



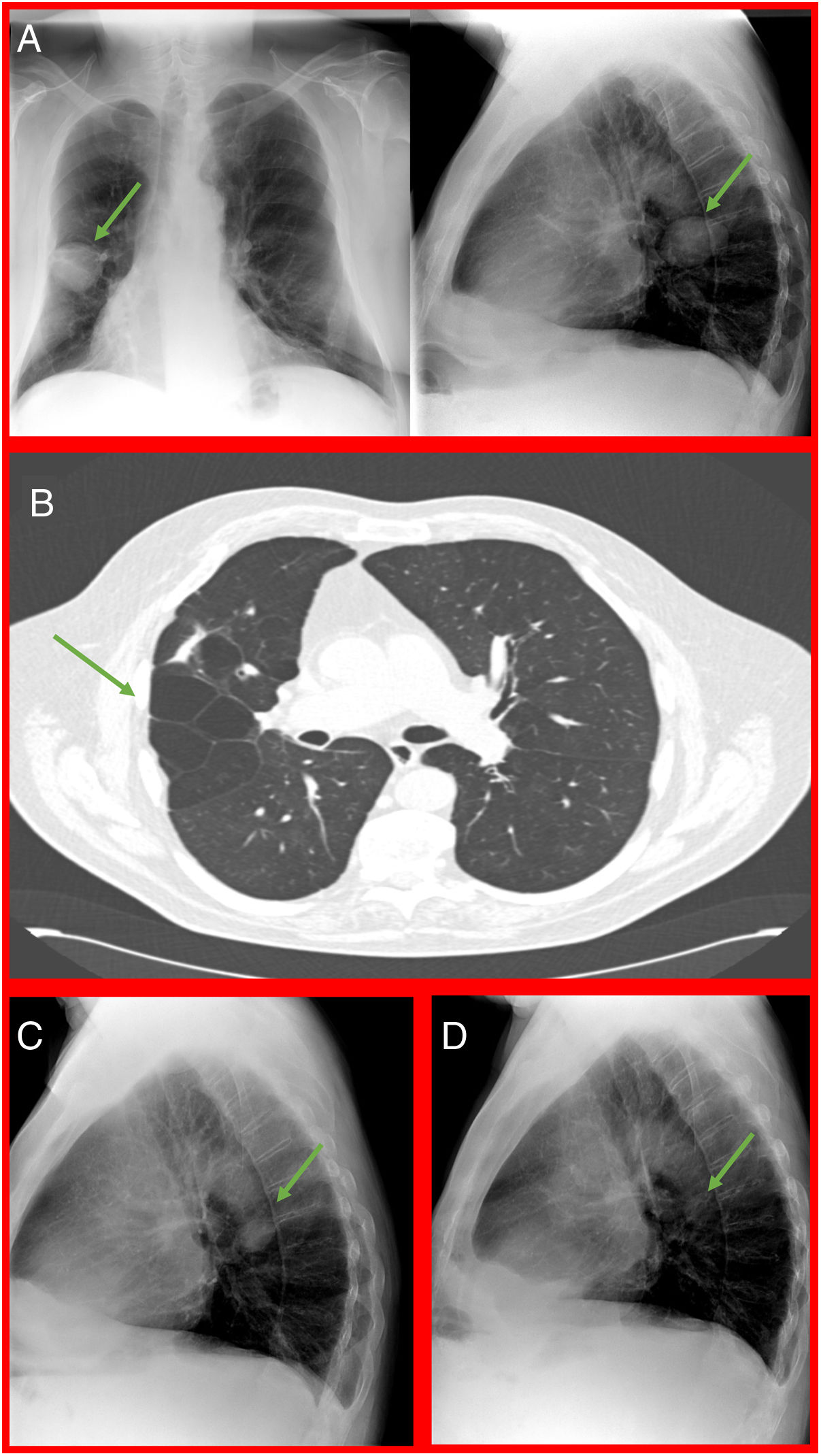
71-year-old male smoker, in follow-up for chronic obstructive pulmonary disease (COPD), emphysema phenotype, with large bullae and bronchiectasis. During follow up a 7cm lung mass is observed in the middle field of the right lung (Fig. 1A). He referred cough, purulent expectoration, fever and one-month dyspnea. On examination, a decrease in bilateral vesicular murmur was detected. Analytical determinations were normal. Differential diagnosis between neoplasms, lung infections, vascular alterations (pulmonary infarction and hematoma) and phantom tumor was considered. The patient, with full awareness of the clinical suspicion and its consequences, rejected the performance of computerized tomography (CT) and bronchoscopy, exercising his right of autonomy. The radiological image was carefully analyzed, highlighting the well-defined edges of the mass, the absence of spiculation or cavitation. In previous chest CTs, the area of development of the mass corresponded to a zone of parenchymal destruction with multiple cystic cavities (Fig. 1B). It was decided to start prolonged antibiotic treatment with amoxicillin-clavulanic with good response (Fig. 1C) and subsequent disappearance of the mass (Fig. 1D).

A. Poster-anterior and lateral chest radiograph. 7cm pulmonary mass. B. CT scan. Centrolobular emphysema with cystic cavities in the right upper lobe. C. Lateral chest radiograph. Clear decrease in the density of the pulmonary mass. D. Lateral chest radiograph. Complete disappearance of lung mass.
Different isolates have been obtained from infected lung bullae (Staphylococcus aureus, Bacteroides, Pseudomonas aeruginosa, etc.).1 It is always important to rule out a neoplastic origin, which in this case was impossible.
