



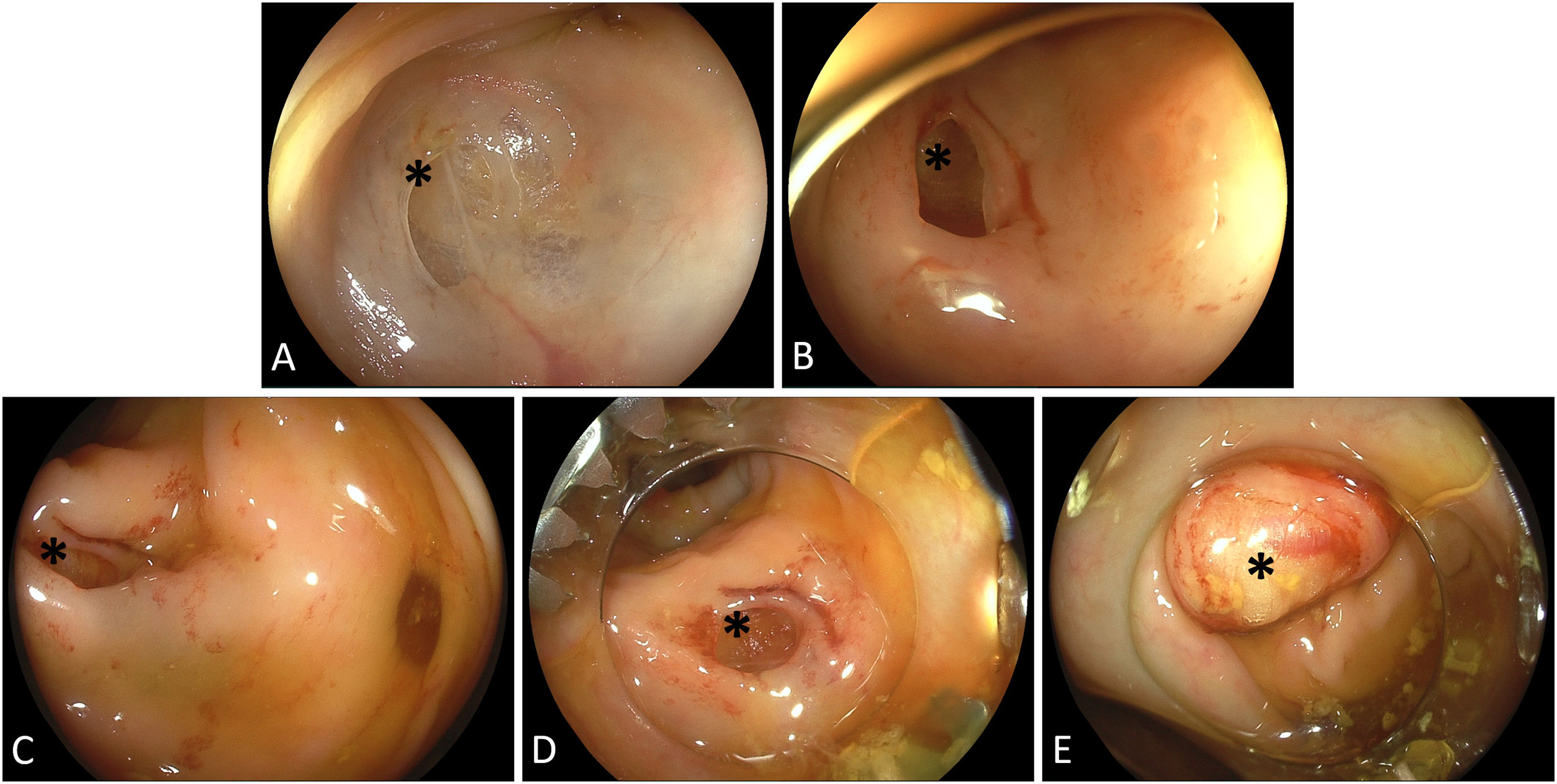
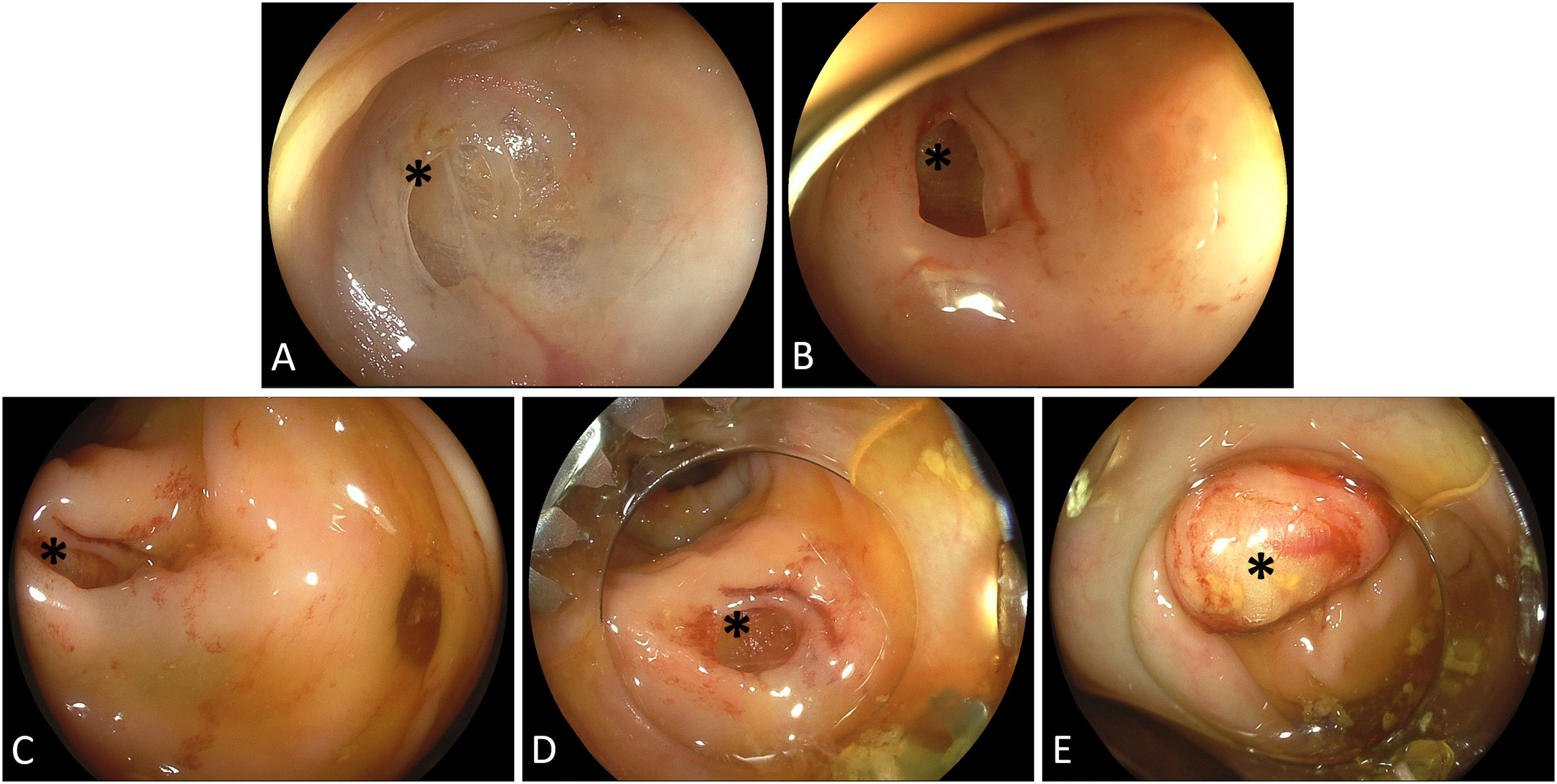
An 89-year-old male patient was admitted for anemia work-up and underwent colonoscopy in the further course to exclude colorectal cancer. In the lower sigmoid advancement of the colonoscope proved difficult due to diverticulosis and sharp angulations, resulting in transmural injury (Fig. 1A). Slight withdrawal of the tip of the scope confirmed an estimated 8-mm perforation with visible peritoneal fat (Fig. 1B). Whether or not the perforation occurred in a diverticula remained uncertain (Fig. 1C). Notwithstanding, after switching to CO2 insufflation and institution of broad-spectrum antibiotics, the scope was removed, and an over-the-scope clip (OTSC, Ovesco, Tübingen, Germany) device mounted. The perforation site was re-localized without difficulties (Fig. 1D). Next, the OTSC clip deployed in pure suction technique with an ancillary peritoneal fat patch sucked into the cap. Post-hoc visualization indicated circumferential capture of the defect margins with a central fat plombage (Fig. 1E). The patient took an uncomplicated clinical course and evacuation of minor gas peritoneum was not warranted in the stable, pain-free patient.
Perforation remains the Achilles heel in diagnostic and/or therapeutic gastrointestinal endoscopy. While formerly this implied surgical treatment, most perforations with intraprocedural appreciation can be managed by endoscopy nowadays with different techniques available including OTSC clips as a powerful tool for small- and moderate-size transmural defects.
