||
| Low | 6.4% | 17.1% | 48.7% |
| Medium | 47.8% | 53.4% | 36.5% |
| High | 45.8% | 29.4% | 14.8% |
Family Affluence Scale. The FAS (Boyce, Torsheim, Currie, & Zambon, 2006), a four-item measure of family wealth, has been developed in the WHO Health Behavior in School-aged Children Study and has been validated by correlations with the Gross National Product across 35 countries. Its questions are (either with 2 or 3 response alternatives): ‘Does your family own a car, van or truck?’, ‘Do you have your own bedroom for yourself?’, ‘During the past 12 months, how many times did you travel away on holiday with your family?’, and ‘How many computers does your family own?’. The FAS score is calculated by summing up the responses to these items.
Value orientations. Basic value orientations were measured with the PVQ 21 item version that is based on the circumflex models of basic values and had been used in the European Social Survey (Schwartz, 2007). Each item describes a person in two sentences (‘portrait’). Respondents are asked to assess how similar to the portrait person they are. Answers range from ‘very similar’ to ‘very dissimilar’, coded from 1 to 6. Two items each measured the values except that three items measured universalism. For example, two items measured hedonism (‘Having a good time is important to her. She likes to “spoil” herself.’, and ‘She seeks every chance she can to have fun. It is important to her to do things that give her pleasure.’). In the current study two sum scales were calculated (traditional values: security, conformity, tradition, benevolence, universalism; modern values: self-direction, stimulation, hedonism, achievement, power). The native language versions of the PVQ have been validated previously for the languages (see European Social Survey, ESS, 2008; Maercker et al., 2009). The alpha reliability coefficients for traditional/modern value sum scores were, respectively, .67/.73 in Germany; .76/.78 in Russia; .77/.77 in China. Reliability coefficients of the ten basic values ranged from .32 (tradition/customs orientation in China) to .73 (achievement in Germany).
Resilience. The scale (Schumacher, Leppert, Gunzelmann, Strauβ, & Brähler, 2005; Wagnild & Young, 1993) consists of 11 items assessing personality characteristics (e.g., ‘I like me’, ‘I keep interested in many things’, ‘I have enough energy’) on a 7-point Likert scale. The German version has been validated in various studies (Schumacher et al., 2005). The Chinese version was previously validated (Gao, Yang, Margraf, & Zhang, 2013). The alpha reliability coefficients were, respectively, .94 in Germany; .81 in Russia; .82 in China.
Social support. The F-SOZU is a well-established scale with 14 items (Fydrich, Sommer, Tydecks, & Brähler., 2009). It measures perceived emotional and instrumental support and social integration by items with a 5-point scale in one sum score (sample item: “I know whom I can go to whenever I feel low”). The alpha reliability coefficients were, respectively, .95 in Germany; .94 in Russia; .95 in China.
Positive mental health. The 9 items questionnaire (Lukat, Margraf, Becker, van der Veld, & Lutz, 2014) comprises statements like: ‘Much of what I do brings me joy’, ‘I enjoy my life’, ‘I am often carefree and in good spirits¿. An earlier version of the scale has been successfully used in our earlier Dresden Predictor Study (see Trumpf, Becker, Vriends, Meyer, & Margraf, 2009; Trumpf et al., 2010) where it showed good reliability and predictive power for various anxiety disorders (Vriends, Becker, Meyer, Michael, & Margraf, 2007; Vriends, Becker, Meyer, Williams et al., 2007). No previous validation existed in Russian and Chinese language; the customary translation-backtranslation-modification procedure was thus applied. The alpha reliability coefficients in the present study were, respectively, .93 in Germany; .86 in Russia; .90 in China. To complement the salutogenic mental health construct, the following more traditional depression scale was applied in parallel.
Depression was measured by a subscale of the Depression Anxiety Stress Scales 21 (DASS-21; Henry & Crawford, 2005) which showed excellent psychometric properties in its validation study. The seven depression items are presented with a 4-point Likert scale. Validated versions exist in the three languages. The alpha reliability coefficients were, respectively, .89 in Germany; .83 in Russia; .79 in China.
Statistical analysisWe first compared means of all model variables. Second, we computed zero-order bivariate correlations to assess the association between model variables and the main outcomes variable of positive mental health. Sum scores for traditional or modern values were additionally calculated.
We then used structural equation modeling. With regard to path analysis, from the five traditional and five modern values in each case two single values were selected as basic model predictors. Criteria were comparably highest correlations with mental health and not being direct neighbors in the circumflex model of values. Subsequently, the two traditional values predicted social support and the two modern values predicted resilience. We allowed the single value orientations to covariate freely as well as the error variances of the factors. Reciprocal paths between social support and resilience were also allowed. In addition to positive mental health as model outcome variable also depression was included into the model, mainly because the latter measure is more established and validated and thus allows comparisons with already existing studies.
We assessed the comprehensive measurement model in the same way in all three countries. We began by assessing the measurement model separately in each country. We used maximum likelihood to estimate parameters with SPSS Amos and evaluated the covariance structure models with several goodness of fit indices: chi-square, root mean square error of approximation (RMSEA, Steiger & Lind, 1980), comparative fit index (CFI, Bentler, 1990), and standardized root mean square residual (SRMR, Jöreskog & Sörbom, 1996).
Finally, we ran a multi-group analysis to assess measurement invariance of the scales of the variables across country samples. Model 1 assessed configural invariance – equivalence of the overall structure (i.e., the same number of factors and the same pattern of loadings) across countries. Model 2 examined metric invariance or equivalence of factor loadings across countries. These models were subsequently re-calculated for controlling for sample differences in gender, age, and family affluence by using parallelized subsamples.
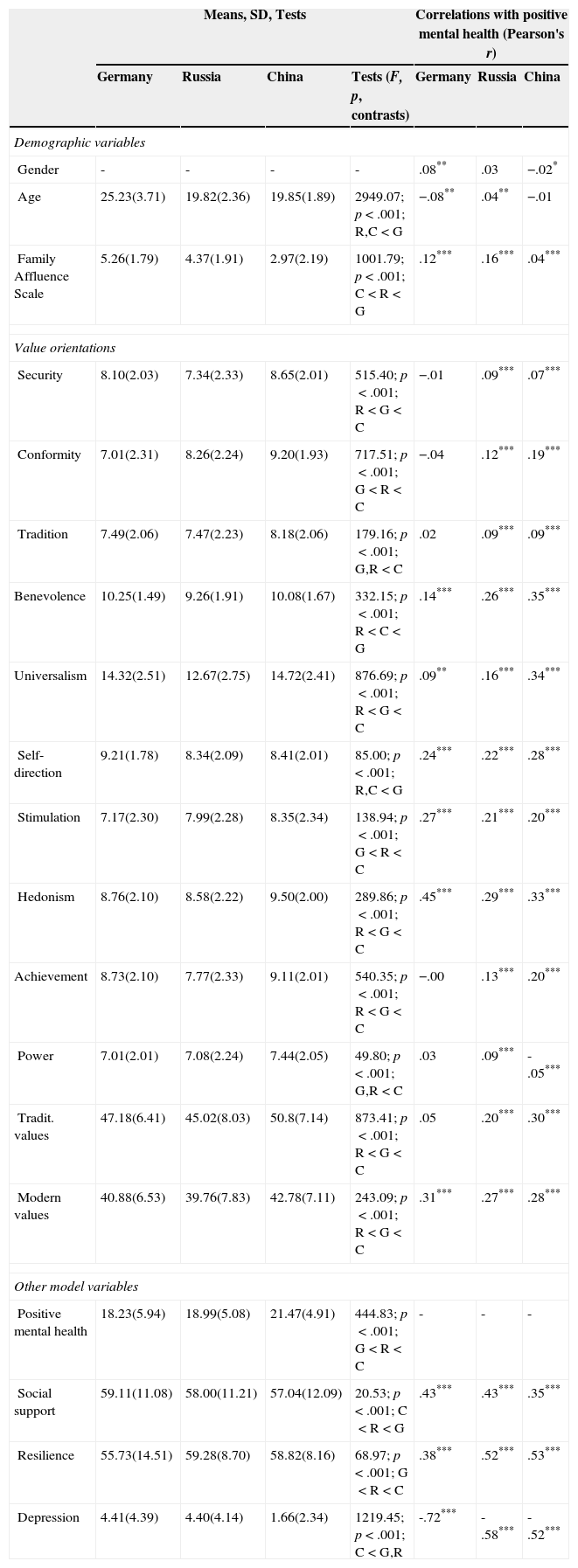
ResultsCross-national differences in valuesTable 2 shows that four of five traditional values are highest in China with the exception of benevolence, which is highest in Germany. These four values by and large consistently follow the rank order of China (highest), Russia (medium) and Germany (lowest). Of the five modern values, four are also highest in China with the exception of self-direction, which is highest in Germany. The rank order changed across the values with lowest scores in Russia for self-direction, hedonism and achievement and lowest scores in Germany for stimulation and power. The comparisons of sum scores (traditional, modern), however, established a general rank order: Russian lower than German lower than Chinese values.
Pearson bivariate correlations of positive mental health with socio-demographic, value-orientation, and other model variables.
| Means, SD, Tests | Correlations with positive mental health (Pearson's r) | ||||||
|---|---|---|---|---|---|---|---|
| Germany | Russia | China | Tests (F, p, contrasts) | Germany | Russia | China | |
| Demographic variables | |||||||
| Gender | - | - | - | - | .08** | .03 | −.02* |
| Age | 25.23(3.71) | 19.82(2.36) | 19.85(1.89) | 2949.07; p<.001; R,C<G | −.08** | .04** | −.01 |
| Family Affluence Scale | 5.26(1.79) | 4.37(1.91) | 2.97(2.19) | 1001.79; p<.001; C<R<G | .12*** | .16*** | .04*** |
| Value orientations | |||||||
| Security | 8.10(2.03) | 7.34(2.33) | 8.65(2.01) | 515.40; p<.001; R<G<C | −.01 | .09*** | .07*** |
| Conformity | 7.01(2.31) | 8.26(2.24) | 9.20(1.93) | 717.51; p<.001; G<R<C | −.04 | .12*** | .19*** |
| Tradition | 7.49(2.06) | 7.47(2.23) | 8.18(2.06) | 179.16; p<.001; G,R<C | .02 | .09*** | .09*** |
| Benevolence | 10.25(1.49) | 9.26(1.91) | 10.08(1.67) | 332.15; p<.001; R<C<G | .14*** | .26*** | .35*** |
| Universalism | 14.32(2.51) | 12.67(2.75) | 14.72(2.41) | 876.69; p<.001; R<G<C | .09** | .16*** | .34*** |
| Self-direction | 9.21(1.78) | 8.34(2.09) | 8.41(2.01) | 85.00; p<.001; R,C<G | .24*** | .22*** | .28*** |
| Stimulation | 7.17(2.30) | 7.99(2.28) | 8.35(2.34) | 138.94; p<.001; G<R<C | .27*** | .21*** | .20*** |
| Hedonism | 8.76(2.10) | 8.58(2.22) | 9.50(2.00) | 289.86; p<.001; R<G<C | .45*** | .29*** | .33*** |
| Achievement | 8.73(2.10) | 7.77(2.33) | 9.11(2.01) | 540.35; p<.001; R<G<C | −.00 | .13*** | .20*** |
| Power | 7.01(2.01) | 7.08(2.24) | 7.44(2.05) | 49.80; p<.001; G,R<C | .03 | .09*** | -.05*** |
| Tradit. values | 47.18(6.41) | 45.02(8.03) | 50.8(7.14) | 873.41; p<.001; R<G<C | .05 | .20*** | .30*** |
| Modern values | 40.88(6.53) | 39.76(7.83) | 42.78(7.11) | 243.09; p<.001; R<G<C | .31*** | .27*** | .28*** |
| Other model variables | |||||||
| Positive mental health | 18.23(5.94) | 18.99(5.08) | 21.47(4.91) | 444.83; p<.001; G<R<C | - | - | - |
| Social support | 59.11(11.08) | 58.00(11.21) | 57.04(12.09) | 20.53; p<.001; C<R<G | .43*** | .43*** | .35*** |
| Resilience | 55.73(14.51) | 59.28(8.70) | 58.82(8.16) | 68.97; p<.001; G<R<C | .38*** | .52*** | .53*** |
| Depression | 4.41(4.39) | 4.40(4.14) | 1.66(2.34) | 1219.45; p<.001; C<G,R | -.72*** | -.58*** | -.52*** |
Note: R<G<C: Russian significantly lower than German group which in turn is significantly lower than Chinese Group; R,G<C: Russian and German Groups significantly lower than Chinese Groups; etc.
All model variables were single-order correlated (Pearson's r) with positive mental health (Table 2, last three columns). For Russia and China, all single value orientations were significantly associated with positive mental health on a low level (r<.30) with three exceptions of somewhat higher correlations only for China (r<.40: benevolence, universalism, hedonism). For Germany, a more differentiated pattern appeared: two modern (achievement, power) and three traditional values (security, conformity, tradition) were not related with mental health; hedonism was most pronouncedly associated (r=.46) while the remaining again only showed low associations. All model variables had lower absolute correlation values with depression compared to its correlations with well-being except for rconformity-depression=.08 (p<.01) in Germany and rpower-depression=.12 (p<.001) in China.
Social support and resilience showed mid-sized correlations with positive mental health (from r=.35—.53). The inverse association between positive mental health and depression ranked from China (r=-.53), Russia (r=-.59) to Germany (r=-.73) (all p<.0001).
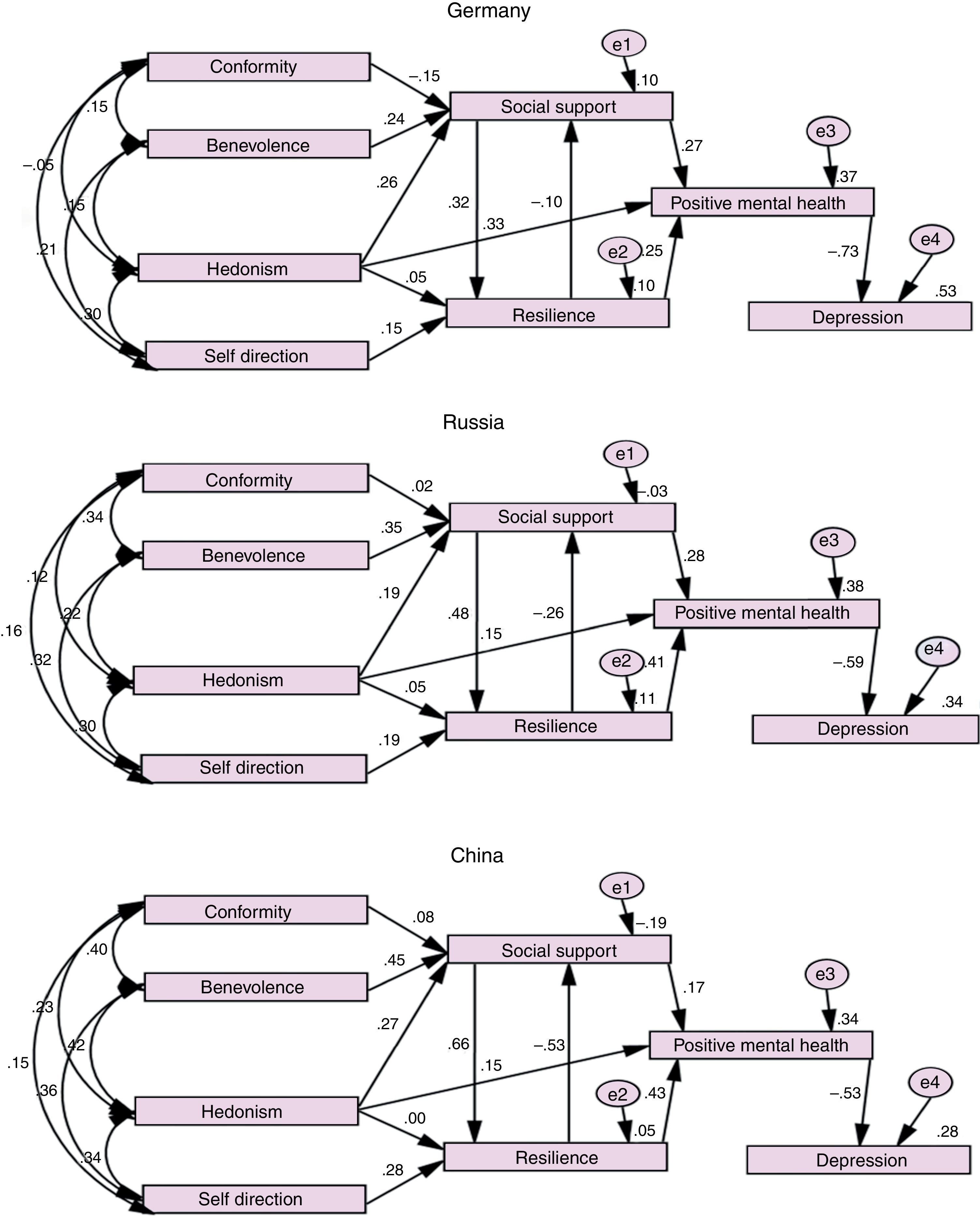
Measurement models and tests for invarianceA first model specified that conformity and benevolence exclusively predicted social support while self-direction and hedonism predicted resilience. Two of three country-specific models failed confirmation: Germany χ2(13)=265.97, p<.001, CFI=.87, SRMR=.09, RMSEA=.13 (.12–.15) and China χ2(13)=1270.60, p<.001, CFI=.92, SRMR=.07, RMSEA=.10 (.10–.11). Only the model for Russia fitted: χ2(13)=373.62, p<.001, CFI=.94, SRMR=.05, RMSEA=.09 (.08–.09).
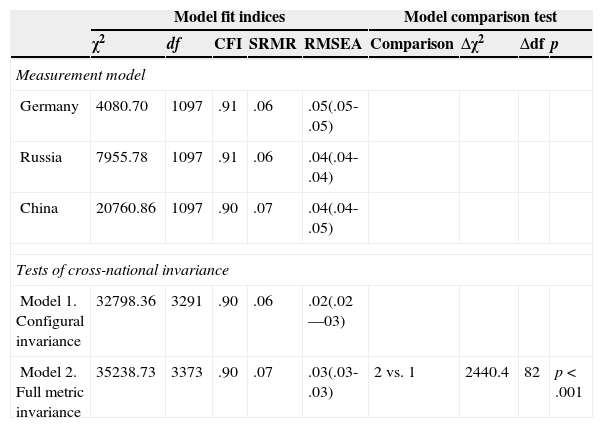
After allowing hedonism additionally predicting social support and (directly) positive mental health, the three models for each country fit the data very well with all fit indices within acceptable ranges (see Table 3, upper part, and Fig. 1). The factor loading of the indicators on the latent variables were for all relevant loadings in the German sample>.42; in the Russian sample>.10; and in the Chinese sample>.15 and significantly different from zero (p<.001). Some exceptions with non-significant loadings emerged: self-direction with social support, positive mental health and depression; conformity with resilience, positive mental health and depression; benevolence with resilience, positive mental health and, subsequently, depression. Thus, the model with its differentiation between social support and resilience predictors and mediated effects on positive mental health or, subsequently, depression was supported.
Goodness of fit statistics for the models tested.
| Model fit indices | Model comparison test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| χ2 | df | CFI | SRMR | RMSEA | Comparison | Δχ2 | Δdf | p | |
| Measurement model | |||||||||
| Germany | 4080.70 | 1097 | .91 | .06 | .05(.05-.05) | ||||
| Russia | 7955.78 | 1097 | .91 | .06 | .04(.04-.04) | ||||
| China | 20760.86 | 1097 | .90 | .07 | .04(.04-.05) | ||||
| Tests of cross-national invariance | |||||||||
| Model 1. Configural invariance | 32798.36 | 3291 | .90 | .06 | .02(.02—03) | ||||
| Model 2. Full metric invariance | 35238.73 | 3373 | .90 | .07 | .03(.03-.03) | 2 vs. 1 | 2440.4 | 82 | p<.001 |
, Russia (b), China (c). All paths in the German sample with loadings >.10, in the Russian sample with loadings >.02 and in the Chinese sample with loadings >.01 are significant.")
Having confirmed the same measurement model in each country, we were able to test the invariance of measurement across countries. The fit statistics in the lower part of Table 3 indicate an adequate (moderate) fit for the configural invariance model (Model 1). This suggests that the same factor structure holds for the three country samples. The fit statistics for the metric equivalence model (Model 2), which constrained all factor loadings to be equal across groups, however, failed an adequate fit. In addition, the chi-square difference test between the two models was statistically significant (delta χ2 (81)=2440.4, p<.001), supporting the non-equivalence so that metric invariance could not be retained. The model did not meet the minimum requirement for metric invariance of at least one equal loading for each measure (Meredith & Horn, 2001). Therefore only configural invariance was established.
Finally, we repeated the same model estimations and tests with subsamples that were parallelized for age, marital status and family affluence since these variables differed between the three national samples. For each subsample n=220 participants were included. By and large results remained identical with configural invariance confirmed but nor metric invariance for all three national samples. CFIs were somewhat reduced but the other indices for misspecified factor loadings (RMSEA) and for model misspecification (SRMR) remained acceptable indicating proof of the measurement model.
DiscussionThe study investigated if personal value orientations are meaningful predictors for mental health outcomes. It applied a distinction into two value categories, traditional and modern values (Ingelhart, 1997) that was already applied to previous studies on values and mental health (Maercker et al., 2009; Müller et al., 2011). Values or societal virtues are increasingly recognized as organizing principles for human behaviors, cognitions and affect expressions. Chinese virtues (
First, we hypothesized according to Inglehart's values theory (Inglehart & Baker, 2000), that traditional values would be most pronounced in China, followed by Russia in contrast to lower representation in Germany. Central parts of this hypothesis got supported with China having highest extents of value orientations that supported Inglehart's theory. It is also corroborated by findings by Jin, Zheng, & Xin (2009), who developed a Chinese Values Questionnaire (CVQ) and showed a tendency for the Chinese to think in terms of the “Good-person”, indicated by high scores on values of integrity, self-support, respect, and public interests. However, the Russian student sample did not rank midway but lowest for the value orientations. The early sociologist and social psychologist Émile Durkheim (1897/2009) had introduced the concept of ‘anomie’ to describe societal states in which ‘disorientation’ and the lack or frailty of value orientations is predominant, usually in countries that experienced setbacks. This concept could possibly explain why the value orientations in Russia by and large were lowest.
Exceptions of the hypothized pattern also appeared with regard to single values of benevolence (a traditional) and self-direction (a modern value) that were the only ones that are most pronounced in the German samples compared to the other samples. Convergent evidence for this finding exists only from research on temporal trends in psychopathology during the last 80 years where for the USA it was found that extrinsic goals including self-expression or narcissism increased while intrinsic goals such as affiliation decreased (Twenge et al., 2010). The findings for benevolence may be corroborated by psycho-historical data that were collected by Pinker (2011) showing an increase in benevolence emerging with economic progress (cf. Inglehart, 1997).
Second, we hypothesized that traditional values would predict mental health mediated by social support, while modern values predict mental health mediated by resilience—and that this is valid in all three countries. We applied a simplified modeling that only included two single value orientations for each the traditional and modern values (single values with the highest correlations with mental health across the three samples). By and large the structural equation model supported the theoretical model assumption with benevolence (significantly) and conformity (non-significantly) predicting social support, and self-direction supporting resilience.
This partial support for the model extends previous findings (Maercker et al., 2009; Müller et al., 2011) on the central role of value orientations for social-support processes in disorders specifically associated with stress (Maercker et al., 2013). In these studies traditional values had deteriorating effects on PTSD, but had relieving effects on overcoming complicated grief or adjustment disorder. Thus, the notion of a Janus phase of social support processes in conjunction with mental health that had been outlined by many authors (e.g., Cohen, 2004; Kawachi & Berkman, 2001) is again supported. Of particular importance remains the overall finding of the present study that traditional values seem primarily important for social support with regard to mental health.
Regarding resilience as a mediator for mental health, the findings looked more mixed. Only self-direction predicted resilience as hypothesized according to a resilience definition that highlights the individual's ability to cope well with life stress (Richardson, 2002). The modern value hedonism failed to directly predict resilience; instead it contributed directly to positive mental health and—somewhat less—social support. Hedonism is still an under-researched phenomenon in psychology, although it seems relevant as a core process of self and identity regulation in contemporary psychology (Baumeister, 2011). One obvious concern could be that the constructs of positive mental health and hedonism overlap to explain the aberration of our hypothesis at stake, but a view on the item formulations (see method section above) does not suggest a complete overlap. In a recent study on German military service personnel, hedonism also stood out with the comparably highest prediction of all value orientations for mental health (Zimmermann et al., 2014).
There are several limitations to the present study. First, given the cross-sectional nature of the data, conclusions on real causality cannot be drawn. Although the path models fit the data, only experimental or longitudinal studies can provide firm confirmation of causal or conditional relationships. Second, the three samples differ on demographic features, with the German sample being somewhat older; the German as well as Russian samples at higher percentages in a romantic relationship and from a higher family affluence backgrounds. However, control analyses by parallelized subsamples provided proof of our original path models albeit with lower test values. Furthermore, other potential demographic confounders were not investigated, e.g. rural or urban family background, which may play a role in the processes under investigation. Third, the data were obtained exclusively by self-report. This method has certain advantages for cross-cultural survey research, e.g. the measures are economical and easy to administer). However, self-report measures may fail to capture well-being, depression or value orientation processes in their full complexity. Finally, generalization of the results towards other age or societal groups than University students is not possible yet, since the study focused only on those better-educated parts of the society.
In conclusion, the present study tries to contribute to a more culturally oriented research agenda for predicting mental health in students by values and the main psychosocial constructs of social support and resilience. Its main findings of differential pathways of traditional or modern values to mental health still needs corroboration and refinement through other research.
Available online 13 August 2014
