




In recent decades there has been a special interest in theories that could explain the regulation of motor control, and their applications. These theories are often based on models of brain function, philosophically reflecting different criteria on how movement is controlled by the brain, each being emphasised in different neural components of the movement. The concept of motor learning, regarded as the set of internal processes associated with practice and experience that produce relatively permanent changes in the ability to produce motor activities through a specific skill, is also relevant in the context of neuroscience. Thus, both motor control and learning are seen as key fields of study for health professionals in the field of neurorehabilitation.
DevelopmentThe major theories of motor control are described, which include, motor programming theory, systems theory, the theory of dynamic action, and the theory of parallel distributed processing, as well as the factors that influence motor learning and its applications in neurorehabilitation.
ConclusionsAt present there is no consensus on which theory or model defines the regulations to explain motor control. Theories of motor learning should be the basis for motor rehabilitation. The new research should apply the knowledge generated in the fields of control and motor learning in neurorehabilitation.
En las últimas décadas ha existido un especial interés por las teorías que podrían explicar el gobierno del control motor y sus aplicaciones. Estas teorías suelen basarse en mode-los de función cerebral, reflejando criterios filosóficamente diferentes sobre la forma en la que el movimiento es controlado por el cerebro, enfatizando cada una de ellas en los distintos componentes neurales del movimiento. Asimismo, en el contexto de las neurociencias, toma relevancia el concepto de aprendizaje motor, considerado como el conjunto de procesos inter-nos asociados a la práctica, y la experiencia, que producen cambios relativamente permanentes en la capacidad de producir actividades motoras, a través de una habilidad específica. Por lo que ambos, control y aprendizaje motor, se posicionan como campos de estudio fundamentales para los profesionales sanitarios en el campo de la neurorrehabilitación.
DesarrolloSe describen las principales teorías de control motor como la teoría de la programa-ción motora, la teoría de sistemas, la teoría de la acción dinámica o la teoría del procesamiento de distribución en paralelo, así como los factores que influyen en el aprendizaje motor y sus aplicaciones en neurorrehabilitación.
ConclusionesEn la actualidad no existe un consenso sobre qué teoría o modelo es definitorio en dar explicación al gobierno del control motor. Las teorías sobre el aprendizaje motor deben ser la base para la rehabilitación motora. Las nuevas líneas de investigación deben aplicar los conocimientos generados en los campos del control y aprendizaje motor en neurorrehabilita-ción.
Studying the cause and nature of movement is essential in medical practice. Recently, doctors have shown particular interest in new theories about motor control (MC) and their applications. However, due to new research in the field of neuroscience, the scientific community lacks a single theory regarding MC and distance is growing between the theories and the therapeutic interventions used for alterations in MC.1
The specific methods that are typically used in neurorehabilitation therefore rest on basic suppositions about the cause and nature of movement, meaning that MC theory actually stems from the theoretical basis underlying therapeutic practices.2
In general terms, the purpose of neurorehabilitation is to cement patients’ existing skills, retrieve any lost skills, and promote learning of new abilities. A variety of factors may have a significant effect on neurorehabilitation and influence motor learning processes. These factors include verbal instructions, characteristics and variability of training sessions, the individual's active participation and motivation, positive and negative learning transfer, posture control, memory, and feedback. All of these factors are clinically applicable and they provide the basis for emerging or established lines of research having to do with retraining sensorimotor function in neurological patients.
The purpose of this study is to present a critical analysis of existing theories and models of MC and motor learning, and also study their potential clinical applications in the field of neurorehabilitation, referring fundamentally to regaining postural control and balance, locomotion, reach, grasp, and manipulation. Lastly, we describe the true possibilities for new technologies applicable to neurological disease.
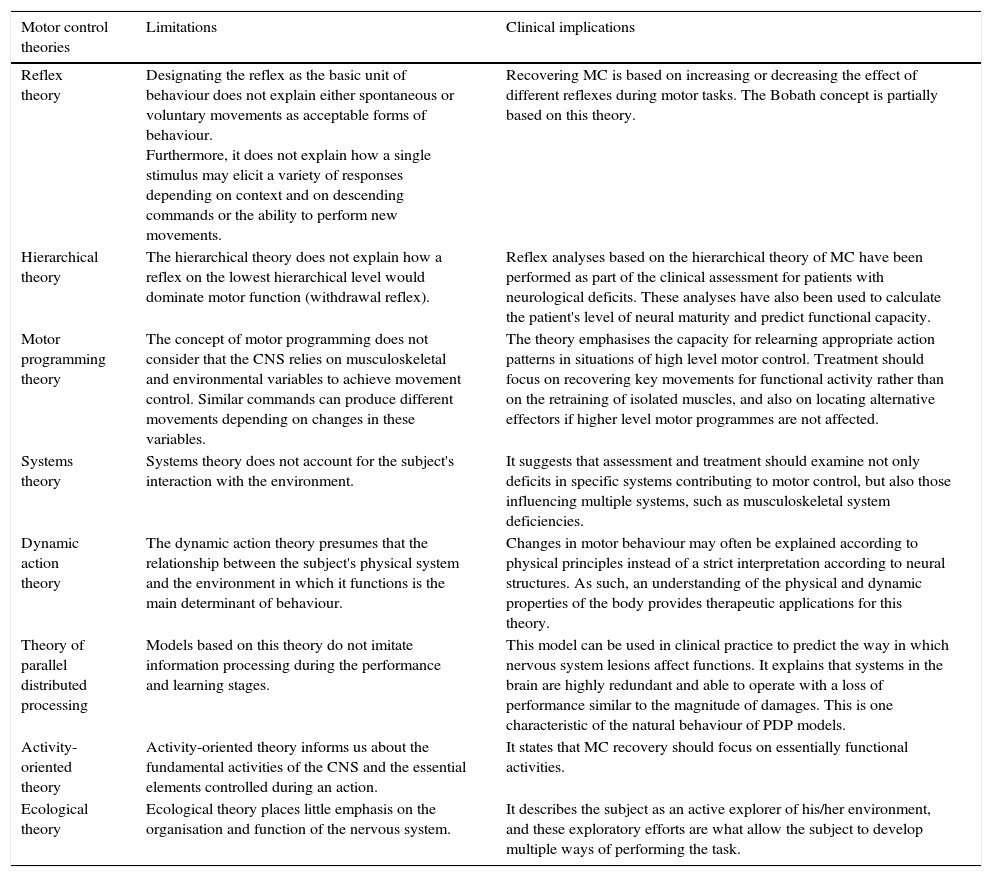
BackgroundTheories on motor controlThe different theories on MC reflect existing ideas of how movement is controlled by the brain. Each different theory emphasises the different neural components of movement.1 The specific methods used in neurorehabilitation are therefore based on general suppositions about the cause and nature of movement, meaning that MC theory actually stems from the theoretical basis underlying therapeutic practices,2 which in turn corroborate or refute these theories.3 The main limitations and clinical implications of different MC theories are shown in Table 1.
Limitations of motor control theories
| Motor control theories | Limitations | Clinical implications |
|---|---|---|
| Reflex theory | Designating the reflex as the basic unit of behaviour does not explain either spontaneous or voluntary movements as acceptable forms of behaviour. Furthermore, it does not explain how a single stimulus may elicit a variety of responses depending on context and on descending commands or the ability to perform new movements. | Recovering MC is based on increasing or decreasing the effect of different reflexes during motor tasks. The Bobath concept is partially based on this theory. |
| Hierarchical theory | The hierarchical theory does not explain how a reflex on the lowest hierarchical level would dominate motor function (withdrawal reflex). | Reflex analyses based on the hierarchical theory of MC have been performed as part of the clinical assessment for patients with neurological deficits. These analyses have also been used to calculate the patient's level of neural maturity and predict functional capacity. |
| Motor programming theory | The concept of motor programming does not consider that the CNS relies on musculoskeletal and environmental variables to achieve movement control. Similar commands can produce different movements depending on changes in these variables. | The theory emphasises the capacity for relearning appropriate action patterns in situations of high level motor control. Treatment should focus on recovering key movements for functional activity rather than on the retraining of isolated muscles, and also on locating alternative effectors if higher level motor programmes are not affected. |
| Systems theory | Systems theory does not account for the subject's interaction with the environment. | It suggests that assessment and treatment should examine not only deficits in specific systems contributing to motor control, but also those influencing multiple systems, such as musculoskeletal system deficiencies. |
| Dynamic action theory | The dynamic action theory presumes that the relationship between the subject's physical system and the environment in which it functions is the main determinant of behaviour. | Changes in motor behaviour may often be explained according to physical principles instead of a strict interpretation according to neural structures. As such, an understanding of the physical and dynamic properties of the body provides therapeutic applications for this theory. |
| Theory of parallel distributed processing | Models based on this theory do not imitate information processing during the performance and learning stages. | This model can be used in clinical practice to predict the way in which nervous system lesions affect functions. It explains that systems in the brain are highly redundant and able to operate with a loss of performance similar to the magnitude of damages. This is one characteristic of the natural behaviour of PDP models. |
| Activity-oriented theory | Activity-oriented theory informs us about the fundamental activities of the CNS and the essential elements controlled during an action. | It states that MC recovery should focus on essentially functional activities. |
| Ecological theory | Ecological theory places little emphasis on the organisation and function of the nervous system. | It describes the subject as an active explorer of his/her environment, and these exploratory efforts are what allow the subject to develop multiple ways of performing the task. |
CNS: central nervous system.
In 1906, the neurophysiologist Sir Charles Sherrington established the basis for the reflex theory of motor control,4 according to which reflexes were the building blocks of complex behaviour intended to achieve a common objective.5 He described this behaviour in terms of compound reflexes and their combined or chained action.6–14 A stimulus provokes a response, which is transformed into the stimulus of the next response.
Hierarchical theoryThe hierarchical theory states that the central nervous system (CNS) is organised in hierarchical levels such that the higher association areas are followed by the motor cortex, followed by the spinal levels of motor function. Each higher level controls the level below it according to strict vertical hierarchy; the lines of control do not cross, and lower levels cannot exert control.3 In the 1940s, Gesell15 and McGraw16 came up with the neuromaturational theory of development. Normal motor development is attributed to increasing corticalisation of the CNS that gives rise to the appearance of higher levels of control over the lower level reflexes; CNS maturation is the main agent of change in development, with only minimal input from other factors. The hierarchical theory has evolved and scientists recognise that each of the levels may act upon the others depending on the activity performed. Reflexes are no longer considered the sole determinant of MC, but rather one of many essential processes in movement initiation and control.17
Motor programming theoriesThe most recent theories on MC distance themselves from the idea of MC as a fundamentally reactive system. They have begun to explore the physiology of actions instead of the nature of reactions. A specific motor response may be elicited by either a sensory stimulus or by a central process where there is no afferent stimulus or impulse. As such, it is more correct to refer to a central motor pattern. This theory, which is mainly supported by locomotion analyses in cats,18 suggests that movement is possible in absence of a reflex action such that the spinal neural network would be able to produce locomotor rhythm without any sensory stimuli or descending patterns from the brain, and movement could be elicited without feedback.3 It also introduces the concept of central pattern generators (CPGs), or specific neural circuits able to generate movements such as walking or running. Incoming sensory stimuli exert an important modulatory effect on CPGs.19–24
Systems theorySystems theory explains that neural control over movement cannot be understood without a prior understanding of the systems that move. It states that “movements are controlled neither centrally nor peripherally, but rather are effected by interactions among multiple systems”.25 The body is regarded as a mechanical system subject to both internal forces and external forces (gravity).19 The same central command may give rise to very different movements due to interactions between external forces and variations in the initial conditions; also, the same movements may be elicited by different commands. The theory attempts to explain how initial conditions affect the characteristics of movement.26
Systems theory predicts real behaviour much more accurately than the preceding theories since it considers not only what the nervous system contributes to motion, but also the contributions of different systems together with the forces of gravity and inertia.
Dynamic action theoryThe study of synergies gave rise to dynamic action theory, an approach that observes the individual in motion from a new perspective.3 Considering the self-organisation principle, the theory states that when a system made up of individual parts is integrated, its parts will act collectively in an organised manner. They will not require any instructions from a higher centre on how to achieve coordinated action.27,28 The theory proposes that movement is the result of elements that interact, with no need for motor programmes. The dynamic action theory attempts to find mathematical descriptions of such self-organising systems in which behaviour is non-linear, meaning that when one of the parameters changes and reaches a critical value, the entire system transforms into a completely new configuration of behaviour. By using these mathematical formulas, it will be possible to predict the ways in which a given system will act in different situations. The dynamic action theory minimises the importance of the idea that the CNS sends commands to control movement, and it searches for physical explanations that may also contribute to the characteristics of movement.
Theory of parallel distributed processingThe theory of parallel distributed processing (PDP) describes the way in which the nervous system processes information in order to act. According to this theory, the nervous system operates both by serial processes (by processing information through a single channel) and by parallel processes (by interpreting information from multiple channels and analysing it simultaneously in different ways). The underlying premise is that the brain is a computer with cells that interact in different ways, and that neural networks are the brain's basic computational systems.29,30 The strategy consists of developing simplified mathematical models of cerebral systems and studying them in order to understand how different mathematical problems can be resolved by means of those mechanisms.29–31 These models consist of elements that are interconnected by circuits. As with neural synapses, each element may be affected by others in a positive or negative way, and to a greater or lesser extent. These elements can be classified as sensory neurons, interneurons, and motor neurons. Efficiency in task performance depends on the quantity of output connections and the strength of those connections.3
Activity-oriented theoryGreene32 pointed out the need for a theory able to explain how neural circuits operate in order to complete an action, and therefore able to provide the basis for a clearer picture of the motor system. The activity-oriented theory is based on the premise that the objective of MC is to master the movement involved in completing a specific action, and not just move for the sake of moving. Movement control is organised according to goal-oriented functional behaviour.3
Ecological theoryIn the 1960s, Gibson33 explored the way in which our motor systems allow us to interact more effectively with our surroundings in order to develop goal-oriented behaviour. He focused on how we detect information in our setting that is relevant to our actions, and how we then use this information to determine our movements.34 The individual actively explores his or her environment, and the environment promotes the performance of activities that are environmentally appropriate.
Motor learningMotor learning (ML) is defined as an array of internal processes associated with practice and experience and which, in the context of acquisition of a specific skill, will produce relatively permanent changes in how motor activity is elicited. What we learn is retained or stored in our brains and referred to as memory,35,36 whereas short-term modifications are not regarded as learning.37–39
The purpose of neurorehabilitation is to cement patients’ existing abilities, retrieve any lost abilities, and foster the learning of new skills. An ability is generally thought to be a relatively permanent characteristic or trait that is typically associated with a genetic component. It cannot be easily altered with practice or experiences.40 Another way of understanding ‘ability’ as a concept is to contrast it with ‘skill’. Unlike an ability, a skill can be modified or even acquired with practice or experience.41,42
Many factors affect ML, including age, race, culture, or genetic predisposition. The skills displayed by each individual are the result of a learning process.43
Theories on motor learningThe Fitts and Posner 3-stage model. Fitts and Posner37,38 suggest that there are 3 main stages in motor learning.
During the cognitive stage, the patient learns a new skill, or relearns an existing one. Patients will need to practise the task frequently, with outside supervision and guidance; it is important to make mistakes and know how to correct them in this process. During the associative stage, the patient is able to perform the task in a situation with specific environmental restrictions. The patient will make fewer errors during the activity and complete it more easily. Patients will begin to understand how the different components of a skill are interrelated. During the autonomous phase, the patient is able to move in a variety of settings and maintain control throughout the task. The true proof of learning is the ability to retain a skill and apply it in different settings through automatisation, since practical situations in real life are generally random.38
Bernstein's 3-stage model. Bernstein's model emphasises quantifying degrees of freedom, that is, the number of independent movements needed to complete an action, as a central component of learning a new motor skill. This learning model includes 3 stages. During the initial stage, the individual will simplify his or her movements by reducing the degrees of freedom. In the advanced stage, the individual will gain a few degrees of freedom, which will permit movement in more of the articulations involved in the task. Lastly, the subject in the expert stage possesses all the degrees of freedom necessary in order to carry out the task in an effective and coordinated manner.
Gentile's 2-stage model. The first stage of Gentile's model includes understanding the purpose of the task, developing movement strategies appropriate for completing the task, and interpreting environmental information that is relevant to organising movement. In the second stage (fixation or diversification), the subject aims to redefine movement, which includes both developing the capacity to adapt movement to changes in task and in setting, and being able to perform the task consistently and efficiently.
Phases in motor programme creation. Different researchers have asked which hierarchical changes might occur in movement control when motor programmes come together during the learning of a new task.40 Motor programmes that regulate a complex behaviour may be created by combining motor programmes controlling smaller units of behaviour until the larger process is completed as a single unit.40
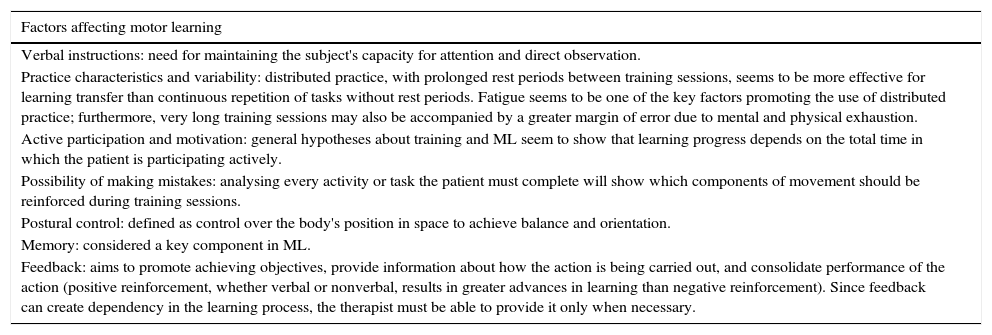
Factors affecting motor learningSeveral factors act on ML processes, such as verbal instructions, characteristics and variability of training sessions, the individual's active participation and motivation, the option of making mistakes, postural control, memory, and feedback (Table 2).
Motor learning
| Factors affecting motor learning |
|---|
| Verbal instructions: need for maintaining the subject's capacity for attention and direct observation. |
| Practice characteristics and variability: distributed practice, with prolonged rest periods between training sessions, seems to be more effective for learning transfer than continuous repetition of tasks without rest periods. Fatigue seems to be one of the key factors promoting the use of distributed practice; furthermore, very long training sessions may also be accompanied by a greater margin of error due to mental and physical exhaustion. |
| Active participation and motivation: general hypotheses about training and ML seem to show that learning progress depends on the total time in which the patient is participating actively. |
| Possibility of making mistakes: analysing every activity or task the patient must complete will show which components of movement should be reinforced during training sessions. |
| Postural control: defined as control over the body's position in space to achieve balance and orientation. |
| Memory: considered a key component in ML. |
| Feedback: aims to promote achieving objectives, provide information about how the action is being carried out, and consolidate performance of the action (positive reinforcement, whether verbal or nonverbal, results in greater advances in learning than negative reinforcement). Since feedback can create dependency in the learning process, the therapist must be able to provide it only when necessary. |
Verbal instructions help subjects focus their attention on specific objectives and influence the learning strategies that these subjects will use when completing a movement.38,44 Regarding characteristics and variability of training sessions, the tasks being assigned should include repetition. We should be mindful of the concept of “repetition without repeating”, that is, training sessions must include recording the parameters that have been modified, since this will challenge the patient and make it easier to extrapolate learning to different settings and situations. In cases in which physical practice is not possible, some researchers suggest that mental practice may be an effective way of stimulating learning.45 Learning can be promoted or interrupted by the context. Different contexts lead to better results and a more generally effective and enriching learning experience. For this reason, practice in the clinical environment should include a range of conditions so that learning can be transferred to a variety of changing situations. The amount of transfer depends on the similarity between the clinical environment and the real environment.46
Another important concept related to ML is the patient's active participation in the task being carried out. In completing the task or activity and resolving and overcoming the problem, the patient's motivation and commitment are crucial factors. Active participation strengthens the learning process and helps keep learning continuous.
Allowing patients to make mistakes while completing a new activity, and providing them with possible solutions or encouraging them to propose their own, are beneficial for ML activities aimed at training new skills.38 Correct postural control47,48 and unimpaired memory are important for patients to be able to learn a new motor activity or recover a previously existing one.49
Feedback is the term for information received as a result of movement (Table 3). We can distinguish between intrinsic feedback, the consequence of movement (exteroceptive and proprioceptive pathways) that permits postural adjustment; and extrinsic feedback, or all information provided by an external source. The purpose of feedback is to provide the patient with information about the result of the movement as a complement to intrinsic information. There are two categories of extrinsic information: understanding of results, that is, all verbal information about the result of the movement, which is particularly important when intrinsic feedback is reduced; and understanding of performance, which is linked to movement patterns employed when completing a task, and which provides information on movement quality.50,51 Extrinsic feedback is essential when the patient's source of intrinsic feedback is reduced or distorted, and this is frequent among patients with neurological impairment. As part of any learning process, subjects should receive some type of information about their errors from an intrinsic or extrinsic source. The characteristics of extrinsic feedback that increase the patient's cognitive abilities are listed in Table 3.
Extrinsic feedback
| Provides information about the subject's progress in learning to do the activity, which fosters motivation. |
| Delivers information about the events that make up the action, allowing the subject to create a mental model of the activity and interpret his or her possibilities for achieving objectives. |
| Provides positive reinforcement when subjects are informed that they have completed the tasks correctly. Feedback has an immediate effect on an individual's motivation, as well as attention span and concentration on the task. |
| Repeated feedback aimed at correcting errors may create dependence and discourage the subject from experimenting with and analysing the characteristics of his or her action. To prevent dependence, feedback should only be given when necessary depending on the complexity of the tasks and the subject's level of experience. This type of reinforcement should therefore be given sporadically and not during every repetition. |
Children do not use feedback in the same way as adults; the latter benefit more from reduced feedback, whereas children require more continuous but less precise feedback. Reduced feedback increases the subject's cognitive effort; when feedback is hidden, the subject will need to focus on and interpret intrinsic information produced by the activity that has been performed. This increase in cognitive effort fosters optimal changes in adult patients and maximises ML, but this is not true in children. Children require more practice sessions with feedback in order to complete the activity more precisely and consistently. After that point, feedback should be decreased progressively in order to stimulate cognitive effort and ML. A subject's ability to process information and focus on the intrinsic information associated with the task will determine the amount of external reinforcement needed.50,51
Clinical applications of motor control and learning theories in neurorehabilitationScientific knowledge must be transferred continuously to clinical practice in order to provide new therapeutic strategies that reinforce and strengthen existing strategies. For methodological reasons, we will describe the therapeutic strategies intended to recover or improve postural control and balance separately from strategies for locomotion and manipulation.
Postural control and balanceThe literature seems to show that physical exercise is an effective means of improving balance in neurological patients,52–56 and such improvements may be able to increase patients’ functional capacity and reduce falling. The effectiveness of exercise programmes depends on whether they include multidimensional tasks instead of tasks focusing on a single area.57 Classic programmes have now been joined by new parallel methods with more holistic approaches, such as tai chi,58,59 sensory training,60 and dual-task training (motor and cognitive tasks).61 Current scientific evidence points to the usefulness of instrumented systems, such as computerised dynamic posturography. Researchers are designing studies that attempt to show that these systems are also valid as retraining tools.62
LocomotionThe purpose of these interventions is to optimise gait by preventing shortening of soft tissues, increase muscle strength and control, and train rhythm and coordination. These goals are achieved by combining stretching, strength, load-bearing, and gait exercises.63
Traditionally, strength training therapy consisted of performing resistance exercises or activities using suspension and pulley systems with springs and weights. Techniques based on the Bobath concept64 or on proprioceptive neuromuscular facilitation65 are still being used; however, few studies have examined their efficacy. Current methodology is somewhat more sophisticated, with techniques ranging from use of elastic bands to exercises on isokinetic machines, and even electrical stimulation. Although studies have shown that strength training for one muscle or muscle group increases total strength, there is no evidence that it increases muscle function. The synergistic skills required in closed kinetic chain (CKC) exercises for locomotion need to be trained repeatedly and often, at different speeds and in different environmental conditions.
Carr and Shepherd66 describe a motor rehabilitation programme for stroke that is based on practising specific functional tasks. Starting from this concept, early recourse to such tools as a treadmill67,68 with partial support for body weight seems appropriate; this therapy may be combined with functional electrical stimulation (FES) during training,69 or with robotic assistance.70
Sensory retraining is one means of implementing the benefits of the therapies listed here. Some studies have observed improvements in dynamic balance among patients whose exercise programme included sensory modification.71 Feedback in treatment programmes helps patients improve their capacity for perceiving movement and provides an effective stimulus for improving execution of the task.72,73
Reach, grasp, and manipulationAlthough the final goal of any treatment programme for the upper limbs will be recovering lost functions or establishing compensatory mechanisms, interventions can be classified as those focusing on deficits, those aimed at recovering function, and those that propose practising specific tasks.
Deficit-oriented interventionsA wide range of approaches, including active exercise, passive exercise, progressive resistance and isokinetic systems,74,75 myofacial release,76 and tai chi programmes have been used in motor re-education. Plaster casts, splints, and orthotics are used to treat rigidity and shortening in different structures. Biofeedback and FES are useful in recruiting paretic muscles. Regarding sensory retraining, Byl et al.77,78 found improvements of 20% in functional independence, fine motor activity, sensory discrimination, and musculoskeletal performance.
Strategies aimed at recovering function through movement trainingStoikov et al.79 used postural activities aimed at improving prehensile functions in the ataxic upper limb, and they found significant improvements after a 4-week programme. Another interesting example is Herdman's proposal for patients with vestibular dysfunction.80
Since the 1970s, researchers have developed various techniques for facilitating active movement using real objects and training different reaching and grasping scenarios using increasingly difficult activities requiring different types of manipulation.81–83 Occupational therapist Rhoda Erhardt published a detailed observation of the development of the sequence followed when letting go of objects.84
Task-oriented trainingDun et al.85 developed a therapeutic framework based on ecological theory. Practising a specific task is important in order to improve function, and training can be applied to several different activities of daily living.86,87
There have been promising results from numerous studies that have shown improvement of upper limb function through constraint-induced movement therapy (CI therapy). However, a recent systematic review in children with hemiplegia88 calls for caution in using the technique in all patients and recommends conducting additional well-designed studies. Furthermore, the systematic review by Langhorne, Coupar, and Pollock seems to indicate that CI therapy in stroke patients yields clinical benefits for arm function, but improvements in hand function are less clear.89 Bilateral or bimanual training in patients with hemiplegia has been shown to improve coordination between the two hands, as well as increasing function on the affected side.90,91 Bimanual training is diametrically opposed to the theory behind CI therapy. It is possible, however, for both treatments to be valid: bilateral treatment is more appropriate for generating new reorganised cortical networks in early stages after stroke, whereas CI therapy is for long-term treatment aimed at recovering networks in disuse.
Use of neuromuscular electrical stimulation (NMES)The functional application of NMES involves activating paralysed muscles using a specific sequence and precise magnitudes in order for the patient to perform functional tasks. This has given rise to the concept of neuroprosthetics, devices able to substitute upper and lower limb motor function needed for self-care and mobility tasks, bladder function, and respiratory control.92
Biofeedback and virtual realityTask-oriented biofeedback therapy is very effective. It employs virtual reality (VR) technology which offers real-life experiences, and results from this technique are superior to those yielded by classic biofeedback methods. However, the true therapeutic benefits of these systems have not yet been tested by well-designed clinical trials.93
Brain-computer interfaceStudies of the devices known as brain-computer interfaces attempt to gain a deeper understanding of the cortical physiology underlying human intention and provide signals for more complex control based on brain signals. The authors of a recent review94 describe the current state of BCI technology and summarise emerging studies aiming to further the clinical applications of these devices.
Use of robotics in neurorehabilitationA recently published systematic review95 found no significant overall benefits for stroke patients treated with robot-assisted therapy as measured by upper limb function or activities of daily living; in contrast, the authors did observe significant improvement in the proximal part of the limb. One of the best-known robotic systems used to improve locomotion in neurological patients is Lokomat, an orthotic device that stimulates and reproduces an individual's physiological gait. Studies of Lokomat published in a variety of scientific journals seem to support the device's utility.96,97
ConclusionsAt present, there is no consensus on which theory or model defines the way motor control is regulated. Motor learning theories should provide the basis for motor rehabilitation. Well-designed studies have shown that transferring neurological patient's key gains in therapy to contexts that are relevant to that patient, in addition to variability, active participation, the possibility of making mistakes, feedback, and incentives for motivation, are crucial for decreasing functional deficits in neurological patients. This being the case, lines of research that investigate these factors may be of interest as new neurorehabilitation methods and technologies come into use.
FundingThis study is part of the research project titled Dispositivos híbridos neuroprotésicos y neurorrobóticos para compensación funcional y rehabilitación de trastornos del movimiento (HYPER) within the framework of CONSOLIDER-INGENIO 2010. 2009 Call for Projects by the Ministry of Science and Innovation. Lead researcher: José Luis Pons Rovira. Institute of Industrial Automation, Spanish National Research Council (CSIC).
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Cano-de-la-Cuerda R, Molero-Sánchez A, Carratalá-Tejada M, Alguacil-Diego IM, Molina-Rueda F, Miangolarra-Page JC, et al. Teorías y modelos de control y aprendizaje motor. Aplicaciones clínicas en neurorrehabilitación. Neurología. 2015;30:32–41.
