


Premature ejaculation (PE) is a significant problem as it can cause a loss of sexual self-confidence and a significant deterioration in quality of life. The frequency of PE varies between 9% and 27%. In the current study, we aimed to compare the levels of the serotonin metabolite 5HIAA (5 hydroxyindole acetic acid) in the cerebrospinal fluid (CSF) of patients with and without PE according to IELT (intravaginal ejaculation latency time) in order to investigate the relationship of PE with CSF 5HIAA levels.
Materials and methodsA total of 60 male patients were included in the study who were planning to undergo surgery under spinal anesthesia, 30 in the patient (PE) group (all of the included patients had an IELT of <1min) and 30 in the control group (patients had an IELT of >1min). Levels of CSF 5HIAA were measured.
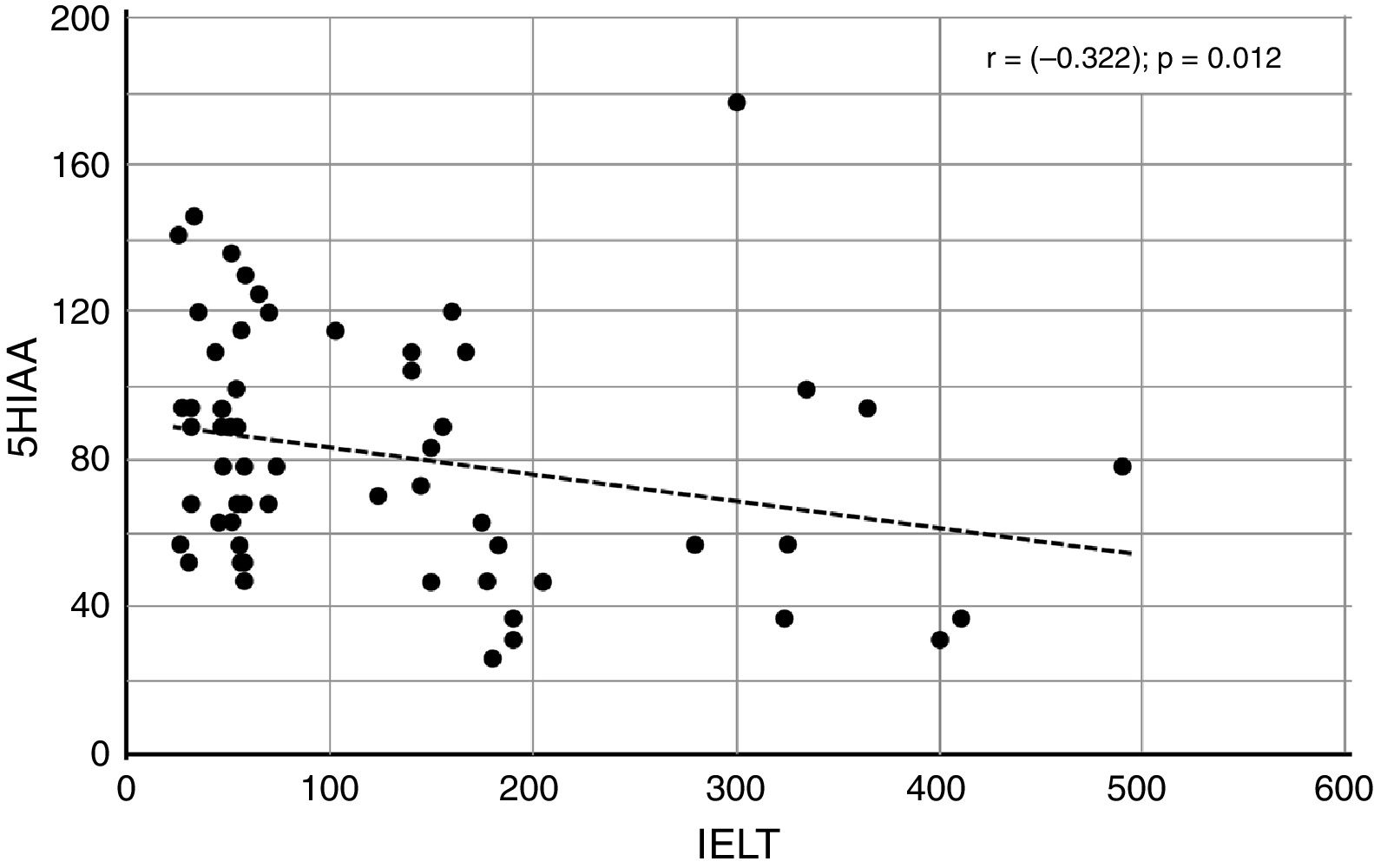
ResultsThere was a significant negative correlation between IELT and the 5HIAA variables in all patients (r=−0.322, p=0.012). Although the average 5HIAA levels (nmol/L) were higher in the patient group (86.80±28.33) than in the control group (76.44±35.91), this difference was not significant (p=0.22).
DiscussionResults of the current study bring new and different perspectives to the explanation of PE pathophysiology. There is a need for more specific and genetic studies to determine the best treatment for this common disorder.
La eyaculación precoz (EP) es un problema importante, ya que puede provocar una pérdida de confianza sexual en uno mismo y un deterioro considerable de la calidad de vida. La frecuencia de EP varía entre el 9 y el 27%. En este estudio, nuestro objetivo fue comparar los niveles del ácido 5-hidroxindolacético (5-HIAA), metabolito de la serotonina, en el líquido cefalorraquídeo (LCR) de pacientes con y sin EP según el tiempo de latencia eyaculatoria intravaginal (TLEI) para analizar la relación de la EP con los niveles de 5-HIAA en el LCR.
Materiales y métodosSe incluyeron en el estudio un total de 60 pacientes de sexo masculino que tenían prevista cirugía con anestesia intradural, 30 en el grupo de pacientes con EP (todos los pacientes incluidos tenían un TLEI <1min) y 30 en el grupo de control (los pacientes tenían un TLEI >1 min). Se midieron los niveles de 5-HIAA en el LCR.
ResultadosHubo una correlación negativa importante entre las variables TLEI y 5-HIAA en todos los pacientes (r=−0,322; p=0,012). Aunque los niveles medios de 5-HIAA (nmol/l) fueron más elevados en el grupo de pacientes (86,80±28,33) que en el grupo de control (76,44±35,91), esta diferencia no fue considerable (p=0,22).
DiscusiónLos resultados del presente estudio aportaron nuevas y diferentes perspectivas a la explicación de la fisiopatología de la EP. Es necesario realizar más estudios específicos y genéticos para establecer el mejor tratamiento de este trastorno frecuente.
Premature ejaculation (PE) is a significant problem as it can cause a loss of sexual self-confidence, decreased sexual satisfaction (in both the man and his partner), and a significant deterioration in quality of life.1 The frequency of PE varies between 9% and 27% depending on the definitions and methods used in many published studies.2,3
Intravaginal ejaculation latency time (IELT) is defined as the time between vaginal entry and discharge into the vagina. On average, IELT is between 2 and 7min; IELT<1min is regarded as premature ejaculation. Serotonin is the most investigated neurotransmitter in PE. Serotonin cannot cross the blood–brain barrier; thus, it is synthesized in the brain from its precursor, the amino acid tryptophan. Tryptophan is transported to the brain via a competing transport system. When it reaches the brain, the enzymes tryptophan hydroxylase and amino acid decarboxylase act on tryptophan to synthesize serotonin. This newly synthesized serotonin is stored in granules at the nerve endings and is released into the synaptic interval by nerve stimulation. A fraction of this serotonin is taken back into the neuron by the carriers, while the other part is destroyed by the mitochondrial enzyme monoaminoxidase (MAO) and converted to 5 hydroxyindole acetic acid (5HIAA). 5HIAA is a terminal inactive product and it has no negative or positive feedback on serotonin. There is a good correlation between 5HIAA and serotonin levels in cerebrospinal fluid (CSF).4
Data obtained from animal studies indicate that the central serotonergic system plays a major role in controlling the spinal ejaculation reflex.5 Serotonergic control of discharge can lead to faster, or even delayed, ejaculation. However, ejaculation itself is most likely not directly affected by the serotonergic system, but rather is influenced by other neurotransmitter systems in the spinal cord.6
In the current study, we aimed to compare the levels of the serotonin metabolite 5HIAA in the CSF of patients with and without PE according to IELT in order to contribute to the clarification of PE pathophysiology and to investigate the relationship of PE with CSF 5HIAA levels.
Materials and methodsIncluded in this study were 30 male patients who were planning to undergo surgery under spinal anesthesia (e.g., varicocele, hydrocele, ureteral stone, etc.) in the Department of Urology at the Bursa Specialized Training and Research Hospital Urology Clinic between April 2015 and October 2015. All of the included patients had an IELT of <1min, were sexually active in the last 6 months, and had complained of premature ejaculation since their first sexual experience. Thirty male patients who had an IELT of >1min, who were sexually active in the last 6 months, and who were also undergoing surgery under spinal anesthesia between April 2015 and October 2015 were enrolled in the study as controls. Patients were excluded from the study if they had been diagnosed with depression and/or were using SSRI for treatment, had a history of endocrine disease, had a mental disorder, had contraindications for regional anesthesia, and if they had sexual dysfunction other than premature ejaculation.
Once consent was received from each patient, he was told how to make an IELT measurement with the help of a stopwatch. The IELT was recorded by the patients in ‘seconds’ so that their sexual relations would not be affected.
Each patient and control in this study was questioned about his smoking history and each patient had his body mass index (BMI) calculated. Further, all patients filled out an AIPE (Arabic Index Premature Ejaculation) questionnaire.
After the preoperative preparations were completed, anesthesiologists were instructed to enter the subarachnoid space from L3/L4 and L4/L5 with a 25G spinal needle between 08:00 AM and 10:00 AM. Before anesthetic injection, 2cc of clear, uncontaminated CSF was collected in a polypropylene tube. CSFs were kept frozen at −80°C until further processing (centrifugation at 1000×g for 10min). The samples were transferred to the laboratory on dry ice without dissolution, and levels of 5HIAA were measured with Shimadzu HPLC (high performance liquid chromatography) and ECD (electrochemical dedector).
The study was approved by the hospital ethical center, and all patients signed informed consent.
Statistical analysisStatistical analyses were performed using the SPSS 22.0 statistical package program. The Shapiro–Wilk test was used to determine whether the data were normally distributed. A t-test was used to compare groups of normally distributed data, and a Mann–Whitney U test was used to compare groups of data that were not normally distributed. Relationships between variables were examined by Pearson and Spearman correlation coefficients. Pearson's Chi-square test was used to analyze the categorical data. Levels of p<0.05 were considered statistically significant.
ResultsA total of 60 male patients were included in the study, 30 in the patient (PE) group and 30 in the control group. There was no difference in the mean age of the patient group (35.40±8.7 years) and control group (36.1±7.3 years) (p=0.738). All of the patients in the patient and control groups were sexually active.
There were no significant differences between the patient and control groups in terms of BMI and smoking. Although the average 5HIAA levels (nmol/L) were higher in the patient group (86.80±28.33) than in the control group (76.44±35.91), this difference was not significant (p=0.22).
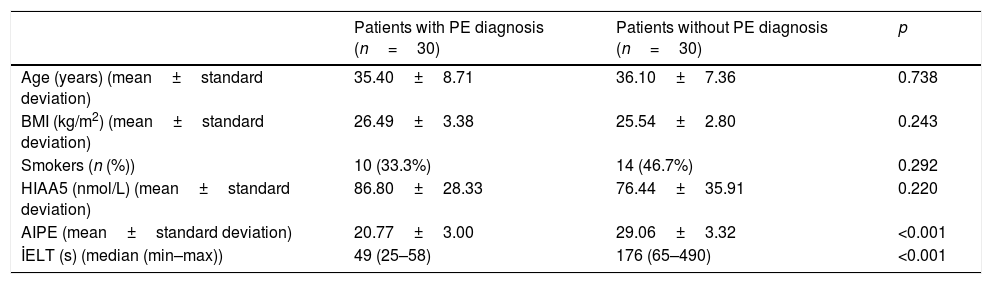
The mean IELT in patients with PE (49s) was significantly lower than that of the control group (176s) (p<0.001). In addition, the mean AIPE score of the patients with PE (20.77±3) was also significantly lower than that of the controls (29.06±3.32) (p<0.001) (Table 1).
Comparison of variables according to diagnosis.
| Patients with PE diagnosis (n=30) | Patients without PE diagnosis (n=30) | p | |
|---|---|---|---|
| Age (years) (mean±standard deviation) | 35.40±8.71 | 36.10±7.36 | 0.738 |
| BMI (kg/m2) (mean±standard deviation) | 26.49±3.38 | 25.54±2.80 | 0.243 |
| Smokers (n (%)) | 10 (33.3%) | 14 (46.7%) | 0.292 |
| HIAA5 (nmol/L) (mean±standard deviation) | 86.80±28.33 | 76.44±35.91 | 0.220 |
| AIPE (mean±standard deviation) | 20.77±3.00 | 29.06±3.32 | <0.001 |
| İELT (s) (median (min–max)) | 49 (25–58) | 176 (65–490) | <0.001 |
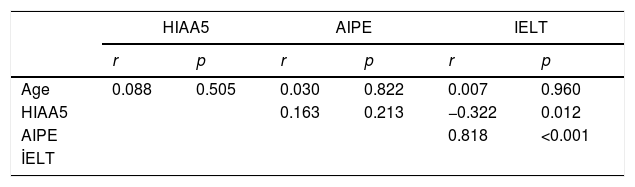
There was a significant negative correlation between IELT and the 5HIAA variables in all patients (r=−0.322, p=0.012) (Fig. 1). On the other hand, there was a significant positive correlation (r=0.818; p<0.001) between IELT and the AIPE variables (Table 2).

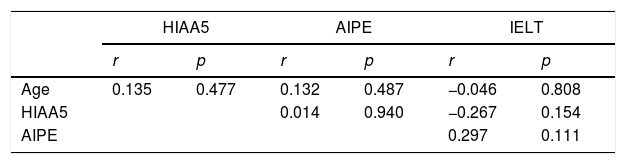
The correlation between AIPE and 5HIAA levels in PE-diagnosed subjects was not significant (p=0.154) (Table 3).
However, there was a significant negative correlation between IELT and 5HIAA variables in those without PE (r=−0.450, p=0.013). There were no significant differences between smokers and non-smokers in terms of IELT, AIPE, and CRF 5HIAA.
DiscussionPE is the most common male sexual dysfunction, although its etiology remains unclear. PE negatively affects quality of life. One study compared men with and without PE and their partners, and found that those with PE had lower sexual function and satisfaction levels, higher levels of personal stress, and more difficulty forming mutual harmony in comparison with non-PE group. The authors concluded that PE placed a significant psychological burden on the men, their partners, and their relationships.1
Previously published studies have argued that SSRIs can be used to increase serotonin in central nervous system ejaculatory centers, thereby prolonging IELT.7 In a human study, it is demonstrated that oral SSRI treatment increased 5HIAA levels in CSF.8 The study by Yang et al. reported that patients with PE had significantly lower serotonin levels in serum compared to controls, and that serum serotonin levels increased significantly after SSRI treatment.9 Contrary to expectations, in the current study, we found a significant relationship between IELT and CSF 5HIAA levels (r=−0.322, p=0.012) among all patients. This suggests that there may be a hyposensitivity at the receptor level as described in PE pathophysiology, and/or that there may be other receptors involved, and finally, that the body might be making an effort to increase serotonin.
One of the basic features of serotonergic nerve conduction is that neuron activity is monitored in order to reduce any increases in 5-HT levels in the synapse.10 Under normal physiological conditions, 5-HT (presynaptic) activates 5-HT1A autoreceptors in the cell bodies of serotonergic neurons. Activation of these 5-HT1A autoreceptors reduces the ignition of the 5-HT neurons and, consequently, decreases the release of 5-HT into the synaptic cleft between the neuronal cells from the presynaptic neuron (mechanism 1). After synaptic release of 5-HT, presynaptic 5-HT1B autoreceptors are activated and inhibit further 5-HT release to the synaptic cleft from the presynaptic neuron. This feedback mechanism most likely prevents the overstimulation of (post) synaptic 5-HT receptors (mechanism II). Another automechanism to inhibit the overstimulation of postsynaptic 5-HT receptors is the immediate reversal of synaptic 5-HT into presynaptic neurons in the serotonergic cell bodies and presynaptic terminations with 5-HT transporters (5-HTT) (mechanism III).
Studies with selective 5-HT receptors have shown that the 5-HT2C receptor plays a more critical role in ejaculation control than the other receptors. Mice given the non-selective 5-HT2C receptor agonist had a prolonged ejaculation period. However, the duration of ejaculation was shortened in mice given the selective 5-HT1A receptor agonist.11 Based on this evidence, Waldinger hypothesized that the cause of premature ejaculation in humans is 5-HT2C hyposensitivity and/or 5HT1A hypersensitivity.12 This approach might be compatible with our work. The correlation between increased CRF 5HIAA and decreased IELT in patients could be the result, but not the cause, of premature ejaculation. Elevated serotonin might also cause the desensitization of 5-HT2C receptors, resulting in a shortened duration of ejaculation.
In our current study, there was no correlation between IELT and CRF 5HIAA levels (p=0.154) in the PE group; however, the results were inversely proportional and significant (r=−0.450, p=0.013) when the entire patient group was taken into account. In addition, while the mean 5HIAA CSF level was higher in the patient group (86.80±28.33>76.44±35.91), the difference was not significant (p=0.22). However, we believe that this comparison should be made using larger patient groups.
ConclusionResults of the current study bring new and different perspectives to the explanation of PE pathophysiology. We believe that the amount of serotonin in CSF is inversely proportional to the duration of ejaculation and that there is a serotonin–receptor interaction that works well in people with longer ejaculation times. Further, we believe that this interaction is impaired in patients with PE, and that the duration of ejaculation is shortened in an effort to increase serotonin. To our knowledge, no other studies have been published in this area, and therefore, there is a need for this data to be supported by larger working groups.
In addition, there is a need for more specific and genetic studies at the receptor level in order to effectively elucidate the pathophysiology and determine the best treatment for this common disorder, which significantly affects the sexual and social life males and their partners.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
FundingThis research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors
Conflict of interestThere is no conflict of interest of any authors in relation to the submission.
Murat Demirbas coordinated and helped to draft the manuscript, Mustafa M. Aydos find patients and control group, Sedat Oner and Murat Sambel get results, performed statistical analyze and Canan Yilmaz collected samples, All authors read and approved the final manuscript.