


Background: Indoor aeroallergens are the main cause of sensitization in children and represent a risk factor for the development of allergic diseases.
Objective: Identify the major indoor aeroallergens most often sensitized to pediatric patients treated at the Allergy Service at the “Dr. José Eleuterio González” University Hospital of Monterrey
Methods: We performed an observational and descriptive study where we reviewed reports of positive skin tests to the following common indoor aeroallergens: Dermatophagoides farinae (D. farinae), Dermatophagoides pteronyssinus (D. pteronyssinus), Canis familiaris (C. familiaris), Felis domesticus (F. domesticus), Blattella germanica (B. germanica) and Periplaneta americana (P. americana), found in patients under 16 years with symptoms of allergy, during the period of 2011-2012.
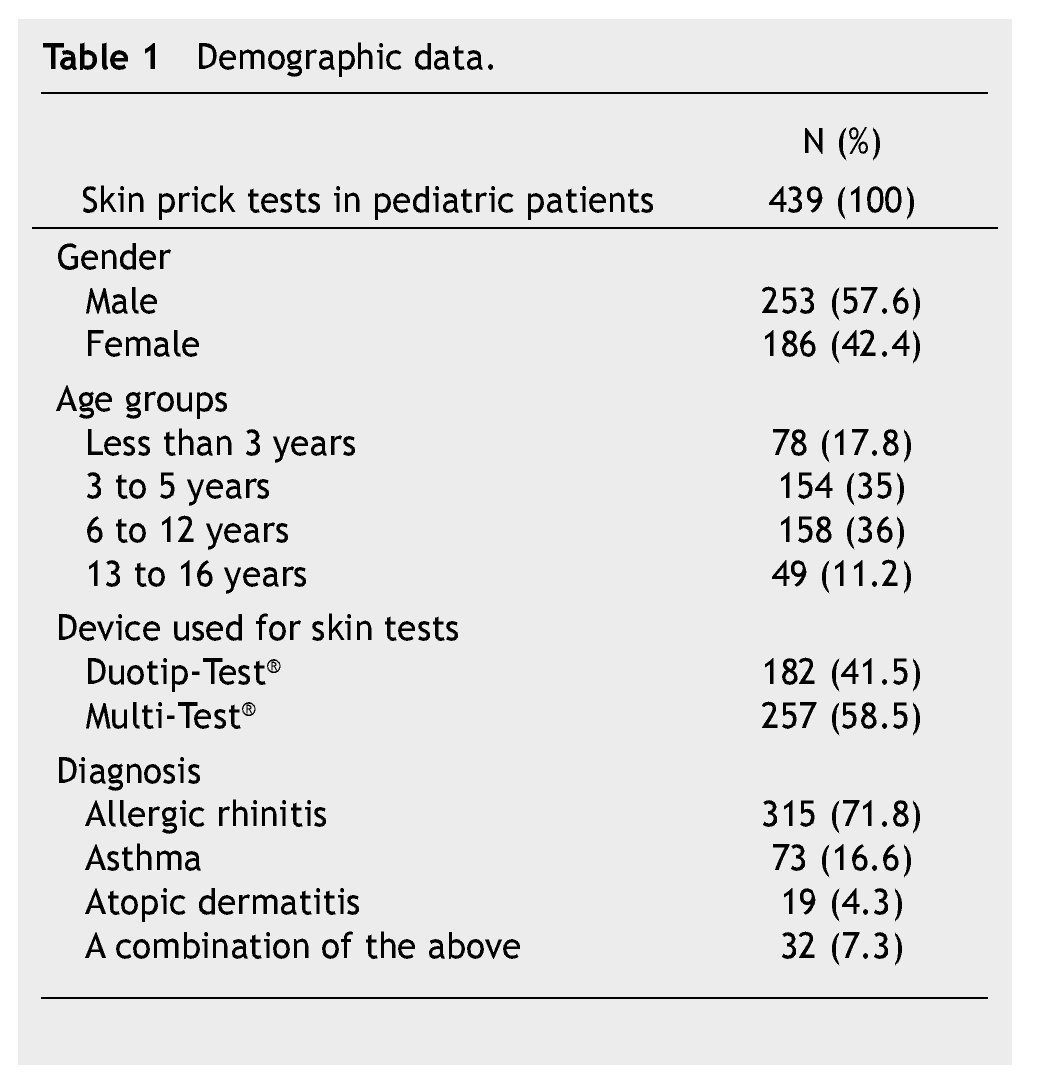
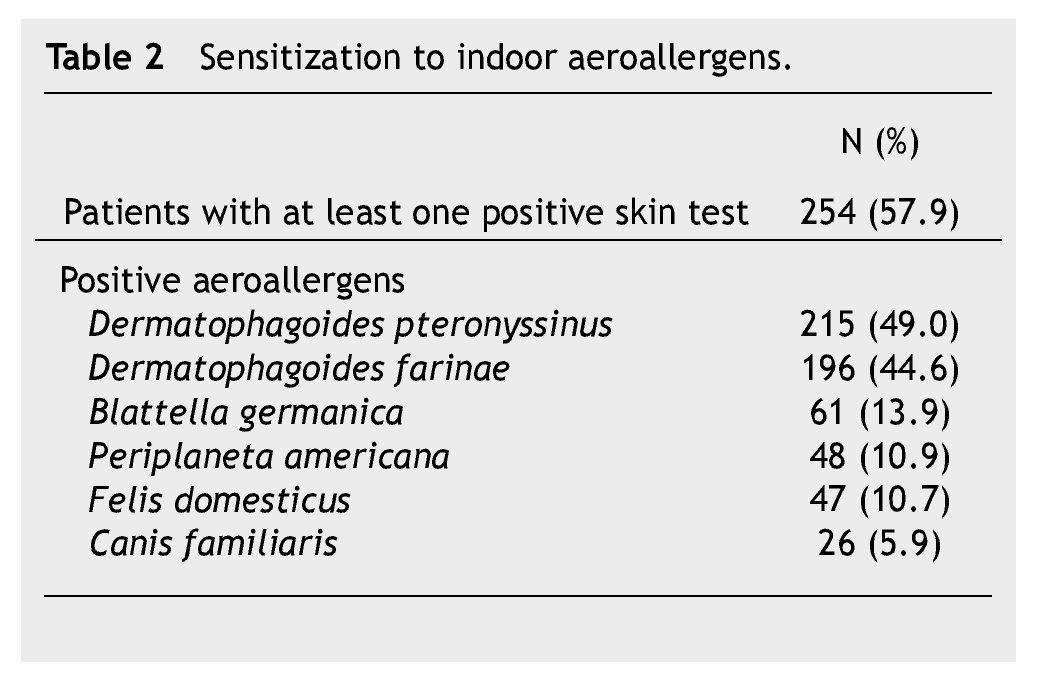
Results: We performed 439 skin tests to aeroallergens in pediatric patients. Of these, 57.6% were male and 42.4% were female. Mean age was 6.3 years. The age groups were under 3 years: 17.8%, 3-5 years: 35%, 6-12 years: 36%, and 13-16 years: 11.2%. The main diagnoses were: allergic rhinitis (71.8%), asthma (16.6%), and atopic dermatitis (4.3%). In 57.9% of the cases, they had at least one positive skin test to any aeroallergen. The rate of sensitization to specific aeroallergens was: D. Pteronyssinus 49.0%, D. farinae 44.6%, B. germanica 13.9%, P. Americana 10.9%, F. domesticus 10.7%, and C. familiaris 5.9%.
Conclusion: Indoor aeroallergen sensitization can occur early in life, although it was more frequent in the preschooler and elementary school group. Dust house mites were the most commom cause of allergic sensitization.
Introduction
The prevalence of organ-specific allergic diseases, such as allergic rhinitis, asthma and atopic dermatitis is on the rise worldwide.1 There is substantial evidence associating allergic sensitization and a hike in allergy and asthma morbidity to early exposure to environmental allergens.2 Atopic children usually begin with monosensitization (sensitization to a single allergen), however, with time they begin sensitizing to other allergens.3 Identification during the early stages of life is required in order to start a specific treatment and be able to modify the allergic disease’s natural history. Skin tests are used to assess Ige-mediated hypersensitivity, and confirm clinical sensitivity induced by allergens and other agents.4,5
The objective of this study was to identify the most frequent indoor aeroallergens which cause sensitization in children who attend the allergy outpatient clinic of “Dr. José Eleuterio González” University Hospital of the Universidad Autónoma de Nuevo León (UANL, by its Spanish acronym).
Methods
We conducted an observational and descriptive study. We reviewed the results of the skin tests for the most common indoor aeroallergens on children under 16 who went for a consult at the Allergy and Immunology Regional Center Clinic of “Dr. José Eleuterio González” University Hospital of the UANL, Mexico between 2011 and 2012.
We collected demographic data: age, gender, clinical diagnosis and skin test results for 6 common indoor aeroallergens: Dermatophagoides farinae (D. farinae), Dermatophagoides pteronyssinus (D. pteronyssinus), Canis familiaris (C. familiaris), Felis domesticus (F. domesticus), Blattella germanica (B. germanica) and Periplaneta americana (P. americana). Skin prick tests were performed using commercial allergen extracts, Duotip-Test® (Lincoln Diagnostics, Decatur, IL) or Multi-Test® (Lincoln Diagnostics, Decatur, IL), as well as a negative control with a saline solution of 0.9% and a positive one with 10 mg/mL of histamine. We considered a positive test that which caused a ≥ 3 mm wheal compared to the negative control.
The collected data was analyzed using Statistical Product and Service Solutions 17 (SPSS® Statistics v. 17.0). We evaluated nominal and ordinal variables, and determined frequencies and percentages.
Results
We evaluated a total of 439 skin tests to indoor aeroallergens in children under 16. The 57.6% of children were male and 42.4% female (Table 1). The most utilized device for skin tests was Multi-Test® (58.5%). On the other hand, Duotip-Test® was used in 41.5% of the cases. There were no reports of complications with either device.
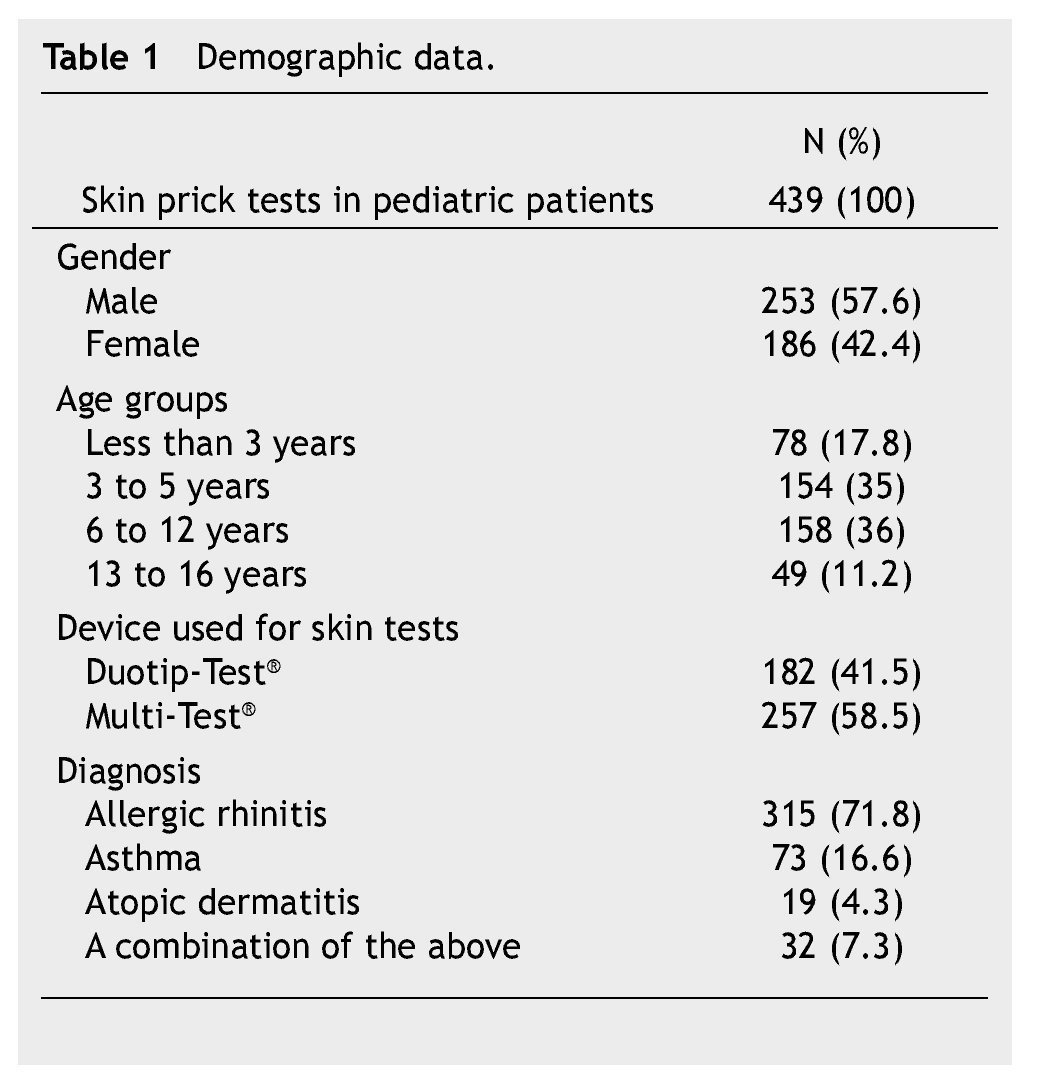
The clinical diagnoses included: allergic rhinitis (71.8%), asthma (16.6%), and atopic dermatitis (4.3%). The 7.3% of children had 2 or more of these allergic diseases.
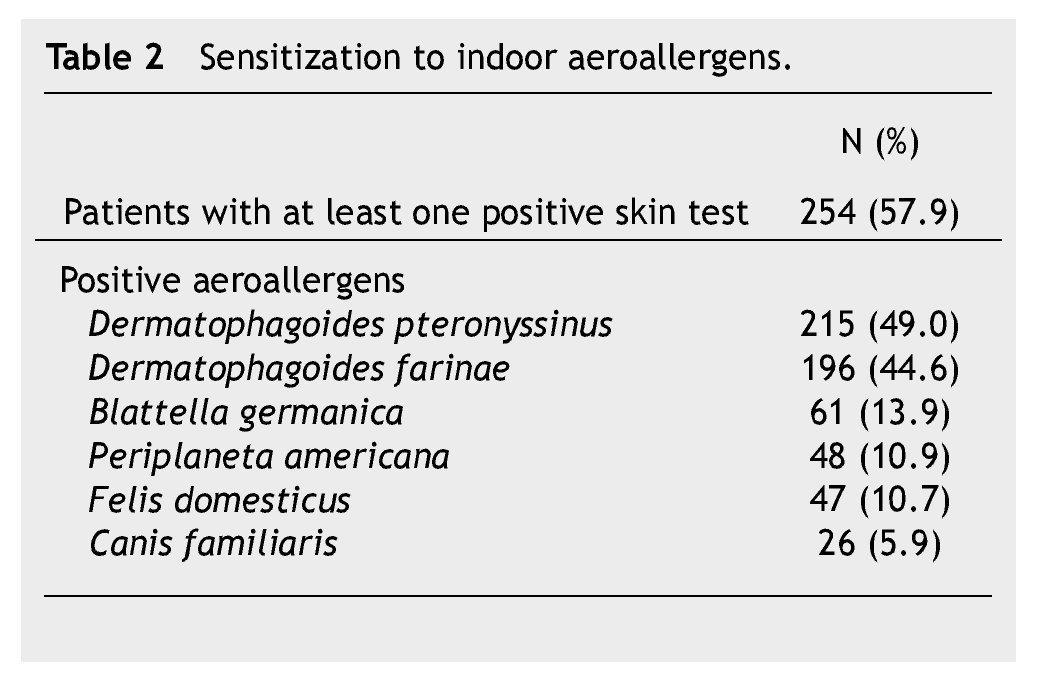
Two hundred and fifty-four of studied patients (57.9%) showed sensitization to at least one of the 6 tested aeroallergens. The main indoor aeroallergens causing sensitization in children included D. pteronyssinus (49%), D. farinae (44.6%) and B. germanica (13.9%) (Table 2).
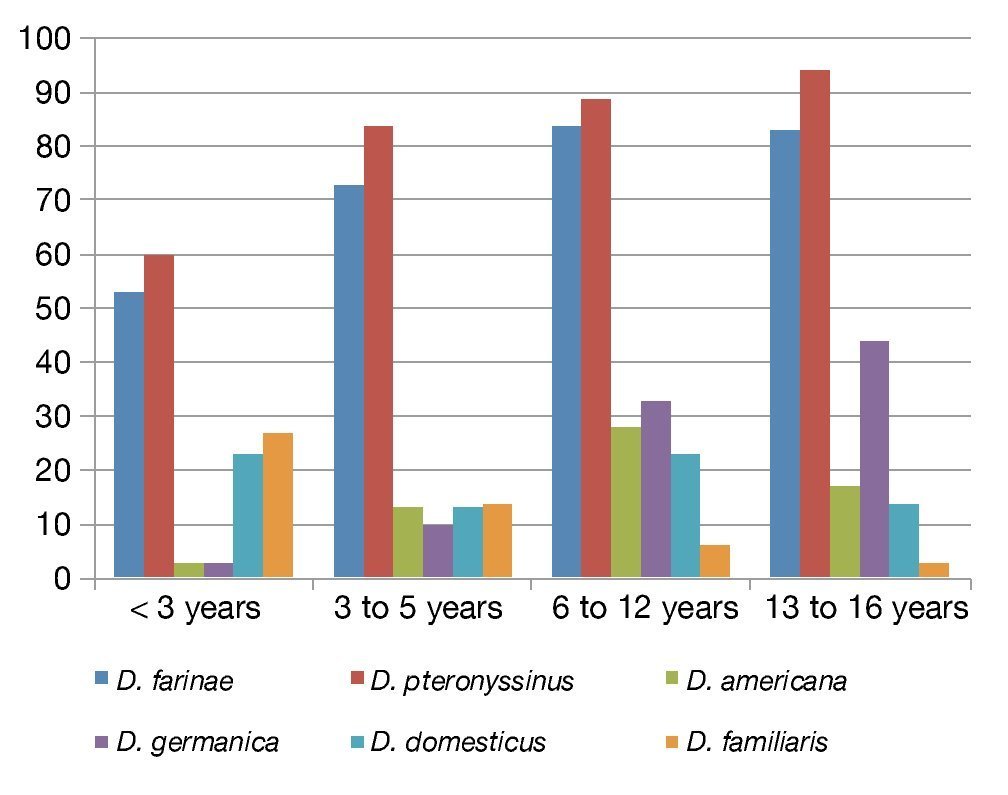
The rate of specific sensitization per age group was as follows: 38% in children under 3 years, 51.3% in children between 3 and 5 years, 69% in children between 6 and 12 years and 73% in children between 13 and 16 years of age (Fig. 1).
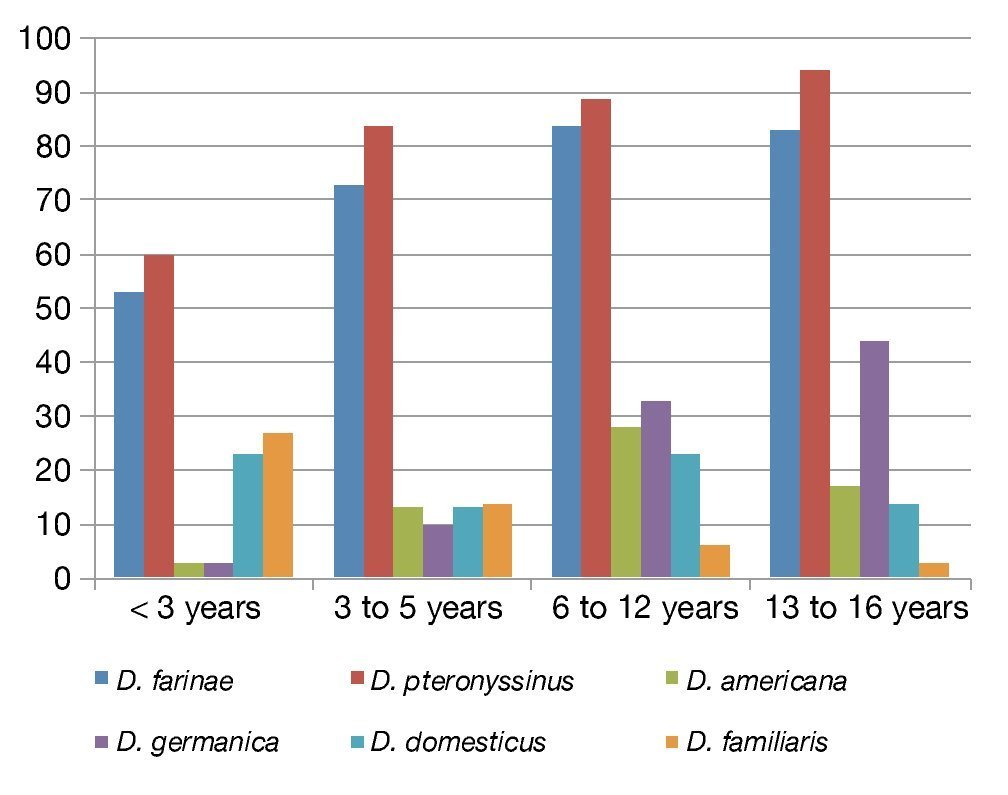
Figure 1 Distribution of sensitization to aeroallergens by age group.
The older the child, the more frequent the sensitization to indoor aeroallergens. Sensitization to dust house mites -mainly D. pteronyssinus- occurred in all age groups. Cockroach sensitization displayed a directly proportional relationship with age, with a greater prevalence to B. germanica in children over 6 years of age. Sensitization rate for C. familiaris displayed a higher proportion in children under 3 years with 27%, decreasing as children get older, reaching 3% in the 13 to 16 group.
Discussion
Indoor aeroallergen sensitization increases the risk of developing allergic diseases, including asthma, allergic rhinitis and atopic dermatitis.6 Different studies conducted in pediatric populations, as well as in adults who suffered from allergies, have shown that as time passes monosensitization leads to allergenic polysensitization, which constitutes a characteristic of the natural history of atopia.7,8 In our study, the rate of indoor allergen sensitization was 57.7%, similar to the results obtained in a study conducted by Sheehan et al. in a pediatric population in Boston, where they reported a sensitization of 51.3% for at least one indoor allergen,2 whereas in the general population sensitization to indoor allergens occurs up 30% of people.9 D. pteronyssinus and D. farinae were the most prevalent indoor aeroallergens as a cause of sensitization in the children in our study. In a study conducted by Kim et al. in a pediatric population in Korea, they found a prevalence of sensitization to D. pteronyssinus of 32.1% and 42.7%, and to D. farinae of 32.4% and 41.9%, in children between 6 and 7 years of age and between 12 and 13 years of age, respectively.10 On the other hand, the prevalence of sensitization to dust house mites had been reported up to 27.5% of people in the general population in the US.11 This shows that indoor allergen sensitization prevalence is greater in the studies where a pediatric population is included and in those studies where the patients are assessed by an allergy specialist.
Sensitization to cockroaches was at 13.9% for B. germanica and of 10.9% for P. Americana. Calabria et al. reported a general sensitization to cockroaches of 12.5% in children with rhinitis.12 In our study, sensitization to cat was 5.9%, similar to the data found in a cohort study from birth to 4 years of age, with a sensitization of 5.1%.13 On the other hand, espinoza et al. found sensitization to cat at 10%, in children up to 4 years old,14 which differs from our study, where sensitization to cat in children up to 5 years old was just 3.8%.
Sensitization to aeroallergens can occur in the early stages of life, increasing as the person ages, in many cases going through monosensitization to polysensitization.15 It is possible to see this transition from monosensitization to polysensitization in pre-school and school-aged children.
In a meta-analysis published by Goldhahn et al., they found a rise in aeroallergen sensitization from 14.2% to 21.6% in patients from 7 to 23 years of age.16 Similar data can be found in a study of children conducted in Turkey where the prevalence in children from 2 to 6 years of age was at 16.1% increasing up to 55.1% in patients 12-18 years of age.17 In pediatric population, the prevalence of sensitization to dust mites, cockroaches, dog and cat appears to be higher in older patients.2 Sensitization to dust mites, and to a lesser degree to pollens seems to have a “triggering” effect in the developing of polysensitization, due to the large number of children who are initially monosensitized to mites.18 A recent preliminary study suggests that a defect in the function of regulatory T cells can explain the tendency to develop polysensitization in this population, because children with persistent monosensitization produce a larger amount of interleukin 10 and interferon gamma than the children who develop polysensitization.19
In the pediatric population that goes to see the doctor at the Allergy Outpatient Clinic of the “Dr. José Eleuterio González” University Hospital of the UANL, indoor aeroallergen sensitization is around 50% and D. pteronyssinus and D. farinae are the main involved allergens. In the atopic population, frequency of sensitization directly increases with the patient’s age; however it may be present from the early stages of life. Early detection is recommended using skin tests on all children under suspicion of allergy, in order to begin a timely treatment and modify the natural history of the allergic disease.
Conflicts of interest
The authors have no conflicts of interest to declare.
Funding
No financial support was provided.
Received: February 2014;
Accepted: June 2014
* Corresponding author:
Regional Center of Allergy and Clinical Immunology (CRAIC),
“Dr. José Eleuterio González” University Hospital. Francisco I.
Madero and Gonzalitos Avenue, Mitras Centro,
Z.P. 64460, Monterrey, N.L., Mexico.
Telephone: (81) 8346 2515. Fax: (81) 8347 6798.
E-mail address: aarias45@hotmail.com (A. Arias-Cruz).