



The main goal of our study was to investigate and compare the relationship between temperament traits postulated by the Regulative Theory of Temperament (RTT) and social support dimensions with the level of trauma symptoms, as appear in posttraumatic stress disorder (PTSD), in an HIV/AIDS patient sample [HIV+ (n=182) and AIDS (n=128)] and in patients suffering from chronic pain (rheumatoid arthritis; n=150). The level of trauma symptoms was assessed with the PTSD Factorial Version Inventory (PTSD-F), temperament was measured with the Formal Characteristics of Behaviour–Temperament Inventory (FCB-TI), and social support was tested with the Berlin Social Support Scales (BSSS). Significant predictors of trauma symptoms among participants were temperament traits (emotional reactivity, perseveration, and sensory sensitivity), and social support dimensions (perceived support, need for support, support seeking, and actually received support). We also noticed significant differences between the levels of trauma symptoms, temperament, and social support between HIV/AIDS and chronic pain patients. The importance of trauma symptoms, as well as temperament traits and social support, should be taken into account in planning the forms of psychological support that should accompany pharmacotherapy for HIV/AIDS and chronic pain patients.
El objetivo fue investigar la relación entre rasgos de temperamento postulados por la Regulative Theory of Temperament (RTT) y dimensiones de apoyo social con el nivel de síntomas de trauma, como aparecen en el trastorno de estrés postraumático (TEPT), en pacientes VIH+ (n = 182) y SIDA (n = 128)] y en pacientes que sufren dolor crónico (artritis reumatoide; n = 150). El nivel de los síntomas de trauma se evaluó con el Inventario TEPT-F, el temperamento se midió con Inventario FCB-TI y el apoyo social con las Escalas BSSS. Los predictores significativos de síntomas de trauma fueron los rasgos de temperamento (reactividad emocional, perseverancia y sensibilidad sensorial) y las dimensiones de apoyo social (apoyo percibido, necesidad de apoyo, búsqueda de apoyo y apoyo real recibido). También destacan las diferencias significativas entre los niveles de síntomas de trauma, el temperamento y el apoyo social entre el grupo VIH/SIDA y pacientes con dolor crónico. La importancia de los síntomas de trauma, así como los rasgos de temperamento y el apoyo social, se deben tomar en cuenta en la planificación de las formas de apoyo psicológico que deben acompañar a la farmacoterapia para el VIH/SIDA y pacientes con dolor crónico.
There is increasing evidence of the association between trauma symptoms, as appear in posttraumatic stress disorder (PTSD; symptoms of recurring flashbacks, avoidance of memories of the traumatic event, hyperarousal) and experiencing various medical conditions (Moye & Rouse, 2014; Tedstone & Tarrier, 2003). The prevalence of medical illness-related trauma symptoms has been observed in cancer patients (Kangas, Henry, & Bryant, 2005), patients with cardiovascular diseases (Coughlin, 2011), HIV+ people (Rzeszutek, Oniszczenko, & Firląg–Burkacka, 2012), and individuals suffering from chronic pain (Asmundson, 2014; Britvić et al., 2015; Rzeszutek, Oniszczenko, Schier, Biernat-Kałuża, & Gasik, 2015). Trauma symptoms in these patient groups are usually related to receiving a medical diagnosis of a life-threatening illness, but they may also be linked to painful treatment and the stressful course of the disease (Norman, Stein, Dimsdale, & Hoyt, 2008). Medical illness-related trauma symptoms are often underdiagnosed and, when untreated, may increase medical and psychiatric morbidity, impact patients’ use of healthcare resources and create added burden for the individual, family, and health care system for the patient's recovery (French-Rosas, Moye, & Naik, 2011).
Trauma symptoms among HIV+ individuals are mainly associated with being diagnosed with a potentially life-threatening disease (Beckerman & Auerbach, 2010), but they are also attributed to the unpredictability of the progression of HIV (Theuninck, Lake, & Gibson, 2010) and social stigmatization (Breet, Kagee, & Seedat, 2014). Trauma symptoms in HIV+ people are usually linked to poor medication adherence (Machtinger, Wilson, Haberer, & Weiss, 2012), greater substance abuse (Nugent, Lally, Brown, Knopik, & McGeary, 2012), and deterioration in immune functioning by lowering CD4 cell counts and increasing the level of physical HIV symptoms (Boarts, Sledjeski, Bogart, & Delahanty, 2006).
The relationship between chronic pain and PTSD was first described by Sharp and Harvey (2001) in their mutual maintenance model, in which these authors proved that chronic pain and PTSD share a few similar intrapsychic mechanisms, such as an increased level of arousal, attentional biases, and avoidance coping style, which are responsible for mutual maintenance of these two disorders. Several other studies have indicated that trauma symptoms in individuals suffering from chronic pain may be particularly linked to overwhelming, chronic pain, precluding normal social functioning, substantially reducing quality of life, and causing significant disability and functional limitations (Beck & Clapp, 2011; Rzeszutek et al., 2015) as well as a risk of premature mortality, which was especially observed among patients with rheumatoid arthritis (Benka, Nagyova, & Rosenberger, 2014). Conversely, other authors found that chronic pain is one of the most often reported physical health complaints among people who have experienced traumatic experiences and developed PTSD (Kendall-Tackett, 2009), which was especially observed among war veterans (Irwin, Konnert, Wong, & O’Neill, 2014) and survivors of natural disasters (Leythan & Powel, 2012).
Some data suggests that personality traits play a significant role in responding to trauma, being either a risk or a protective factor against PTSD (Lauterbach & Vrana, 2001). In particular, neuroticism (LaFauci, Schutt, & Marotta, 2011) and temperament traits identified by Cloninger, such as harm avoidance (the tendency to excessive worrying, shyness, being fearful and easily fatigued; Cloninger, Svrakic, & Przybeck, 1993) are thought to contribute to the exacerbation of trauma symptoms. Alternately, extraversion and conscientiousness from the NEO-FFI model of personality (Lauterbach & Vrana, 2001) increase trauma symptoms resilience. All of the personality traits mentioned above correlate with the temperament traits from the Regulative Theory of Temperament (RTT) (Hornowska, 2011), which were the focus of this study.
Regulative Theory of Temperament (RTT) emphasises the role of temperament in the regulation of people's relations with their environment (Strelau, 2008). According to RTT, temperament refers to basic, relatively stable personality traits, which are manifested in the energetic characteristics (response intensity) and temporal characteristics (speed, tempo and mobility) of behaviour. RTT postulates following temperament traits: briskness (the tendency to respond swiftly, to maintain a high tempo of activity, to switch easily from one behaviour to another); perseveration (the tendency to maintain and repeat behaviours after the situation which evoked these behaviours has changed); sensory sensitivity (the capacity to respond to sensory stimuli whose stimulating value is low); emotional reactivity (the tendency to respond intensely to emotogenic stimuli); endurance (the capacity to respond adequately in situations requiring highly stimulating activity) and activity (the tendency to engage in behaviours which are themselves highly stimulating) (Strelau, 2008). The significance of these traits comes from the fact that temperament is present at birth, and the biological mechanisms linked to these traits work together to regulate the state of stress as well as its consequences. The relationship between temperament traits from the RTT and trauma symptoms has been observed in the case of many traumatic events such as trauma after flooding (Strelau & Zawadzki, 2005), trauma among participants in motor vehicle accidents (Zawadzki & Popiel, 2011), trauma associated with HIV infection (Rzeszutek & Oniszczenko, 2013) and trauma among people suffering from chronic pain (Rzeszutek et al., 2015). Specifically, emotional reactivity and perseveration are considered as predictors, while briskness, activity, endurance and sensory sensitivity are seen as protective resources in the case of traumatic stress (Strelau, 2008). The location of RTT traits among many other temperament and personality theories has been proven by means of correlational and factor analytic studies conducted by other authors (Kandler, Held, Kroll, & Bergeler, 2012).
Finally, poor social support following a traumatic event is one of the greatest risk factors for PTSD (Ozer, Best, Lipsey, & Weiss, 2003). In early studies on the role of social support in the course of PTSD, it was noted that social support can act as a buffer against traumatic stress (Cohen & Wills, 1985). Further research has proven that the presence of negative social interaction (e.g., hostile reactions from the family) was a more significant risk factor for PTSD compared to the absence of positive social support (Kaniasty & Norris, 2008). In particular, Łuszczyńska, Kowalska, Mazurkiewicz, and Schwarzer (2006) underlined the significance of adequateness of support to the trauma survivor's needs.
Current studyThe main goal of our study was to investigate the relationship between temperament traits postulated by the RTT and social support dimensions with the level of trauma symptoms in a HIV/AIDS sample (HIV+ and AIDS patients) and in patients suffering from chronic pain, as the example of patients with rheumatoid arthritis (RA). Although this study was mainly explorative, as it was the first research to compare the relationship between temperament traits and social support dimensions with the level of trauma symptoms in such samples, we formulated specific hypotheses based on the previous studies on the link between temperament traits from RTT, social support and trauma symptoms. Firstly, we expected that HIV/AIDS patients would differ from RA patients in respect of the level of temperament traits, social support dimensions and the intensity of trauma symptoms. Secondly, we expected, on the one hand, a positive association between the level of emotional reactivity and perseveration, and, on the other hand, a negative association between the level of briskness, activity, endurance and sensory sensitivity and the level of trauma symptoms among participants. Finally, we expected a negative link between aspects of social support (perceived social support, need for support, support seeking and actually received support) and the level trauma symptoms among participants.
MethodParticipants and procedureThe sample consisted of 460 adults divided into groups as follows. There were 310 HIV/AIDS patients: 182 HIV+ individuals [95 men and 87 women, aged 19 to 62 (M = 35.25; SD = 8.69)] and 128 individuals with AIDS [62 men and 66 women, aged 22 to 68 (M = 40.48; SD = 10.18)]. In addition, there were 150 patients with a clinical diagnosis of rheumatoid arthritis [42 men and 108 women, aged 20 to 84 (M = 55.45; SD = 14.40)]. This was an anonymous, cross-sectional study, and participation was voluntary. The research questionnaires were distributed in paper form by the professional pollsters in Warsaw between the years 2013 and 2015. HIV/AIDS participants were recruited from patients of Warsaw's Hospital for Infectious Diseases. Participants suffering from RA were recruited from patients of the Institute of Rheumatology in Warsaw, the Military Institute of Medicine in Warsaw, and the Department of Rheumatology at the Central Clinical Hospital in Warsaw. The study response rates were: 56% HIV/AIDS and 66% RA. Participants were asked to complete a paper-pencil version of the measures. Informed consent was obtained from all patients before they were included in the study, and participants were not remunerated. The research project was approved by the local ethics commission of the Faculty of Psychology, University of Finance and Management.
MeasuresTo measure the level of trauma symptoms in the studied patient group, we used the PTSD Factorial Inventory (PTSD-F; Strelau, Zawadzki, Oniszczenko, & Sobolewski, 2002). This inventory contains 30 items, which are divided into three scales: intrusion/arousal (recurrent thoughts relating to the traumatic event and causing arousal; 15 items; scores range 0-45), avoidance/numbing (avoidance of trauma-related stimuli and weakened response to these stimuli; 15 items; scores range 0-45), and a global trauma score (all 30 items; scores range 0-90). Higher scores in the PTSD-F scales indicate higher levels of trauma symptoms. The theoretical basis for the construction of the PTSD-F was the criteria for PTSD contained in the DSM-IV (American Psychiatric Association, 1994). The PTSD-F has satisfactory psychometric properties: assessed with Cronbach's α, the reliabilities for the intrusion/arousal scale, the avoidance/numbing scale, and the global trauma score are .96, .92, and .93, respectively.
Temperament traits were assessed with the Formal Characteristics of Behaviour – Temperament Inventory (FCB-TI), which was constructed as an attempt at operationalizing Strelau's Regulative Theory of Temperament (Zawadzki & Strelau, 1997). The FCB-TI consists of 120 items that describe temperament traits, which were defined in the Introduction section (Cronbach α’s are given in parentheses): Briskness (.77), Perseveration (.75), Sensory sensitivity (.72), Emotional reactivity (.84), Endurance (.83) and Ativity (.80). Scale scores can range from a minimum of 0 to a maximum of 20. Higher total scores in the FCB-TI scales indicate higher levels of the respective trait.
The nature of participants’ social support was assessed with the Berlin Social Support Scales (BSSS), adapted to Polish by Łuszczyńska and colleagues (2006). The BSSS are a set of six scales used to measure cognitive and behavioural aspects of social support, including: perceived support (perceived degree to which help from others is available; 8 items; scales scores range 8-32), need for support (the degree to which social support in stressful situations is important to the respondent; 4 items; scores range 4-16), support seeking (the frequency or range of support from others that the respondent seeks; 5 items; scores range 5-20), actually received support (the actual amount of support received from others; 15 items; scores range 15-60). Higher scores in the BSSS scales indicate higher levels of particular dimension of social support. Satisfactory Cronbach's α reliability coefficients were found for all scales, fluctuating between .74 and .90 (Łuszczyńska et al., 2006).
ResultsThe statistical analysis of the data was conducted using IBM SPSS 21 statistical software (SPSS Inc., 2012). Firstly, we compared means and standard deviations for temperament traits, social support aspects, and trauma symptoms level using analysis of variance and (depending on the degree of normality of the data) Kruskal-Wallis test to identify the statistical differences between these three groups of patients in general. The results of the analysis are presented in Table 1. However, in order to find statistically significant intergroup differences between HIV+ vs. RA patients and between AIDS vs RA patients we additionally performed t-test and (according to the degree of normality of data) U-Mann-Whitney test. We did not compare HIV+ and AIDS individuals as these data can be found in our other studies (Rzeszutek & Oniszczenko, 2013). Below we present Z values for the Mann-Whitney U-test and t- test values for statistically significant intergroup differences.
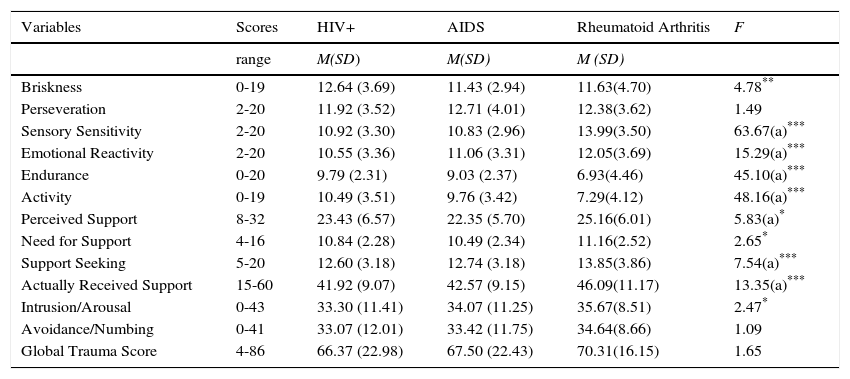
Means and Standard Deviations comparisons for temperament traits, social support dimensions, and trauma symptoms in HIV+ (n=182), AIDS (n=128), and rheumatoid arthritis (n=150) patients.
| Variables | Scores | HIV+ | AIDS | Rheumatoid Arthritis | F |
|---|---|---|---|---|---|
| range | M(SD) | M(SD) | M (SD) | ||
| Briskness | 0-19 | 12.64 (3.69) | 11.43 (2.94) | 11.63(4.70) | 4.78** |
| Perseveration | 2-20 | 11.92 (3.52) | 12.71 (4.01) | 12.38(3.62) | 1.49 |
| Sensory Sensitivity | 2-20 | 10.92 (3.30) | 10.83 (2.96) | 13.99(3.50) | 63.67(a)*** |
| Emotional Reactivity | 2-20 | 10.55 (3.36) | 11.06 (3.31) | 12.05(3.69) | 15.29(a)*** |
| Endurance | 0-20 | 9.79 (2.31) | 9.03 (2.37) | 6.93(4.46) | 45.10(a)*** |
| Activity | 0-19 | 10.49 (3.51) | 9.76 (3.42) | 7.29(4.12) | 48.16(a)*** |
| Perceived Support | 8-32 | 23.43 (6.57) | 22.35 (5.70) | 25.16(6.01) | 5.83(a)* |
| Need for Support | 4-16 | 10.84 (2.28) | 10.49 (2.34) | 11.16(2.52) | 2.65* |
| Support Seeking | 5-20 | 12.60 (3.18) | 12.74 (3.18) | 13.85(3.86) | 7.54(a)*** |
| Actually Received Support | 15-60 | 41.92 (9.07) | 42.57 (9.15) | 46.09(11.17) | 13.35(a)*** |
| Intrusion/Arousal | 0-43 | 33.30 (11.41) | 34.07 (11.25) | 35.67(8.51) | 2.47* |
| Avoidance/Numbing | 0-41 | 33.07 (12.01) | 33.42 (11.75) | 34.64(8.66) | 1.09 |
| Global Trauma Score | 4-86 | 66.37 (22.98) | 67.50 (22.43) | 70.31(16.15) | 1.65 |
Note: (a) chi square = value for Kruskal-Wallis test.
There were significant differences between HIV+ and rheumatoid arthritis patients when it came to: briskness (t = -2.25; p<.05), sensory sensitivity (Z = -7.98; p<.001), emotional reactivity (Z = -3.91; p<.001), endurance (Z = -6.72; p<.001), activity (Z = -6.94; p<.001), perceived support (Z = -2.42; p<.05), support seeking (Z = -2.74; p<.01), actually received support (Z = -3.66; p<.001), and the intrusion/arousal scale (t = 2.27; p<.05). We also found significant differences between AIDS and rheumatoid arthritis patients in terms of: sensory sensitivity (Z = -7.40; p<.001), emotional reactivity (Z = -2.70; p<.05), endurance (Z=-4.69; p<.001), activity (Z = -5.15; p< .001), perceived support (Z = -4.02; p<.001), need for support (t = 2.24; p<.05), support seeking (Z = -2.48; p<.05), and actually received support (Z = -2.82; p<.01).
Second, correlations in each patient group between temperament traits, social support dimensions, and the level of global trauma score were calculated using the Pearson product-moment correlation procedures. The analysis was performed on the global trauma score from the PTSD-F questionnaire, as intrusion/arousal and avoidance/numbing scales are highly intercorrelated (Strelau et al., 2002).
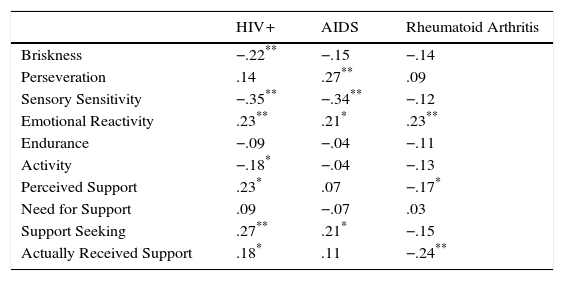
As can be seen in Table 2, the following correlations with the global trauma symptoms can be observed:
- -
HIV+ sample: emotional reactivity, perceived support, support seeking, and actually received support correlated positively, while briskness, sensory sensitivity, and activity correlated negatively.
- -
AIDS sample: perseveration, emotional reactivity, and support seeking correlated positively, while sensory sensitivity correlated negatively.
- -
Rheumatoid arthritis patients: emotional reactivity correlated positively, while perceived support and actually received support correlated negatively.
Pearson's r correlations between temperament traits, social support scales, and Global Trauma Score in HIV+ (n=182), AIDS (n=128), and rheumatoid arthritis (n=150) patients.
| HIV+ | AIDS | Rheumatoid Arthritis | |
|---|---|---|---|
| Briskness | −.22** | −.15 | −.14 |
| Perseveration | .14 | .27** | .09 |
| Sensory Sensitivity | −.35** | −.34** | −.12 |
| Emotional Reactivity | .23** | .21* | .23** |
| Endurance | −.09 | −.04 | −.11 |
| Activity | −.18* | −.04 | −.13 |
| Perceived Support | .23* | .07 | −.17* |
| Need for Support | .09 | −.07 | .03 |
| Support Seeking | .27** | .21* | −.15 |
| Actually Received Support | .18* | .11 | −.24** |
Note.
To determine the extent to which the studied variables can be viewed as predictors of the global trauma score (treated as the explained variable) in the patient groups, we conducted three hierarchical regression analyses for each patient group. We selected predictor variables to the regression equation basing on the second and third hypothesis of our study and we entered them into the models using the enter method. Therefore, we incorporated temperament traits in the first step and social support dimensions in the next step. In each step the significance of the increment in the explained variance was assessed on the basis of the F-change indicator. In order to assess multicollinearity, we computed variance inflation factors for all predictors in three regression models. None of the values exceeded the cut-off value of 10. The maximum achieved value was 1.99. It means that multicollinearity of predictors did not disturb the regression models (Kutner, Nachtsheim, & Neter, 2004).
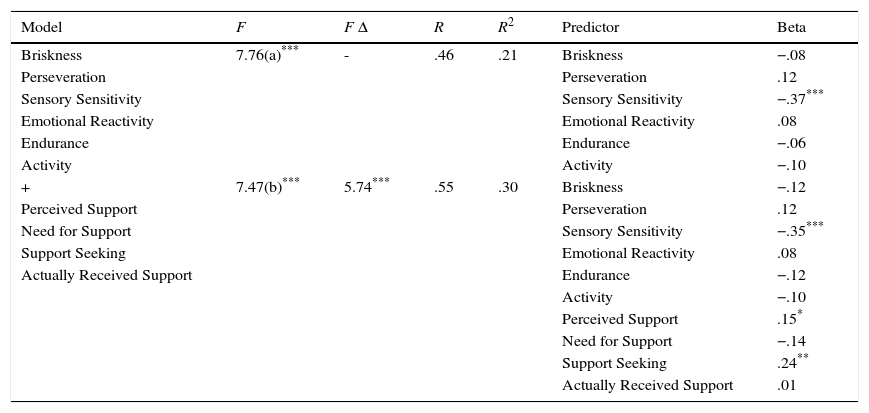
We noticed, on the one hand, a positive relationship between support seeking and perceived support and, on the other hand, a negative relationship between sensory sensitivity and the global trauma score among HIV+ patients. The model explained 30% of variance of the explained variable.
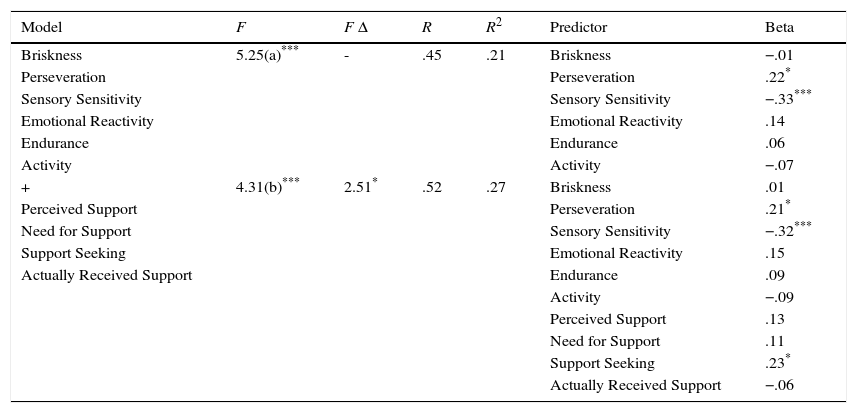
We found, on the one hand, a positive relationship between perseveration and support seeking and, on the other hand, a negative relationship between sensory sensitivity and the global trauma score among AIDS patients. The model explained 27% of variance of the explained variable.
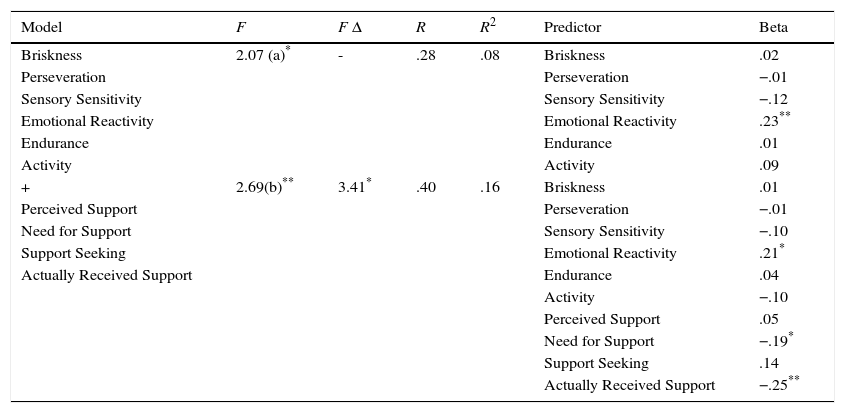
We observed, on the one hand, a positive relationship between emotional reactivity and, on the other hand, a negative relationship between actually received support and need for support and the global trauma score among RA patients. The model explained 16% of variance of the explained variable.
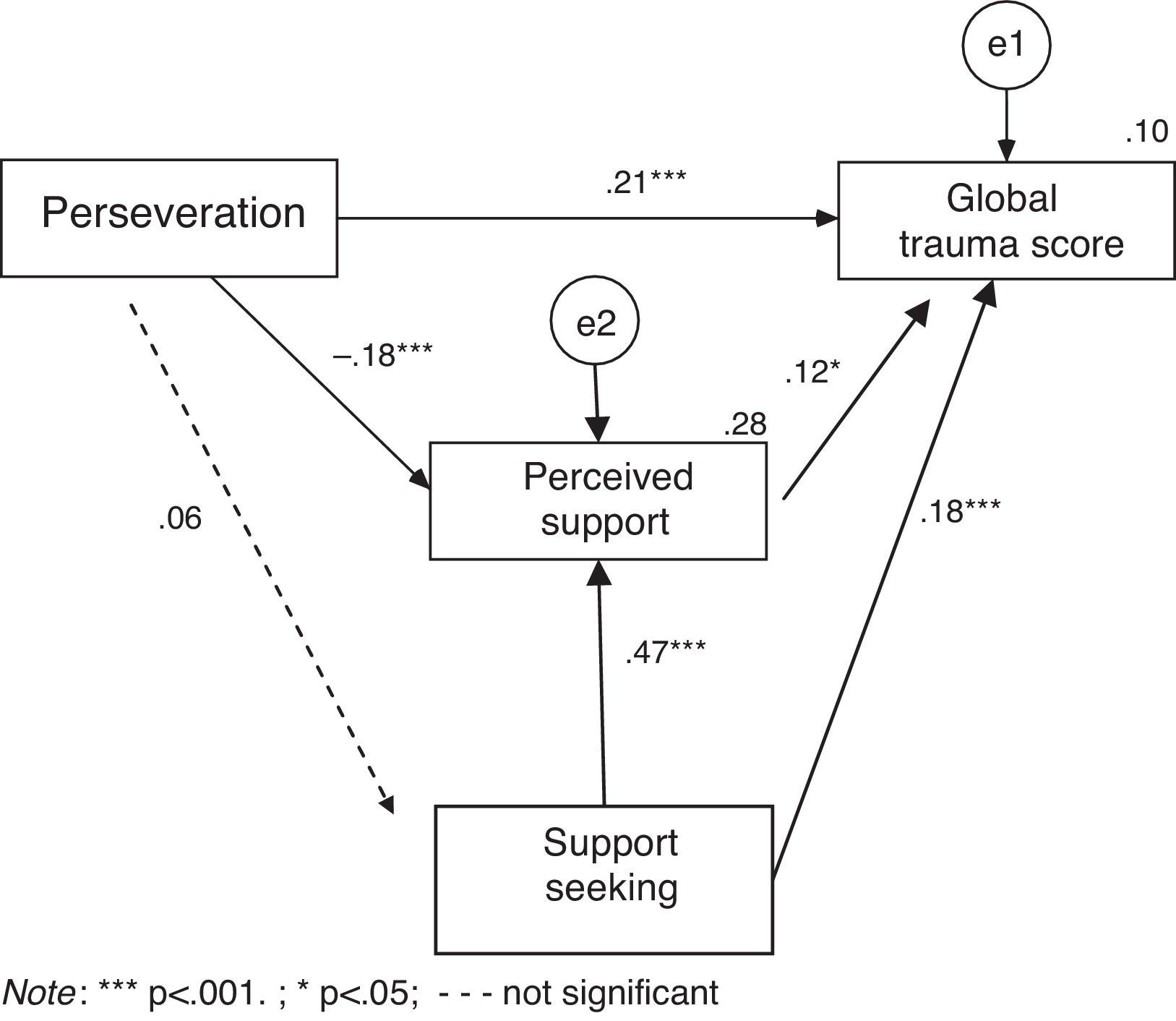
Finally, we decided to investigate an indirect link between temperament traits, social support and the global trauma score among HIV/AIDS and RA patients. First, the AMOS graphics program was used in order to create an input path diagram representing the relationship between the level of perseveration, perceived support, support seeking and the global trauma score, which was treated as an explained variable, in the entire sample of HIV/AIDS patients. Perseveration was treated as an exogenous variable and the calculations were conducted based on the maximum likelihood method. The goodness of fit given by the chi2 value indicates that the model did not differ significantly from the obtained data (χ2 = 0.93; df = 1; p>.05). The values of other goodness of fit indices suggested that the model fit was very good (CFI= .999; RMSEA = .001). We found the perceived support to be a partial mediator between perseveration and global trauma score. The Sobel test was statistically significant, Z = 2.276; p<.05. In addition, support seeking increased the level of global trauma score and the level of perceived support. All three predictors explained 10% of the variance of the explained variable.
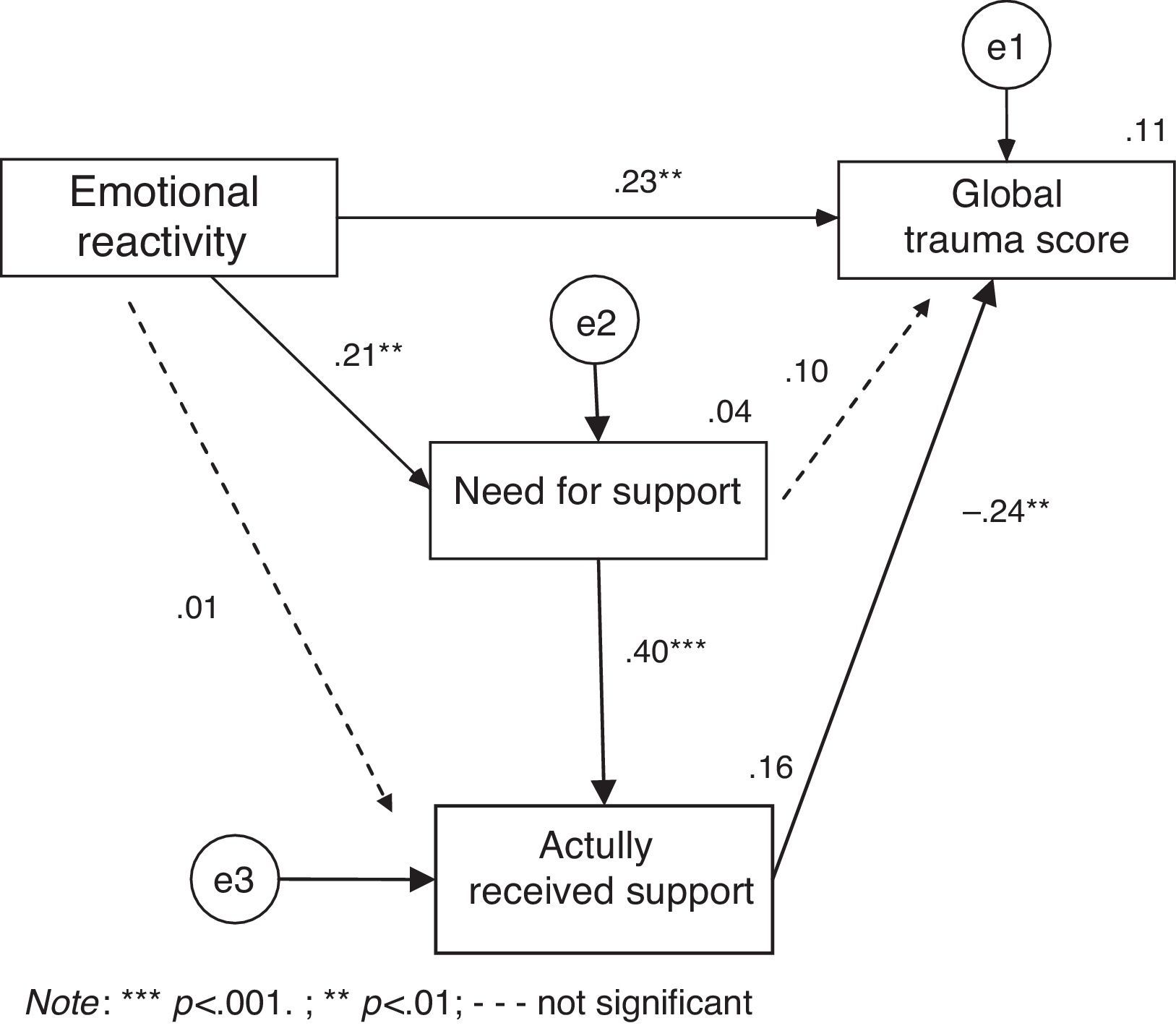
Second, the AMOS graphics program was used in order to create an input path diagram representing the relationship between the level the emotional reactivity, need for support, actually received support and the global trauma score, which was treated as an explained variable, in the sample of RA patients. Emotional reactivity was treated as an exogenous variable and the calculations were conducted based on the maximum likelihood method. The goodness of fit given by the chi2 value indicates that the model did not differ significantly from the obtained data (χ2 = 2.41; df = 2; p>.05). The values of other goodness of fit indices suggested that the model fit was very good (CFI= .991; RMSEA = .037). On the one hand, emotional reactivity increased the level of the global trauma score. On the other hand, emotional reactivity increased the need for support, which intensified the level of actually received support, which, in turn, decreased the level of global trauma score. All three predictors explained 11% of the variance of the explained variable.
DiscussionFirstly, we noticed significant differences in respect to some temperament traits, social support scales, and trauma symptoms between the HIV/AIDS sample and RA patients (see Table 1), which was in line with the first hypothesis. The most interesting fact is that HIV/AIDS individuals presented significantly lower social support levels compared to RA patients. At the same time, HIV+ (not AIDS) patients had a significantly lower level of intrusion/arousal symptoms compared to individuals with RA. It seems that the differences in social support may be attributed to intensive social stigmatization of HIV/AIDS people (Breet et al., 2014), which is not experienced to such an extent by people suffering from RA. Moreover, it is worth mentioning that the results obtained for the PTSD-F scales among all patient groups do not appear to differ markedly from the results obtained by Strelau et al. (2002) for the original scale.
In addition, the results of our study showed that emotional reactivity (RA patients) and perseveration (AIDS patients) were positively, whereas sensory sensitivity (HIV+ and AIDS patients) was negatively related to the global trauma score among our participants (see Tables 2, 3, 4, and 5), which corresponds substantially with the second hypothesis. In searching for a general mechanism that may explain these results, the “temperament–stress” relationship model is worth mentioning, in which temperament is a stress moderator (Strelau, 2008). In other words, temperament affects the state of stress as well as its consequences, thus influencing outcomes such as level of performance or ways of coping. Temperament traits from RTT affect an individual level of activation and self-regulatory functions, which are often deregulated among people suffering from trauma symptoms (Strelau & Zawadzki, 2005). In particular, emotional reactivity was again positively related to trauma symptoms intensity (Strelau, 2008). This trait is described as high sensitivity and low emotional resistance and correlates with other personality traits that are predictors of trauma symptoms, such as neuroticism, introversion, anxiety, and harm avoidance (Hornowska, 2011). Likewise, perseveration, which is a tendency to maintain and repeat behaviours and to experience emotional states following a cessation of the stimuli evoking these behaviours or states, is also positively correlated with the above-mentioned personality predictors of trauma symptoms (Strelau & Zawadzki, 2005). Perseveration also appeared to be a predictor of illness-related outcomes and somatic anxiety in various patients groups (Fruehstorfer, Veronie, Cremeans-Smith, & Newberry, 2012). Conversely, sensory sensitivity was negatively related to the trauma symptoms in our participants. Sensory sensitivity is one's ability to perceive stimuli and then to regulate their response to stimuli by either seeking out further stimulation or removing excessive stimulation depending on the strength of the stimuli. HIV/AIDS individuals often experience internal arousal caused by HIV-related physical symptoms and, at the same time, increased isolation related to social stigmatisation, which may deprive them of external stimulation and cause depression and trauma symptoms (Breet et al., 2014). In this context, intensification of sensory sensitivity may compensate for these processes by restoring effective stimulation regulation and self-regulatory functions.
Hierarchical regression analysis of temperament traits and social support scales as predictors of Global Trauma Symptoms in the HIV+ sample (n = 182).
| Model | F | F Δ | R | R2 | Predictor | Beta |
|---|---|---|---|---|---|---|
| Briskness | 7.76(a)*** | - | .46 | .21 | Briskness | −.08 |
| Perseveration | Perseveration | .12 | ||||
| Sensory Sensitivity | Sensory Sensitivity | −.37*** | ||||
| Emotional Reactivity | Emotional Reactivity | .08 | ||||
| Endurance | Endurance | −.06 | ||||
| Activity | Activity | −.10 | ||||
| + | 7.47(b)*** | 5.74*** | .55 | .30 | Briskness | −.12 |
| Perceived Support | Perseveration | .12 | ||||
| Need for Support | Sensory Sensitivity | −.35*** | ||||
| Support Seeking | Emotional Reactivity | .08 | ||||
| Actually Received Support | Endurance | −.12 | ||||
| Activity | −.10 | |||||
| Perceived Support | .15* | |||||
| Need for Support | −.14 | |||||
| Support Seeking | .24** | |||||
| Actually Received Support | .01 |
Note. (a) df = 6/175; (b) df = 4/171.
Hierarchical Regression Analysis of, Temperament Traits and Social Support Scales as Predictors of Global Trauma Symptoms in the AIDS Sample (n = 128).
| Model | F | F Δ | R | R2 | Predictor | Beta |
|---|---|---|---|---|---|---|
| Briskness | 5.25(a)*** | - | .45 | .21 | Briskness | −.01 |
| Perseveration | Perseveration | .22* | ||||
| Sensory Sensitivity | Sensory Sensitivity | −.33*** | ||||
| Emotional Reactivity | Emotional Reactivity | .14 | ||||
| Endurance | Endurance | .06 | ||||
| Activity | Activity | −.07 | ||||
| + | 4.31(b)*** | 2.51* | .52 | .27 | Briskness | .01 |
| Perceived Support | Perseveration | .21* | ||||
| Need for Support | Sensory Sensitivity | −.32*** | ||||
| Support Seeking | Emotional Reactivity | .15 | ||||
| Actually Received Support | Endurance | .09 | ||||
| Activity | −.09 | |||||
| Perceived Support | .13 | |||||
| Need for Support | .11 | |||||
| Support Seeking | .23* | |||||
| Actually Received Support | −.06 |
Note. (a) df = 6/121; (b) df = 4/117.
Hierarchical regression analysis of temperament traits and social support scales as predictors of Global Trauma Symptoms in the rheumatoid arthritis sample (n = 150).
| Model | F | F Δ | R | R2 | Predictor | Beta |
|---|---|---|---|---|---|---|
| Briskness | 2.07 (a)* | - | .28 | .08 | Briskness | .02 |
| Perseveration | Perseveration | −.01 | ||||
| Sensory Sensitivity | Sensory Sensitivity | −.12 | ||||
| Emotional Reactivity | Emotional Reactivity | .23** | ||||
| Endurance | Endurance | .01 | ||||
| Activity | Activity | .09 | ||||
| + | 2.69(b)** | 3.41* | .40 | .16 | Briskness | .01 |
| Perceived Support | Perseveration | −.01 | ||||
| Need for Support | Sensory Sensitivity | −.10 | ||||
| Support Seeking | Emotional Reactivity | .21* | ||||
| Actually Received Support | Endurance | .04 | ||||
| Activity | −.10 | |||||
| Perceived Support | .05 | |||||
| Need for Support | −.19* | |||||
| Support Seeking | .14 | |||||
| Actually Received Support | −.25** |
Note. (a) df = 6/143; (b) df = 4/139.
Furthermore, our study provided an interesting insight into the link between social support and trauma symptoms (see Tables 2, 3, 4, and 5). Whereas actually received support and need for support were negatively related to the global trauma score in RA patients, which was in line with our third hypothesis, support seeking (HIV+ and AIDS) and perceived support (HIV+) were positively associated with the level of trauma symptoms in the HIV/AIDS sample, which contradicted our third hypothesis. In addition, social support occurred to be a mediator variable in the association among temperament traits and trauma symptoms in our participants (see Figures 1 and 2). Several authors have shown, on the one hand, a positive association between social support and good physical and psychological functioning among chronic pain patients, and, on the other hand, a significant relationship between a lack of social support and exacerbation of pain, disability, and psychological disorders (Evers, Kraaimaat, Geenen, Jacobs, & Biglsma, 2003). In a related sense, HIV/AIDS individuals experience intensive social stigmatization, which disrupts their existing social status and prevents them from seeking treatment (Breet et al., 2014). Furthermore, the disclosure of HIV status may lead to rejection and discrimination, as HIV still evokes many negative stereotypes (Theuninck et al., 2010). Negative attitudes toward HIV+ people increase with the increasing number of physical symptoms of HIV infection (Cohen, Harezlak, Schifitto, Hana, & Clark, 2010). All the above-mentioned factors may explain why support seeking and perceived support were positively related to the level of trauma symptoms in the HIV/AIDS sample.
. Note. *** p < .001; * p < .05; - - - not significant.")
. Note. *** p < .001; ** p < .01; - - - not significant.")
Our study is not free of limitations. Firstly, the cross-sectional design of the study is inherently limited in understanding causal processes; i.e., we cannot directly state whether trauma symptoms, temperament, and social support were modified during the course of disease in our participants. Secondly, we did not investigate other social support dimensions (e.g., those who provided social support) that may be related to trauma symptoms in participants. Finally, we did not thoroughly examine demographic characteristics and some medical issues related to the course of disease in our participants (e.g., the year of diagnosis; length of disease, especially the AIDS phase or medical treatment). Aforementioned factors should be taken into in account in the future studies dedicated to the problematic described in this study.
Despite these limitations, our research provided new insight into the psychosocial aspects of living with HIV/AIDS and chronic pain. The importance of trauma symptoms, as well as their temperamental and social determinants should be taken into account in planning the forms of psychological support that should accompany pharmacotherapy for HIV/AIDS and chronic pain patients. However, the awareness of the association between trauma symptoms, and experiencing medical conditions among mental health care remains still limited (Sartorius, Holt, & Maj, 2015). Therefore, it is important to increase mental health providers’ awareness of the risk of medical-illness related trauma symptoms. In the face of the constant difficulties modern medicine has with a completely successful treatment of HIV+ individuals and RA patients and, it seems that continuing research, such as the research described in this manuscript, is justified.
This work was supported by the University of Warsaw, Faculty of Psychology (Grant BST 1712 – 2014). The authors declare no conflict of interest.
