



Burnout syndrome (BS) has been evaluated in few populations of medical students, and its relationship with depression is even less studied. The objective was to determine the frequency of BS in medical students of the Universidad Pedagógica y Tecnológica de Colombia (UPTC), in Tunja, Colombia, as well as its association with depression and other social, economic, demographic, and academic factors.
MethodsAn observational, analytical, cross-sectional study was carried out on 182 UPTC medical students during 2018. The Maslach Burnout Inventory-Student Survey (MBI-SS) was applied, with which 3 components were obtained to determine positive SB. This was crossed in the Stata 15 program for depression and other social, economic, demographic, and academic covariates with the Generalised Linear Model (GLM).
ResultsOf 182 respondents, 51.4% were women. The median age was 21 years (20−23 years). 14% had BS, of which 48% had depression. In the multiple regression, BS was significantly associated with a higher frequency of depression (RPa = 5.54; IC95%, 2.36−13.02; P < 0.001) and the feeling of insufficient money (RPa = 4.37; IC95%, 1.95−9.83; P < 0.001), in contrast to a negative association with smoking (RPa = 0.13; IC95%, 0.06−0.30; P < 0.001) and being a woman (RPa = 0.32; IC95%, 0.12−0.82; P = 0.018). The age of onset of marijuana use was not significant.
ConclusionsBS shows a high association with increased depression and a feeling that the money is not enough at the end of the month, but it showed a negative association with tobacco consumption and being a woman. Such students should be detected to provide them with adequate academic support
El síndrome de burnout (SB) se ha evaluado en escasas poblaciones de estudiantes de Medicina, y aún menos su relación con la depresión. El objetivo es determinar la frecuencia de SB en estudiantes de Medicina de la Universidad Pedagógica y Tecnológica de Colombia (UPTC), de Tunja, Colombia, así como su asociación con depresión y otros factores sociales, económicos, demográficos y académicos.
MétodosEstudio observacional analítico de corte transversal realizado en 182 estudiantes de Medicina de la UPTC durante 2018; se les aplicó la prueba Maslach Burnout Inventory-Student Survey (MBI-SS), con lo que se obtuvieron los 3 componentes para determinar SB positivo, y se cruzó en el programa Stata 15 según la depresión y otras covariables sociales, económicas, demográficas y académicas con los Modelos Lineales Generalizados (GLM).
ResultadosDe los 182 encuestados, el 51,4% era mujeres, con una mediana de edad de 21 [20–23] años. El 14% tenía SB; de ellos, el 48% tenía depresión. En la regresión múltiple, se asoció significativamente el SB con una mayor frecuencia de depresión (RPa = 5,54; IC95%, 2,36–13,02; p < 0,001) y sentir que el dinero no alcanza (RPa = 4,37; IC95%, 1,95–9,83; p < 0,001), al contrario que la asociación negativa con tabaquismo (RPa = 0,13; IC95%, 0,06–0,30; p < 0,001) y ser mujer (RPa = 0,32; IC95%, 0,12−0,82; p = 0,018). La edad de inicio del consumo de marihuana no fue significativa.
ConclusionesEl SB sí muestra una alta asociación con el incremento de depresión y sentir que el dinero no alcanza a fin de mes, pero se mostró una asociación negativa con el consumo de tabaco y ser mujer, por lo cual se debe detectar a dichos estudiantes con el fin de brindarles un apoyo académico adecuado.
Medicine is one of the academic environments in which the highest rates of anxiety and stress have been reported, due to the high level of demand during the undergraduate degree, something that differs from other university majors.1 All of this, finally, can lead to an imbalance in the medical student that, ultimately, generates a higher level of depression, accumulated stress, among others, and therefore, as studies progress, i.e., the longer the academic semester or year, the greater the concern and demand. This has been reported, to a large extent, throughout Latin America and the world2,3 as a great concern for medical students.
Currently, in a world where information is constantly changing and advances in health are becoming more frequent, medical students must store a large amount of new information, which adds to the stress level of their career.1 This causes many of them to end up generating a response to chronic academic stress as a final form of adaptation, known as Burnout Syndrome (BS).4
Academic BS is characterised by exhaustion due to the demands endured, a cynical attitude towards academia and quite marked inefficiency, properties that make up the triad of positive BS4 in which, at a higher level of exhaustion and cynicism along with lower effectiveness, greater BS is found in those exposed. There are many ways to make this diagnosis; one is the one that includes the three components of BS, but it can also be done with one of these two altered criteria, which is known as the BS by binomial.5
BS has been well studied in health workers, mainly nursing,6 while in students (especially medicine) there are very few, mostly descriptive studies,7,8 with few realities9 or only with students who are completing their degree.10,11 Likewise, there are few investigations that have evaluated the relationship between BS and some mental, psychosocial or academic alterations in this population,9–11 mostly carried out on graduated professionals, which demonstrates the lack of information about the characteristics in which intervention could be made to reduce the frequency of the disease, as well as the little importance given to the mental health of future doctors who, by not being completely healthy, could end up indirectly harming patients and, ultimately, increasing work absenteeism and the cost for the health system of any country.
For all of the above, the objective of this study is to establish the frequency of BS in medical students at the Universidad Pedagógica y Tecnológica de Colombia [Pedagogical and Technological University of Colombia] (UPTC), in Tunja, Colombia, as well as its association with depression and other social, economic, demographic and academic factors.
MethodsDesign and populationThis was a cross-sectional analytical observational study; a survey was applied to collect data in the UPTC Faculty of Health Sciences (FCS) in its medical school. The sampling was non-probabilistic for convenience. The statistical power of the crosses of the main variable with the main covariates was calculated and excellent powers were obtained for depression (100%), tobacco consumption (98%), feeling that money is not enough to make ends meet (90%) and marijuana use (97%).
Students enrolled during the 2018-I period who agreed to voluntarily enter the study were included. Surveys without data on the variables of interest or that had repetitive schemes, were from students in a rotating medical internship, or had other circumstances that generated difficulties in their inference were eliminated (no exclusions were made).
Instruments and variablesThe measurements of the dependent variable were obtained according to the Maslach Burnout Inventory-Student Survey (MBI-SS),12 a scale with excellent psychometric properties validated in many countries and translated into Spanish and endorsed by studies carried out in Colombia,1,8,13 as well as corresponding publications in various Colombian cities and Latin American countries.14 The scores for each dimension of BS (exhaustion, cynicism and negative self-efficacy) were divided by the number of questions in it, and if the NTP-732 cut-off points for the concurrence of the three dimensions were met (exhaustion, ≥2.9; cynicism, ≥2.26; academic self-efficacy, ≤3.83), it was positive for BS with trimodal criteria, which made it possible to determine the proportion of positives and negatives qualitatively and thus obtain the recoded variable between having BS and not having it.
With the determination of BS (main variable), the proportional differences with the exposure variable were found, the latter calculated using the self-applied Zung scale for depression,15 which consists of 20 Likert-type questions that evaluate the level of depression that a person may have; when the score obtained is added, it classifies depression as mild (50–59), moderate (60–69) or severe (≥70). Subsequently, those who were classified within any of the previous three were considered depressed. The scale has been translated into Spanish and validated,16 and has been applied to Colombian students17 and medical students18 with excellent reliability (α = 0.92) and factorial validity.19
In addition, the independent covariates were investigated: sex, age, single status, academic cycle (basic/clinical), cumulative average, hours of daily study outside the university, feeling that money is not enough to make ends meet, tobacco consumption at some time in life and age of initiation of consumption, consumption of alcohol at some time in life and age of initiation of consumption, and consumption of marijuana at some time in life and age of initiation of consumption.
Procedures and ethicsThe data were obtained through a self-administered questionnaire, the first part of which corresponded to the MBI-SS questions. In the second part, the social, economic, demographic and academic data were investigated, while in the third the Zung test was applied.
After the approval of the ethics committee of the Hospital Nacional Docente Madre-Niño San Bartolomé [San Bartolomé Mother-Child National Teaching Hospital] in Lima, Peru, endorsed by the National Institute of Health (NIH), the surveys were carried out at the medical school during the months of February, March and May 2018, during academic hours after asking permission from the professor in charge and explaining the voluntary nature of the survey, as well as the justification and objective of the research. The data were loaded into a Microsoft Office Excel 2016 for Windows spreadsheet in order to debug and filter the information. Finally, everything was transferred to Stata statistical software version 15 (StataCorp LP, United States) for analysis.
Data analysisFor descriptive statistics, prevalence and frequency distribution measures were used, characterising the respondents according to sex and some social and academic characteristics to provide a context for the analysed sample. Interval variables were represented with median [interquartile range], after evaluating whether they were non-normal with the Shapiro–Wilk test, histogram, mean/median comparison, skewness and kurtosis; only for the variable age of initiation of alcohol consumption, due to its normality, the mean ± standard deviation was used.
The bivariate analysis was carried out with the χ2 test for the association between positive BS and categorical variables, except in the cross between BS and alcohol consumption, being single and depression, in which cases Fisher's exact test was used because they had expected frequency values ≤5% in a percentage >20% of the expected values, while with the interval variables the sum of ranks was used; the Student's t test was used only for the crossover with the variable age of initiation of alcohol consumption due to its normal distribution and homogeneity of variances. For simple and multiple regression analysis, due to the large sample size, generalised linear models (GLM) and the Poisson family were used due to the qualitative nature of the dependent variable, log link function, robust models and the year as cluster, with which the crude prevalence ratio (PR) and adjusted prevalence ratio (APR), the 95% confidence intervals (95% CI) and the p values were obtained.
An initial model was generated with the variables with p < 0.2 in the simple backward stepwise regression eliminating variables one by one comparing with the preceding model, as well as the change in the goodness of fit with the Pearson χ2 test until achieving the reduced model, in which removing any variable did not make the model fit better. After that, it was verified whether adding new variables improved the model or not, resulting in the final multivariate model, which included the variables: depression, tobacco consumption, feeling that money is not enough, being a woman, and age at the start of marijuana consumption. A p-value < 0.05 was considered significant.
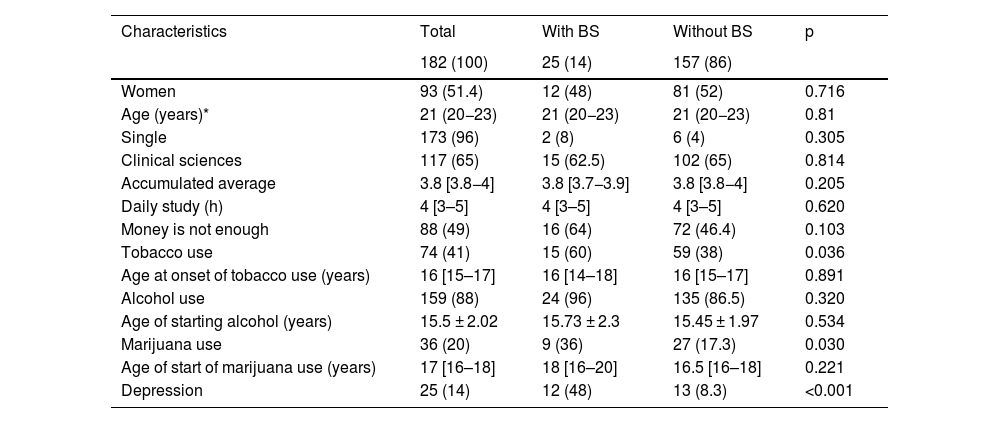
ResultsOf the 182 students who completed the survey —median age, 21 [20–23] years—, 51.4% (93) were women. 96% (173) were single, and 65% (117) were from clinical sciences. The cumulative academic average had a median of 3.8, with a score above 3.0 being considered passed. Forty-one percent (74) have used tobacco; 88% (159), alcohol and only 20%, marijuana (Table 1).
Social, economic, demographic and academic characteristics and their bivariate relationship with BS in students of a Colombian medical school, 2018.
| Characteristics | Total | With BS | Without BS | p |
|---|---|---|---|---|
| 182 (100) | 25 (14) | 157 (86) | ||
| Women | 93 (51.4) | 12 (48) | 81 (52) | 0.716 |
| Age (years)* | 21 (20−23) | 21 (20−23) | 21 (20−23) | 0.81 |
| Single | 173 (96) | 2 (8) | 6 (4) | 0.305 |
| Clinical sciences | 117 (65) | 15 (62.5) | 102 (65) | 0.814 |
| Accumulated average | 3.8 [3.8−4] | 3.8 [3.7−3.9] | 3.8 [3.8−4] | 0.205 |
| Daily study (h) | 4 [3–5] | 4 [3–5] | 4 [3–5] | 0.620 |
| Money is not enough | 88 (49) | 16 (64) | 72 (46.4) | 0.103 |
| Tobacco use | 74 (41) | 15 (60) | 59 (38) | 0.036 |
| Age at onset of tobacco use (years) | 16 [15–17] | 16 [14–18] | 16 [15–17] | 0.891 |
| Alcohol use | 159 (88) | 24 (96) | 135 (86.5) | 0.320 |
| Age of starting alcohol (years) | 15.5 ± 2.02 | 15.73 ± 2.3 | 15.45 ± 1.97 | 0.534 |
| Marijuana use | 36 (20) | 9 (36) | 27 (17.3) | 0.030 |
| Age of start of marijuana use (years) | 17 [16–18] | 18 [16–20] | 16.5 [16–18] | 0.221 |
| Depression | 25 (14) | 12 (48) | 13 (8.3) | <0.001 |
BS: Burnout Syndrome.
Values are expressed as n (%), median [interquartile range] or mean ± standard deviation. For the p values of the categorical variables, the χ2 test was used, except “consume alcohol” and “single” (Fisher's exact); for quantitative variables, Mann–Whitney U test, except “age of start of alcohol” (Student's t).
Of the total students, 14% (25) had BS, as well as depression. Of those who had BS, 48% (12) had depression (Table 1). Statistically significant differences (p < 0.001) are observed between suffering from BS and the different categories of depression (Table 2).
Categories of depression in relation to BS in students of a Colombian medical school, 2018.
| Variables | With BS, n (%) | Without BS, n (%) | Pa |
|---|---|---|---|
| Depression | |||
| Severe | 3 (12) | 3 (12) | <0.001 |
| Mild | 9 (36) | 144 (92) | |
| Normal | 13 (52) | 0 | |
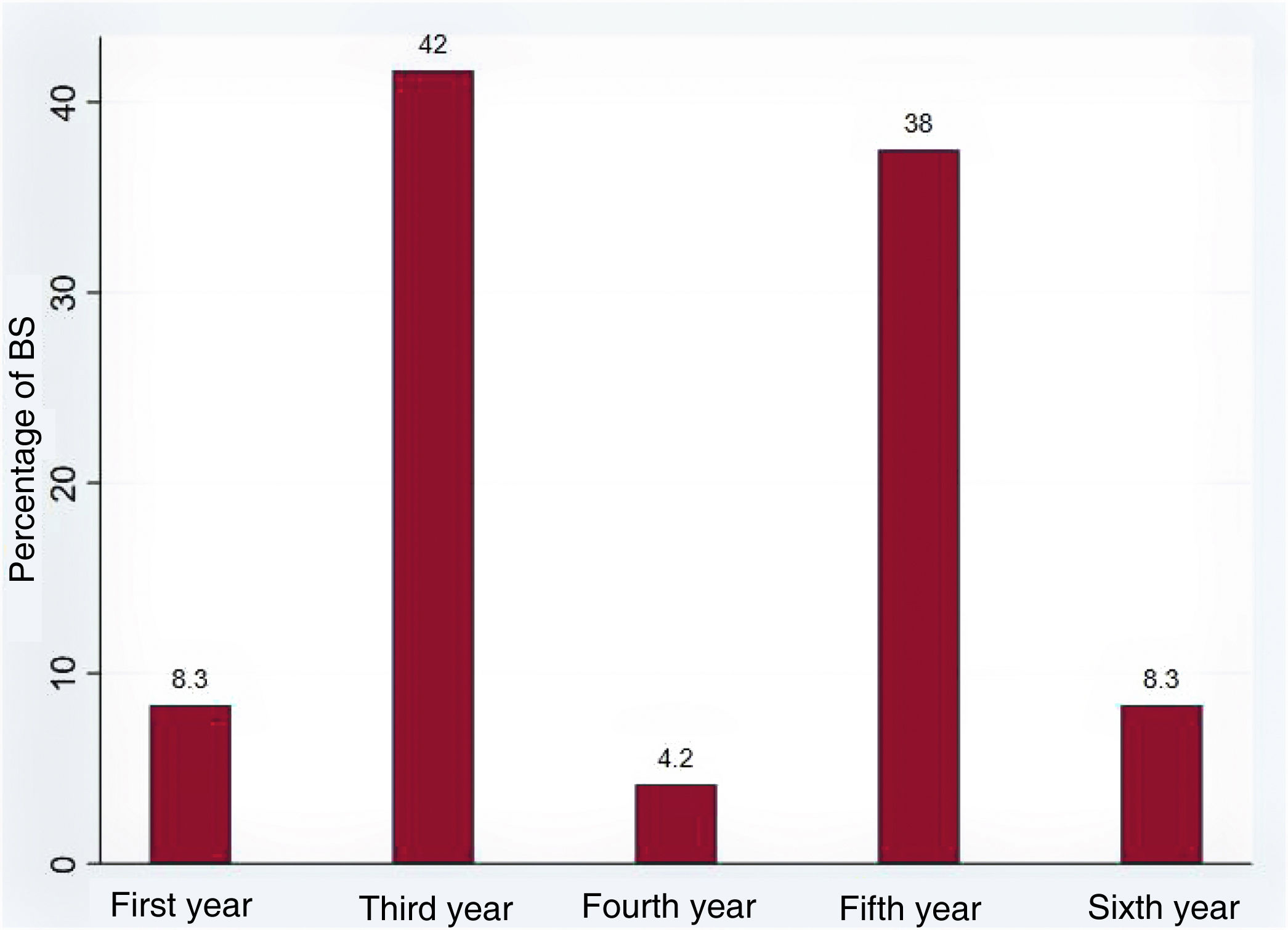
It is observed that, depending on the academic year completed at the time of the survey, there is more BS in key years: the third and fifth. In the third year, the transition from basic sciences to clinical sciences occurs, while in the fifth year, great academic activity occurs due to the subject of general surgery at the UPTC medical school. On the other hand, it is observed that the first and sixth years remain higher than the fourth year, and the sixth is the transition to the rotating medical internship (Fig. 1).

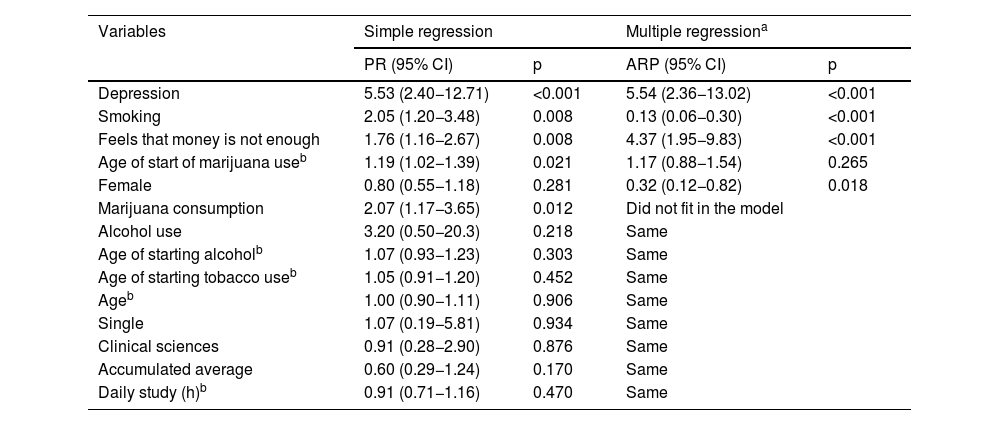
In the simple regression, an association was found between BS and depression (p < 0.001), using marijuana (p = 0.012), starting age of marijuana (p = 0.021), using tobacco (p = 0.008) and the feeling that money is not enough (p = 0.008). When performing the multiple regression analysis with the significant variables or with p < 0.2, after eliminating variables until reaching the final reduced model and adjusting for confounding variables, among those who suffered from BS there was a higher frequency of depression (ARP = 5.54; 95% CI, 2.36−13.02; p < 0.001) and feeling that money is not enough (ARP = 4.37; 95% CI, 1.95−9.83; p < 0.001), opposite relationship with tobacco consumption (ARP = 0.13; 95% CI, 0.06−0.30; p < 0.001) and being a woman (ARP = 0.32; 95% CI, 0.12−0.82; p = 0.018). On the other hand, the age of starting marijuana use was not significant, but contributed to the model (Table 3).
Simple and multiple regression of burnout syndrome in relation to depression and other variables in medical students from a Colombian medical school, 2018.
| Variables | Simple regression | Multiple regressiona | ||
|---|---|---|---|---|
| PR (95% CI) | p | ARP (95% CI) | p | |
| Depression | 5.53 (2.40−12.71) | <0.001 | 5.54 (2.36−13.02) | <0.001 |
| Smoking | 2.05 (1.20−3.48) | 0.008 | 0.13 (0.06−0.30) | <0.001 |
| Feels that money is not enough | 1.76 (1.16−2.67) | 0.008 | 4.37 (1.95−9.83) | <0.001 |
| Age of start of marijuana useb | 1.19 (1.02−1.39) | 0.021 | 1.17 (0.88−1.54) | 0.265 |
| Female | 0.80 (0.55−1.18) | 0.281 | 0.32 (0.12−0.82) | 0.018 |
| Marijuana consumption | 2.07 (1.17−3.65) | 0.012 | Did not fit in the model | |
| Alcohol use | 3.20 (0.50−20.3) | 0.218 | Same | |
| Age of starting alcoholb | 1.07 (0.93−1.23) | 0.303 | Same | |
| Age of starting tobacco useb | 1.05 (0.91−1.20) | 0.452 | Same | |
| Ageb | 1.00 (0.90−1.11) | 0.906 | Same | |
| Single | 1.07 (0.19−5.81) | 0.934 | Same | |
| Clinical sciences | 0.91 (0.28−2.90) | 0.876 | Same | |
| Accumulated average | 0.60 (0.29−1.24) | 0.170 | Same | |
| Daily study (h)b | 0.91 (0.71−1.16) | 0.470 | Same | |
95% CI: 95% confidence interval; PR: crude prevalence ratio; APR: Adjusted prevalence ratio.
A causal relationship can be estimated between suffering from BS and developing depression, as well as between being a woman and a lower risk of BS, since in the first case the logic and pathophysiological processes of mental illness allow us to determine that BS precedes depression, while in the second sex is a constant that logically precedes it; however, in the intersection with the variables of feeling that money is not enough and tobacco use, it is only possible to determine an association but not causality, since it is impossible to recognise what precedes what, since it is subject to temporality bias.
DiscussionAbout two in 10 students had BS. This result is worrying due to the high percentage it represents for the FCS, and the ideal is to take it to zero levels. The data obtained are similar to those reported in other studies, such as those carried out on medical students in Brazil — 14.9,20 1221 and 26.4%22— and the investigation of Popa-Velea et al.,23 with a prevalence of 15% of medical students in Romania. However, these results are considerably different from the frequencies by Nakandakari et al.24 in 158 medical students in Peru, which shows 30% positive BS, 30.6% of Pakistani medical students25 or 22.6% of students in Spain.26 This difference in the results obtained, with greater frequencies in the latter, may be due to multiple factors, such as a difference in the instrument used or the way of evaluating the diagnostic criteria of BS, since the majority of those that show results similar to those of this study are those who used the triple criterion (exhaustion, cynicism and negative self-efficacy), while those with higher results probably only took one or two criteria into account.
On the other hand, an association was found between depression and BS in the students of the faculty, which is also evidenced in a study with 6,351 Austrian doctors, which found that, compared to those not affected by BS, the Odds Ratio (OR) of suffering from major depression was 2.99 (95% CI, 2.21–4.06) for doctors with mild BS, 10.14 (95% CI, 7.58–13.59) with moderate BS, and 46.84 (95% CI, 35.25–62.24) with severe BS.27 Likewise in Lima, Peru, the information of 84 resident doctors was analysed; it was observed that the coexistence of BS and depressive symptoms was 32.9%.28 Whether BS is a form of depression or a different phenomenon is the subject of controversy, since it has been pointed out that both, in reality, could coincide in the same pathological area29,30 or at least be part of a common disease course, where one can lead to the other. The nature of such an association may be due to excessive study load, demanding educational requirements, and lack of time for leisure, family, and friends20 leading to chronic stress which, together with individual personality traits such as perfectionism and self-imposed standards, are finally expressed in depression, anxiety, aggression and anger, which remain under the influence of the physical and psychological exhaustion that accompanies frustration, fatigue, helplessness and a cynical attitude,20,31 that is, a joint development of said mental disorders.
Furthermore, in this study it is observed that tobacco uses acts as a protective factor against BS, which has been confirmed in various studies.32–34 Continuous tobacco use is considered a form of behavioural manifestation, functioning as a strategy to forget and distance oneself from one's environment, as well as a search for pleasure that is not achieved in daily academic/work activities. Stress has been classified as a predictor of students abusing tobacco and perceiving calming and relaxing effects after consuming it,34–36 which is why, although at the beginning of the BS condition there is an increase in smoking in order to obtain relaxation, in the long term it could act as a factor that protects against said chronic stress, something that, although partially beneficial, carries a greater number of harmful effects on health, so it should not be used.
It was found that BS is related to the feeling of not making ends meet with the money available monthly. This may be because the subjective sense of financial stability is a more reliable indicator of emotional well-being,20,37 and it is important to highlight that not being able to buy the basic basket of goods generates a greater presence of mental conditions38; if this persists, chronic stress may be found that would lead to BS.
Finally, women showed a lower frequency of BS, similar to a study in doctors and nurses in Peru,39 where men showed more BS, perhaps because "the influence of greater empathy in women and better understanding of emotional signals have influenced this association"39; however, there are many studies with contrary results, such as that of Serrano et al.8 in future doctors from Colombia, whose difference in percentages of positive BS was greater in women, as well as several others with opposite results or simply without statistical difference.11,14,40 This can be explained by the sample size and the only reality presented in this research, unlike larger studies that include multiple realities, which is decisive when making inferences with a variable that very possibly behaves as a confounder. Although it is true that there are studies with a similar result,39 it is also true that the majority are doctors and/or nurses who have already graduated, which can influence the data obtained.
A limitation of the study is the selection bias, since a random sampling was not carried out to choose the medical students, but this is not a problem, since the objective of the study was always to find the differences in BS according to depression and various associated factors. It was possible to control the temporality bias, always implicit in any cross-sectional study, by using main variables that logically allow us to determine which is the cause of the other. There could be an information bias, since the participants could not reveal information for fear of their identity being known; however, the study was conducted through a completely anonymous and self-administered survey, which did not request codes, identification or names. Measurement bias was controlled using nationally and internationally validated scales in the measurement of BS and depression using the MBI-SS and the Zung test respectively. Likewise, confounding bias could be reduced by adjustment with multivariate models. In addition, the study only takes into account a single population reality; however, the results are important because they show a reality in a Colombian health school regarding BS in association with depression and other factors, something poorly evaluated in future doctors in the country, which opens the doors to new research on the topic.
It is possible to conclude that BS in Medicine students at a university in Colombia has a positive association with depression and feeling that money is not enough to make ends meet; on the contrary, being a woman and having more tobacco consumption reduce the frequency of the syndrome.
FundingThis study received no specific funding from public, private or non-profit organisations.
Conflicts of interestThe authors declare that they have no conflicts of interest.
I would like to thank Dr. Cristian Pulido Medina, for his collaboration in redirecting the research idea and his guidance on the type of statistical analysis to use.
- •
Burnout syndrome is common in stressed medical students.
- •
Depression is common in medical students with burnout syndrome.
- •
Lack of money and its mismanagement can cause mental disorders.
- •
Tobacco, although harmful, reduces stress and burnout syndrome.
- •
Sex usually shows a significant association with burnout syndrome.
