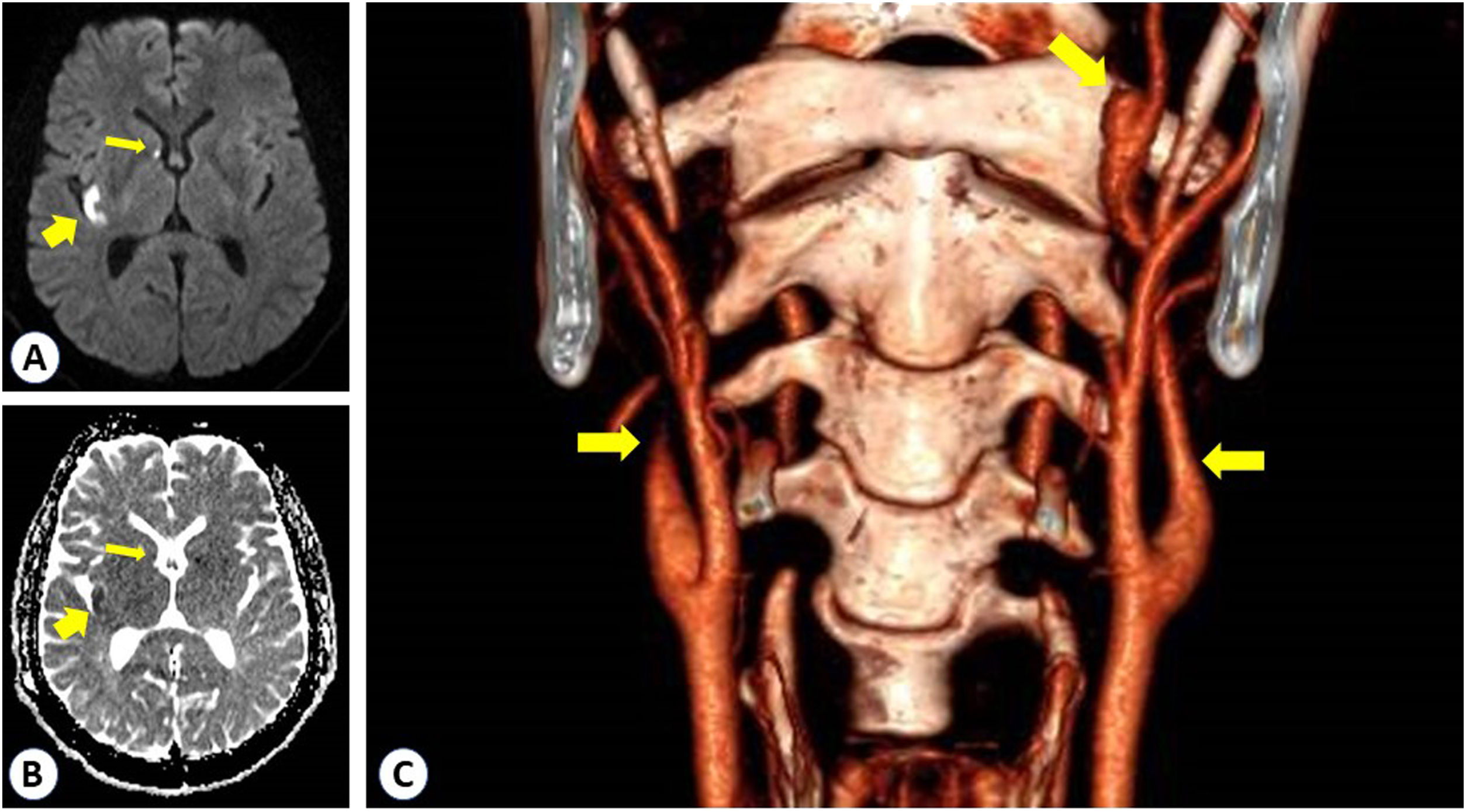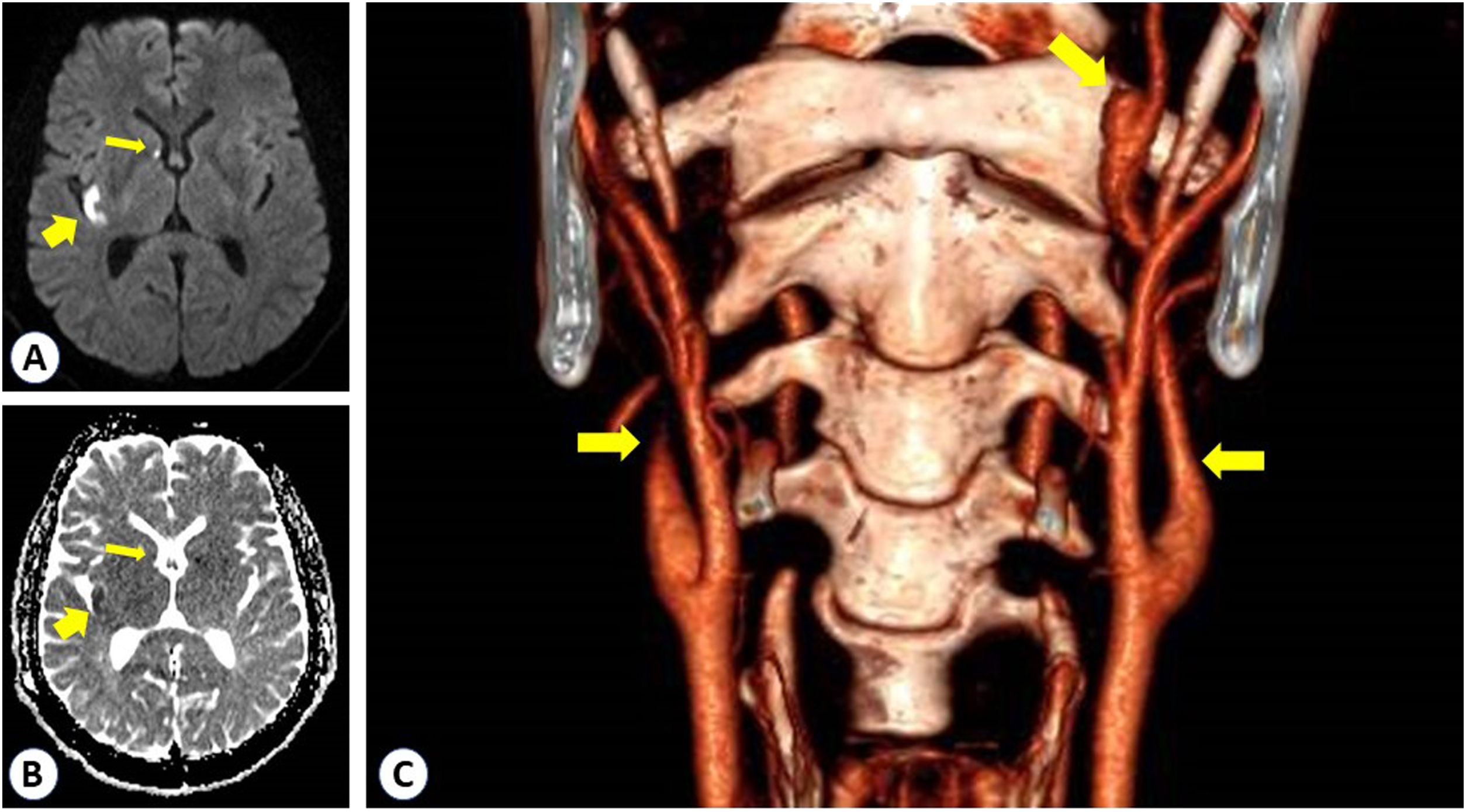
A male in his thirties presented to the emergency room referring a minute-long sudden-onset episode of inability to talk, lost look and paresthesia in the left upper extremity. He admitted a persistent harsh cough the previous days as sequel of a flu syndrome, but any relevant previous history. He showed two acute right hemispheric infarctions on MRI (arrows in panel A -DWI- and B -ADC map-). Angio-CT showed a typical beak sign in the right internal carotid artery (ICA) together with an abrupt narrowing on the left ICA immediately after inception with a distal pseudoaneurism; both consistent with dissections (arrows in panel C). A full cardiological and systemic work-up was negative. The genetic analysis performed in the following weeks revealed a pathogenic mutation in Exon 5 of the Col3A1 gen, consistent with Ehlers-Danlos type IV disease. No short or long-term recurrence was registered more than three years later.
Up to 20% of sporadic carotid artery diseases affect more than one vessel at onset or have early recurrence (8–12 weeks), and up to 1% may have an underlying genetic disease. The unique point comes from how the event constituted the clinical debut of an Ehlers-Danlos disease (Fig. 1).