




The purpose of this letter is to present failure mode and effects analysis (FMEA), a tool with clinical safety applications that may be useful for minimising risks associated with healthcare procedures. We also describe our experience with applying FMEA to intrathecal chemotherapy at Hospital Universitario Donostia.
Intrathecal chemotherapy is an invasive procedure associated with numerous adverse events, many of which may be caused by human error.
At Hospital Universitario Donostia, intrathecal chemotherapy has traditionally been prescribed and ordered by haematology or oncology departments, whereas the neurology department is responsible for administering the treatment. Since there have been several severe incidents related to intrathecal chemotherapy, we recently decided to find a way to minimise the risks associated with this procedure.
FMEA was performed according to the following steps:
- 1.
Select a high-risk process. The chosen process was intrathecal chemotherapy.
- 2.
Assemble a team. We gathered a multidisciplinary work team, including doctors and nurses familiar with intrathecal chemotherapy from the haematology, oncology, pharmacy, neurology, and quality control departments.
- 3.
Describe the process. We designed a diagram describing the different steps in the process and how they are interrelated (Fig. 1).
- 4.
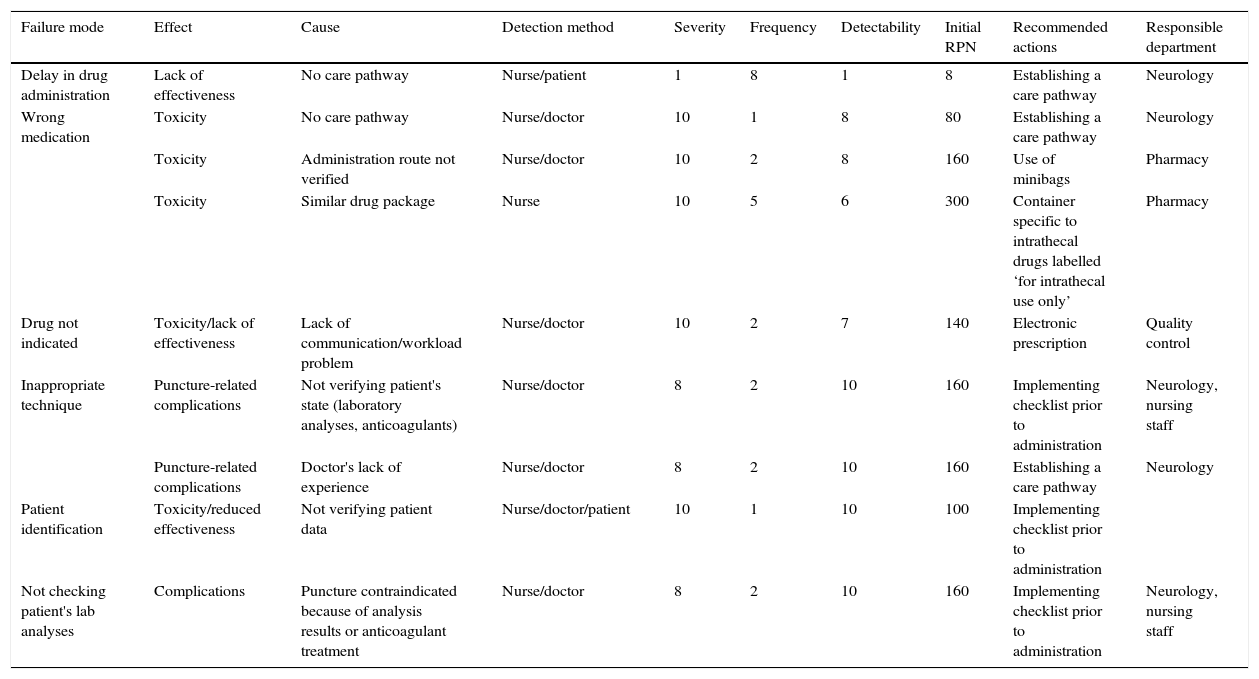
Analyse risk. Team members brainstormed to list different possible ways in which each sub-process might fail. Next, cause, effect, and detection method for each failure mode were identified and rated for frequency, severity, and detectability on scales of 1 to 10. Finally, total risk for each failure mode was calculated by multiplying the values of these 3 factors (frequency, severity, and detectability) to give the risk priority number (RPN). As an example, Table 1 shows the model sheet used to collect risk analysis data for the sub-process of administering the drug.
Table 1.Risk analysis table for the administration sub-process in intrathecal chemotherapy.
Failure mode Effect Cause Detection method Severity Frequency Detectability Initial RPN Recommended actions Responsible department Delay in drug administration Lack of effectiveness No care pathway Nurse/patient 1 8 1 8 Establishing a care pathway Neurology Wrong medication Toxicity No care pathway Nurse/doctor 10 1 8 80 Establishing a care pathway Neurology Toxicity Administration route not verified Nurse/doctor 10 2 8 160 Use of minibags Pharmacy Toxicity Similar drug package Nurse 10 5 6 300 Container specific to intrathecal drugs labelled ‘for intrathecal use only’ Pharmacy Drug not indicated Toxicity/lack of effectiveness Lack of communication/workload problem Nurse/doctor 10 2 7 140 Electronic prescription Quality control Inappropriate technique Puncture-related complications Not verifying patient's state (laboratory analyses, anticoagulants) Nurse/doctor 8 2 10 160 Implementing checklist prior to administration Neurology, nursing staff Puncture-related complications Doctor's lack of experience Nurse/doctor 8 2 10 160 Establishing a care pathway Neurology Patient identification Toxicity/reduced effectiveness Not verifying patient data Nurse/doctor/patient 10 1 10 100 Implementing checklist prior to administration Not checking patient's lab analyses Complications Puncture contraindicated because of analysis results or anticoagulant treatment Nurse/doctor 8 2 10 160 Implementing checklist prior to administration Neurology, nursing staff - 5.
Propose improvements and monitor implementation of the redesigned process. A total of 10 improvement actions were defined, with priority given to failure modes with higher RPNs. We also decided which team members would be responsible for implementing each new process (Table 1).

Twenty-eight months after implementing improvements, 141 intrathecal chemotherapy procedures have been performed in a total of 38 patients and no incidents have been detected.
FMEA is a tool enabling systematic and prospective identification and prevention of the risks associated with a process. This technique has been widely used not only in healthcare but also in the aerospace and automotive industries.1
In addition to identifying and preventing failures that already occur or may potentially occur, it enables sharing experiences with different units participating in the same process. It is also recommended by several national and international health organisations.2,3
However, some of the main limitations of FMEA are the absence of studies verifying its validity or utility, its reliance on team members’ previous experiences, the mathematically flawed way in which RPN is calculated, and the fact that costs and healthcare available resources are not taken into consideration.4
In conclusion, FMEA is a useful tool since it provides an organised and systematic method which can help resolve failure modes that involve several professionals taking part in a single process.
In addition to intrathecal chemotherapy, neurology departments currently perform many other invasive procedures whose safety could be increased by using this technique. Examples include immunoglobulin administration, plasmapheresis sessions, and intravenous administration of antibiotics or immunosupressants.
Please cite this article as: de la Riva P, Martinez Zabaleta MT, Arruti González M, Urtasun Ocariz MA. Análisis de modos de fallo y sus efectos aplicado al procedimiento de quimioterapia intratecal. Neurología. 2015;30:62–64.
This study was presented orally, under the same title, at the 64th Annual Meeting of the Spanish Society of Neurology.
