



Depression represents a leading cause of disability and a major contributor to the overall global burden of disease with women systematically reporting a higher prevalence than men. This study aimed to examine the predictive value and relation of three transdiagnostic psychological factors (perceived stress, psychological inflexibility and loneliness) on depression and its sex differences for the general population in a large sample of Ecuador.
MethodA non-probabilistic and non-clinical sample of 16.074 people from across Ecuador were online surveyed using a cross-sectional design. The structural equation model was based on scores from standardized questionnaires as measures of depression, psychological perceived stress, psychological inflexibility, and loneliness.
ResultsWomen reported significantly higher levels of depression, mediated by differences in perceived stress, psychological inflexibility and loneliness. Perceived stress was the most important predictor of depression and mediated the effect of loneliness on depression. Complementarily, psychological inflexibility partially mediated the effect of perceived stress and loneliness on depression. The overall model accounted for the 78% of the total variance in depression.
ConclusionsResults of this study provide a novel and robust transdiagnostic model of sex differences on depression and insights on how to design effective programs for preventing depression targeting modifiable transdiagnostic risk factors.
Depression is a common illness worldwide, with an estimated 3.8% of the population affected, and more prevalent in women than men (World Health Organization [WHO], 2021). It is also a leading cause of disability and a major contributor to the overall global burden of disease (Moussavi et al., 2007; WHO, 2021). In Latin America, Ecuador is one of the countries with the highest rates of depression (Pan American Health Organization, 2018), therefore, the development of cost-effective interventions for depression represents a priority (Kohn et al., 2018) and global target (WHO, 2013). Moreover, the COVID-19 pandemic has aggravated the situation in Ecuador (González-Andrade, 2022; Killgore, Cloonen, Taylor & Dailey, 2020; Our World in Data, 2019).
Transdiagnostic models of mental health problems are becoming increasingly prominent focusing on underlying fundamental processes involved in multiple conditions, as transdiagnostic risk factors may account for comorbidities (Carragher, Krueger, Eaton & Slade, 2015; Dalgleish, Black, Johnston & Bevan, 2020; Nolen-Hoeksema & Watkins, 2011), leading to multiple conditions (multifinality) or divergent trajectories (Levine, Tabri & Milyavskaya, 2021; Mansell, Harvey, Watkins & Shafran, 2009; Nolen-Hoeksema & Watkins, 2011). This approach is particularly important in low and middle-income countries, where access and availability of specialized professionals and treatments are scarce (Evans-Lacko et al., 2018), in addition to the current and widespread concern about the overprescription of antidepressants and anxiolytics (WHO, 2021).
Previous studies from fields of health and clinical psychology have suggested that at least three important transdiagnostic variables might be involved in depression: (1) Psychological stress, defined as the degree to which people feel that the demands in their lives exceed their abilities to cope effectively (Cohen, Gianaros & Manuck, 2016); (2) Psychological inflexibility, defined as a pattern in which behavior excessively controlled by one's thoughts and feelings, where individuals seek to avoid, scape, or otherwise control their occurrence, despite their harmful consequences or at the expense of more effective and meaningful actions (Bond et al., 2011; Levin et al., 2014); and (3) Loneliness, that refers to the perception of mismatch between the quantity or quality of meaningful relationships an individual has and the relationships one desires (Cacioppo & Cacioppo, 2018; Cacioppo et al., 2006). In this sense, loneliness or perceived social isolation is distinctive from being physically alone. However, despite the importance of such variables, the relationship between these transdiagnostic variables in depression by sex remains unclear.
The aim of this study was to develop a transdiagnostic model of the risk of depression and its sex differences, analyzing the relations between perceived stress, psychological inflexibility and loneliness, in a large sample of Ecuadorian adults from the general population.
MethodsParticipantsA non-probabilistic and non-clinical sample of 20.036 adults across Ecuador were online surveyed. Participants were recruited in two ways: first, via advertisements from the Ministry of Public Health, the Secretariat of Higher Education, Science, Technology and Innovation of Ecuador (Secretaría de Educación Superior, Ciencia, Tecnología e Innovación, SENESCYT-SGES-SIES-2021–1156-O) and 48 public and private institutions of Higher Education in Ecuador displayed in their websites on our request; second, from email invitations received after attending a series of webinars organized on October 10th, 2021, for the commemoration of the World Mental Health Day. Data were collected for three months, from October 2021 to January 2022. Participants received no economic compensation for their participation. Those who failed to complete the survey were removed, resulting a final sample size of 16.074 participants. No additional cases or items were removed afterwards. The final sample was composed of 53.2% men. Participants were geographically distributed across Ecuador as follows: 60.9% from the central region, 30.2% from the West coast region, 8.7% from East Amazonian region, and 0.2% from Galapagos Islands. Mean age was 30.91 years (SD = 10.05; ranging from 18 to 72 years old). Most participants were single (54.3%), then married (40.1%) or separated/divorced/widowed (5.6%). Additionally, most participants reported a full-time job (56%), then unemployed (27.7%) or a partial-time job (16.3%).
MeasuresSociodemographic data. This section included information regarding basic sociodemographic data, such as age, sex, marital status, geographic region, and employment status.
Patient Health Questionnaire-9 (PHQ; Kroenke, Spitzer & Williams, 2001; Ecuadorian adaptation by López-Guerra et al., 2022). PHQ-9 represents a self-reported questionnaire that measures depressive symptomatology for Major Depressive Disorder. It consists of 9 items and participants respond in a 4-point scale (0 = “not at all”; 1 = “several days”; 2 = “more than half the days”; 3 = “nearly every day”). Scores range from 0 to 27 where higher scores indicate more severe depressive symptoms. An example item of the scale is: “Trouble falling or staying asleep or sleeping too much”. The internal consistency for this study was high, with a Cronbach's α = 0.94.
Perceived Stress Scale (PSS-10; Cohen, Kamarck & Mermelstein, 1983; Ecuadorian adaptation by Ruisoto, López-Guerra, Paladines, Vaca & Cacho, 2020). PSS-10 consists of a 10-item scale that evaluates the degree to which people perceive a lack of control in their daily lives. Participants should respond to a 5-point Likert-type scale, ranging from 0 (“never”) to 4 (“very often”). Higher scores indicate higher levels of psychological stress. Scores range from 0 to 40 points. The questionnaire showed good internal consistency, with a Cronbach's α = 0.85 and a bifactorial structure. An example item would be “In the last month, how often have you felt nervous and “stressed”?”.
Acceptance and Commitment Questionnaire (AAQ-II; Bond et al., 2011; Ecuadorian version by Paladines-Costa, López-Guerra, Ruisoto, Vaca-Gallegos & Cacho, 2021). It is the most widely used general measure of psychological inflexibility and includes 7 items, to which participants must respond in a 7-point Likert-type scale, ranging from 1 = “never” to 7 = “always”. Higher scores indicate a tendency to act under the need to control or avoid aversive thoughts, memories or feelings. The following item represents an example of this scale: “I worry about not being able to control my worries and feelings”. The internal consistency for this study was high, with a Cronbach's α = 0.96.
Loneliness Scale Revised-Short (UCLA) (Hughes, Waite, Hawkley & Cacioppo, 2004; Russell, 1996). This scale assesses the subjective feeling of loneliness, understood as the perception of less social support being available tan desired. Participants respond based on their agreement with a series of statements, where 1 = “hardly ever”, 2 = “sometimes”, and 3 = “often”. Higher scores indicate a greater feeling of loneliness or lack of social support. An example item is “How often do you feel that you lack companionship?”. Internal consistency for this study was good, with a Cronbach's α = 0.85.
Design and procedureA cross-sectional study was conducted. The study was approved by the Ethics Committee for Research in Human Beings (Comité de Ética de Investigación en Seres Humanos, CEISH) of the Universidad San Francisco de Quito (USFQ) in August 2021 (CEISH: 2021–072E), supported by the Ecuador´s Ministry of Public Health, and conducted according to the principles expressed in the Declaration of Helsinki (World Medical Association [WMA], 2013). All participants provided individual consent to voluntarily participate in the study.
Data analysisThe statistical analyses were carried out using the IBM Statistical Package for the Social Sciences (SPSS) software (IBM Inc., Chicago, IL, USA; version 26.0). For all measures, means (M) and standard deviation (SD) were used when normality, asymmetry and kurtosis was met as tested using Kolmogorov-Smirnov test. On the other hand, Levene´s test was used to analyze homocedasticity. We used Student´s t-test to examine the sex differences in the main outcome variables, and Cohen´s d to measure effect sizes with values of 0.15, 0.40, and 0.75 as thresholds to interpret small, medium, and large effects (Gignac & Szodorai, 2016). Variance Inflaction Factor (VIF) was used for detecting multicollinearity with a cut off above 5 (Sheather, 2009).
Relationships between transdiagnostic variables were examined using a model of structural equations by means of the maximum likelihood method with AMOS (IBM 228 Inc., Armonk, NY, USA; version 25.0). The following goodness-of-fit estimators were used: χ2 by degrees of freedom (CMIN/DF), Bentler comparative fit index (CFI), Tucker–Lewis Index (TLI), Goodness of Fit Index (GFI), Bentler-Bonnet Normed Fit Index (NFI), Adjusted Goodness of Fit Index (AGFI) and the root mean square error of approximation (RMSEA). Following Byrne (2016), good fit was considered if CMIN/DF ≤ 2, CFI, TLI, GFI and NFI ≥ 0.95, AGFI ≥ 0.90 and RMSEA ≤ 0.05; acceptable if CMIN/DF ≤ 3, CFI, TLI, GFI and NFI ≥ 0.90, AGFI ≥ 0.85 and RMSEA < 0.08.
In addition, parsimony normed fit index (PNFI), parsimony comparative fit index (PCFI) and parsimony good of fitness index (PGFI) where used, considering a good parsimony-fit set by PNFI and PCFI ≥ 0.80, PGFI ≥ 0.70; and acceptable if PNFI and PCFI ≥ 0.60 and PGFI ≥ 0.50 (Byrne, 2016). The significance level was set at p < .05.
ResultsSample descriptionWomen reported significantly higher scores of depression (t(14,657) = 34.191, p < .001, d = 0.544), perceived stress (t(16,072) = 35.655, p < .001, d = 0.563), psychological inflexibility (t(14,657) = 39.043, p < .001, d = 0.621) and loneliness (t(14,657) = 29.746, p < .001, d = 0.469), than men (see Table 1).
Sex differences in transdiagnostic risk factors and depression.
Note: M = Mean; SD = Standard Deviation.
The three transdiagnostic variables significantly (p < .001) correlated with depression, as follows: perceived stress (r = 0.698), psychological inflexibility (r = 0.784), and loneliness (r = 0.669). VIF ranged between 1 and 2.8, below the cut-off point of 5 required for multicollinearity.
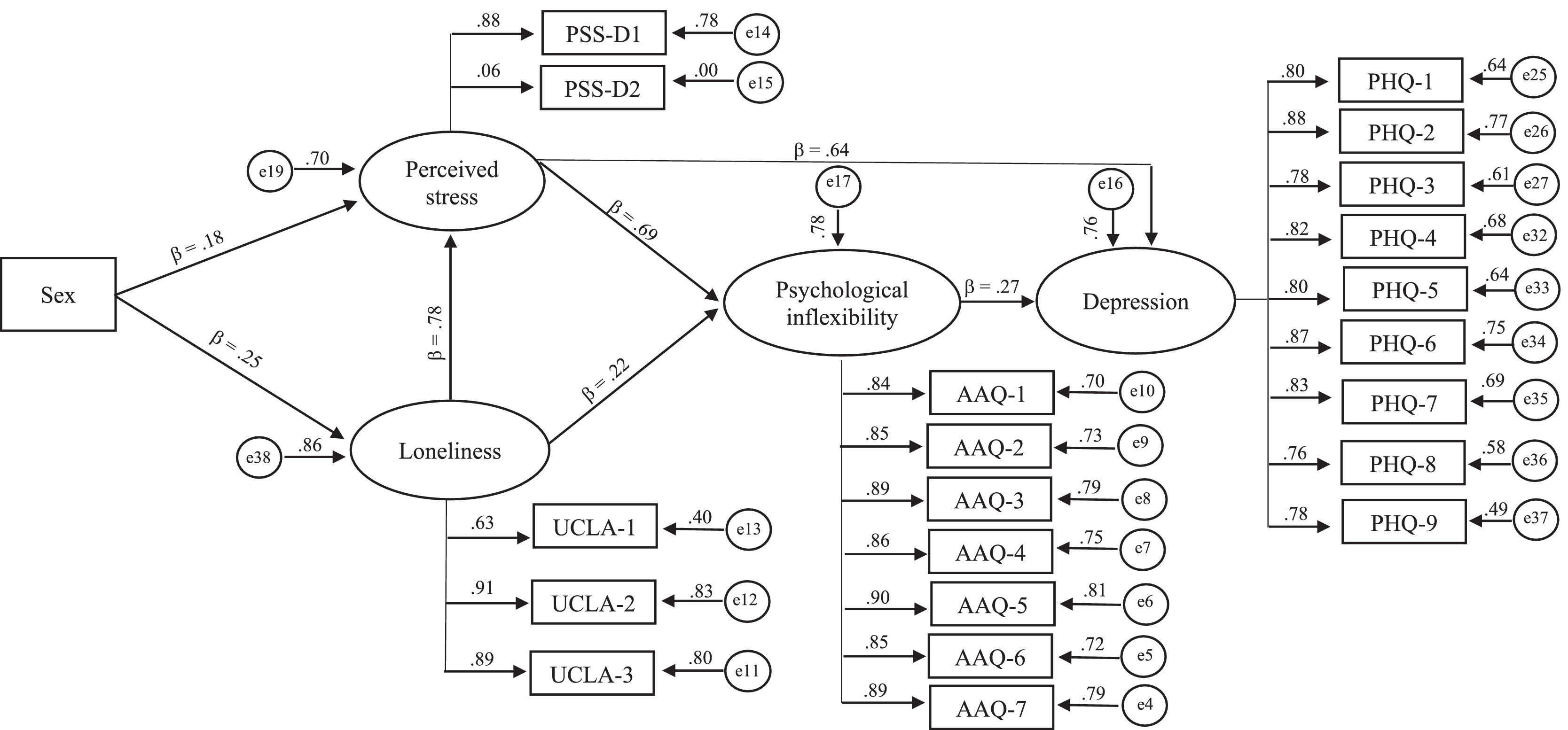
Transdiagnostic model of sex differences in depressionFirst, based on the transdiagnostic model, perceived stress was the single best predictor of depression and mediated the effect of loneliness on depression (see Fig. 1). Second, psychological inflexibility mediated the effect of perceived stress and loneliness on depression. Third, a closer look to the perceived stress scores revealed two latent dimensions: perceived helplessness (items 1, 2, 3, 6, 9 and 10, corresponding to PSS-D1 in Fig. 1) and perceived self-efficacy (items 4, 5, 7 and 8, corresponding to PSS-D2 in Fig. 1), where only the former was a significant predictor of depression. Regarding the strength of the effect of each individual transdiagnostic risk factor on depression, it is worth mentioning the weight of loneliness on perceived stress, as well as the later on psychological inflexibility and depression. Individually, perceived stress, loneliness and psychological inflexibility accounted by the 70%, 86% and 78% respectively of the total variance in depression and, together, the relations between the three transdiagnostic variables accounted for up to 78% of the total variance in depression.
.")
Overall, the model showed good fit to the data based on the following indexes: CFI = 0.957; TLI = 0.95; GFI = 0.913; NFI = 0.951; AGFI = 0.891; RMSEA = 0.069; PNFI = 0.828; PCFI = 0.828 and PGFI = 0.726. On the other hand, CMIN/DF = 73.887 due to its high sensibility to large sample size (Hair, Black, Black, Babin & Anderson, 2010). Moreover, the overall model accounted for the 78% of the total variance in depression, and very large effect size was found, f2 = 3.54, following Cohen (1988).
DiscussionTo our knowledge, this is the first study that provides a novel and comprehensive model that integrate transdiagnostic risk factors involved in depression, from three different theoretical approaches: clinical psychology (psychological inflexibility), health psychology and behavioral medicine (perceived stress), and social neuroscience (loneliness). Moreover, this study provides a robust transdiagnostic model for accounting differences on depression fully driven by data (with no post hoc model modifications) from the largest sample size examined to date in Ecuador. This is important taking into account that Ecuador is one of the top-five countries in Latin America in rates of disability due to depression (Pan American Health Organization, 2018).
The following conclusions can be drawn for our transdiagnostic model of psychological factors and sex differences on depression:
Firstly, our study found medium to large sex differences on depression. This result is consistent with the current sex differences in the rates of depression reported in Ecuador, being 5.8% for women and 3.8% for men (WHO, 2015), supporting that women deserve special attention as a vulnerable population in this field as suggested by previous studies (Harkness et al., 2010; Heidari, Babor, De Castro, Tort & Curno, 2016; Kneavel, 2021). Moreover, a marked and systematic gap was reported between men and women for each of the three transdiagnostic risk factors integrated in the model, providing useful insights about source of these sex differences on depression.
Secondly, perceived stress represented the single best predictor of depression, a well-established finding in the scientific literature (Cristóbal-Narváez, Haro & Koyanagi, 2020; Yang et al., 2015). However, our study highlight that is helplessness, but not perceived self-efficacy, the main driver of the negative impact of stress on depression. This is consistent with the conceptualization of learned helplessness as behavioral and the most widely studied animal model of depression and used to test antidepressants (Maier & Seligman, 2016; Wang, Timberlake, Prall & Dwivedi, 2017). This outcome is important because highlight the importance of perceived control over our own lives. In this regard, two important implications can be drawn from these results: first, the nature of the perceived control relevant for depression is social, not personal, due to “self” efficacy fails to predict stress-induced depression. However, a more “social” helplessness account for the negative impact of perceived stress on depression. Second, consistent with these interpretations, loneliness or perceived social isolation represents a core stressor by itself, highlighting the necessity for social connection to exert control over our lives. In this sense, higher risk of depression would be expected on the face of “social” adversities and “social” deprivations (Weil, 2020). Moreover, sex differences in perceived stress are also consistent with the higher prevalence of most of stress and anxiety disorders in women compared to men (Gradus, 2017; Remes, Brayne, van der Linde & Lafortune, 2016). Scientific literature suggests at least two main interpretations on the source of these sex differences in perceived stress (Jick & Mitz, 1985). First, differences in the degree of pressure or strains experienced by men and women. For example, in general, women spend two to ten times more time on unpaid domestic and care work than men (Ferrant, Pesando & Nowacka, 2014), and these figures that may have aggravated during the COVID-19 pandemic (Xue & McMunn, 2021). Second, differences in the cognitive appraisal or coping behaviors between men and women. For example, women tend to report more sedentary and private activities such as reading to manage stress, while men tend to report more active and social physical activities such as exercising (Azevedo et al., 2007).
Thirdly, the negative effect of loneliness on depression is not only accounted by its role as a powerful stressor of a social nature, as previously suggested (Hawkley & Cacioppo, 2010; Heinrich & Gullone, 2006), but also by impairing our ability to deal with stressing adverse events, in line with recent studies (Hofmann & Hayes, 2019). In other words, it seems that loneliness increases the risk of a psychologically inflexible pattern of behavior characterized by seeking to avoid, scape, or control stressful thoughts and feelings despite their harmful consequences or at the expense of more effective and meaningful actions (Bond et al., 2011; Browning, Van Kirk & Krompinger, 2021; Levin et al., 2014). Moreover, consistent with this interpretation, perceived stress also increases the risk of psychological inflexibility, enhancing the risk of depression; in other words, psychological inflexibility accounted for a significant part of the impact of perceived stress on depression. This result is important because provides insights about the underling mechanisms involved in the negative impact of loneliness, a well-established risk factor for health, on depression (Holt-Lunstad, Smith, Baker, Harris & Stephenson, 2015; van Winkel et al., 2017).
Regarding sex differences in loneliness, they have usually been examined without a clear a priori theoretical hypothesis. The main line of reasoning hypothesizes that sex differences emerge in the adolescence, when men report a preference for spending time alone, so aloneness will not necessarily lead to loneliness (Maes, Qualter, Vanhalst, Van den Noortgate & Goossens, 2019). Also, in the context of the evolutionary theory of loneliness, by which loneliness serves as a warning system for missing social relationships and driving force to reconnect to significant others (Cacioppo et al., 2015), women might become more sensitive to interpersonal aspects of the social environment to develop desirable social relationships (Martel, 2013).
Altogether, the model illustrates a direct pathway of perceived stress on depression, as well as an indirect pathway of perceived stress and loneliness on depression via psychological inflexibility. Indeed, psychological flexibility worked as an effective stress-copying skills for effectively managing adverse internal events mediating the negative impact of both perception of lack of control (perceived stress) and loneliness (a core stressor for stress-related depression). This result is consistent with previous studies that highlight the importance of transdiagnostic risk factors on depression (Hamblen & Mueser, 2021). Furthermore, these results raise serious concerns about the implications of the COVID-19 pandemic, in terms of social lost and social restrictions associated with confinement and social distance measurements (Aknin et al., 2022; Bermejo-Franco et al., 2022; Palgi et al., 2020).
Several limitations of this study deserve attention. First, this is a cross-sectional study that prevent us from drawing cause-effect relations. Second, data collection is based on self-reported measures and therefore, subject to some inaccuracies due to memory bias. In spite of these limitations, the large sample and effect sizes reported within the model provide additional support of our findings.
In conclusion, the results of this study provide rationale and useful heuristic for developing more effective assessment and treatment of depression, targeting modifiable stress-related transdiagnostic risk factors such as psychological inflexibility and loneliness, particularly among women as a more vulnerable population. Overall, results support the social nature of depression and central role of process-based transdiagnostic risk factors (Hofmann & Hayes, 2019), supporting the need to move beyond biomedical approaches primarily focused on individual pharmacological interventions (Kendler, 2009; Remes, Mendes & Templeton, 2021). Regarding sex differences, although this study highlights the importance of social context, biological differences in stress sensitivity and response across lifespan should be further examined in future studies as part of our best efforts in mental health research (Bale & Epperson, 2015; Bangasser & Wiersielis, 2018; Wellman et al., 2018).
Conflict of interestThe authors declare that this study was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Author contributionsConceptualization, P.R. and V.L.-G.; methodology, formal analysis, investigation and data curation, P.R., V.L.-G., C.L.-N. and B.P.-C; writing—original draft preparation, P.R., C.L.-N., R.S.-P., B.P.-C and N.P.-C.; writing—review and editing, P-R., V.L.-G., C.L.-N.; project administration and funding acquisition, V.L.-G., B.P.-C, N.P-C. All authors have read and agreed to the published version of the manuscript.
FundingThe study was funded by the Particular Technical University of Loja (Ecuador) (PROY-INV-PSI2020–2781). Additional funding to P.R. was provided by the European Union – “NextGenerationEU” through the Grant for the Requalification of the Spanish University System for 2021–2023 at the Public University of Navarra (Resolution 1402/2021).
Authors would like to thank the Ecuador´s Ministry of Public Health for its collaboration in the dissemination of the survey and collection of population-data for this study.
