


A previous survey on allergens used by Mexican allergists in their skin prick test (SPT) panel showed wide variation. Humidity varies in different zones of Mexico. This might lead to differences in natural exposure and allergic sensitisation throughout the country. We aim to describe the SPT sensitivity patterns in the different climatic zones in Mexico and to show the usefulness of a structured SPT chart-review including multiple clinics in obtaining these allergen sensitisation patterns.
Methods: A retrospective, structured chart-review of SPT results was undertaken in allergy clinics throughout Mexico. Ratios of SPT positivity were calculated for individual allergens, per climatic zone and nation-wide. Per allergen group the most important allergens were identified. Statistically significant differences between zones and the nation-wide data were tested with Pearson's Chi-squares test.
Results4169 skin test charts were recollected. The most important allergens causing sensitisation were very similar in different zones, despite climate variation. The allergen with highest ratio of SPT positivity was Dermatophagoides pteronyssinus (51%), with trees (Ash-27%, Alder-22%, Oak19%), and Bermuda grass (26%) as second and third. In the hot zones (humid and dry) Aspergillus was statistically significant more frequently than in more temperate zones. Cockroaches thrive in big cities and humid zones and Mesquite and Poplar in dry zones. Weeds are less important.
ConclusionMexico has its own SPT sensitisation pattern, which is different from America and Europe. A structured chart-review of SPT results is able to show this and might be a tool for allergists in other countries.
The only treatment of allergic rhinitis that interferes with the immunological alterations and the natural course of the disease is immunotherapy.1 As such, it may have long lasting and preventive effects2 and lately an indication for its early use in the therapy of allergic rhinitis and asthma has been supported by experts.3 Immunotherapy is allergen-specific; as a consequence an adequate diagnosis of the patient's allergies4 is mandatory for immunotherapy to be effective. The composition of the panel with which diagnostic skin prick testing is performed should include all relevant allergens in the region, taking into account cross-reactivity patterns between aeroallergens.5,6 However, in many regions in the world a full pollen mapping is not yet a reality, making it difficult for the allergists in those countries to adequately select with which allergens to test. The current study shows that a simple retrospective chart-review of previous skin prick test (SPT) results in allergists’ offices can give a clue to the skin test sensitivity of a population in defined climatologic zones.
In Mexico, only very recently attempts have been made to map the pollen count in the air of the major cities.7 As a result, a nationwide survey on which allergens are being used by Mexican allergists in SPT showed wide variation among centres. Moreover, some allergens recommended to be used in diagnostic testing in the United States and in Europe were not included.8 Climate and race differences between Mexico and other areas might lead to a dissimilar sensitisation pattern and oblige Mexican allergists to adjust their diagnostic allergen panel, but this is hard to accomplish, given the scarce aerobiological data.9 Also, at a national level sensitisation patterns could show divergence between regions, because of climatic diversity. Tropical humidity predominates in the Eastern and Southern part, as opposed to hot, dry desert areas in the North of the country. As such, Mexico is divided into different climatic zones by the National Institute for Statistics and Geography (Instituto Nacional de Estadística y Geografía, INEGI).10 This division will be used in our present survey.
The objective of our study is dual. In the first place we would like to describe the SPT sensitivity pattern of Mexico as a whole to contrast it with the patterns described in America and Europe. In second place we would like to investigate if differences exist in allergy sensitisation patterns in the various climatic zones within Mexico, as classified by INEGI (see below under methods, Table 1).
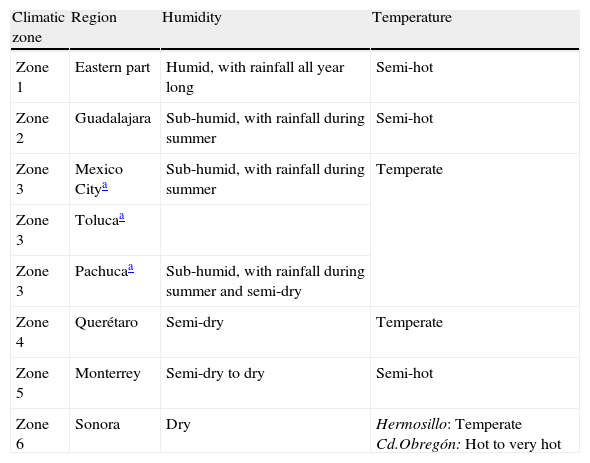
Classification into climatic zones of the study-centres according to the climatic characteristics of their geographical position.
| Climatic zone | Region | Humidity | Temperature |
| Zone 1 | Eastern part | Humid, with rainfall all year long | Semi-hot |
| Zone 2 | Guadalajara | Sub-humid, with rainfall during summer | Semi-hot |
| Zone 3 | Mexico Citya | Sub-humid, with rainfall during summer | Temperate |
| Zone 3 | Tolucaa | ||
| Zone 3 | Pachucaa | Sub-humid, with rainfall during summer and semi-dry | |
| Zone 4 | Querétaro | Semi-dry | Temperate |
| Zone 5 | Monterrey | Semi-dry to dry | Semi-hot |
| Zone 6 | Sonora | Dry | Hermosillo: Temperate Cd.Obregón: Hot to very hot |
This is an observational, cross-sectional retrospective study of SPT sensitivity in various regions in Mexico carried out from January 2007 to December 2008.
Allergists practicing in different regions in Mexico were asked to download into a standardised Excel spreadsheet the results of their last hundred positive SPTs, done during routine workup of clinically allergic patients in their practice, using the panel of allergen extracts, lancets and technique they normally use. Subjects of any age and sex were included, as long as they had a history of allergic rhinitis, conjunctivitis or asthma or allergic skin disease. Patients signed informed consent before the SPT, according to daily routine in each clinic.
The study-centres were classified according to the climatological characteristics of their geographical position. In the world map of climates, most of the territory of Mexico is situated in the temperate temperature zone, so the division used in this study is primarily based on humidity and secondary on average temperature, see Table 1. The results for Mexico City and its two neighbouring cities, Toluca and Pachuca, will be grouped, as their climates are quite alike.
For each centre the demographic data of the patients and SPT results were downloaded into a standardised Excel spreadsheet. Skin test results were tabulated as ‘positive’, ‘negative’ or ‘not done’ according to the physician's report on the clinic's SPT form and per clinic the ratio of SPT positivity was calculated for each allergen. Next, study-centres’ results were electronically grouped per climatic zone (see climatic zone distribution, Table 1). Finally, the frequency of SPT positivity was calculated per zone. Subsequently, an average value was given for the whole country. In some zones more data could be gathered than in other zones, with just one or two study-centres. For the nationwide data, all zones were given the same weight of importance, to avoid over-representation of certain zones with a lot of centres.
The routine SPT panel of allergens was used in each clinic, resulting in some allergens being tested in some clinics and not in others, as there is variation in the allergens included in the individual SPT panels of Mexican allergists.8 For that reason results are given as ratios dividing the total number of positive tests by the total number of tests done with each particular allergen. For figures and calculations only allergens which were tested in more than one study-centre will be taken into account.
The data will first be presented nationwide and then per allergen group. Per climatic zone the twelve allergens that give positive SPT with major frequency will be depicted. We will describe detectable trends in SPT sensitivity comparing humid with drier zones of the Mexican Republic. Finally, Pearson's Chi-squares test will be used to calculate if statistically significant differences can be found for SPT sensitivity of some allergens between certain zones and the nationwide data as expressed by the risk ratios and their 95% confidence intervals.
ResultsA total of 4169 positive skin prick tests were included.
Patient characteristicsPatients’ ages ranged between 2 and 65 years, with some exceptions. 34% of the patients were diagnosed with allergic rhinitis; 17%with asthma; 44%with rhinitis and asthma; and 5% with allergic skin disease.
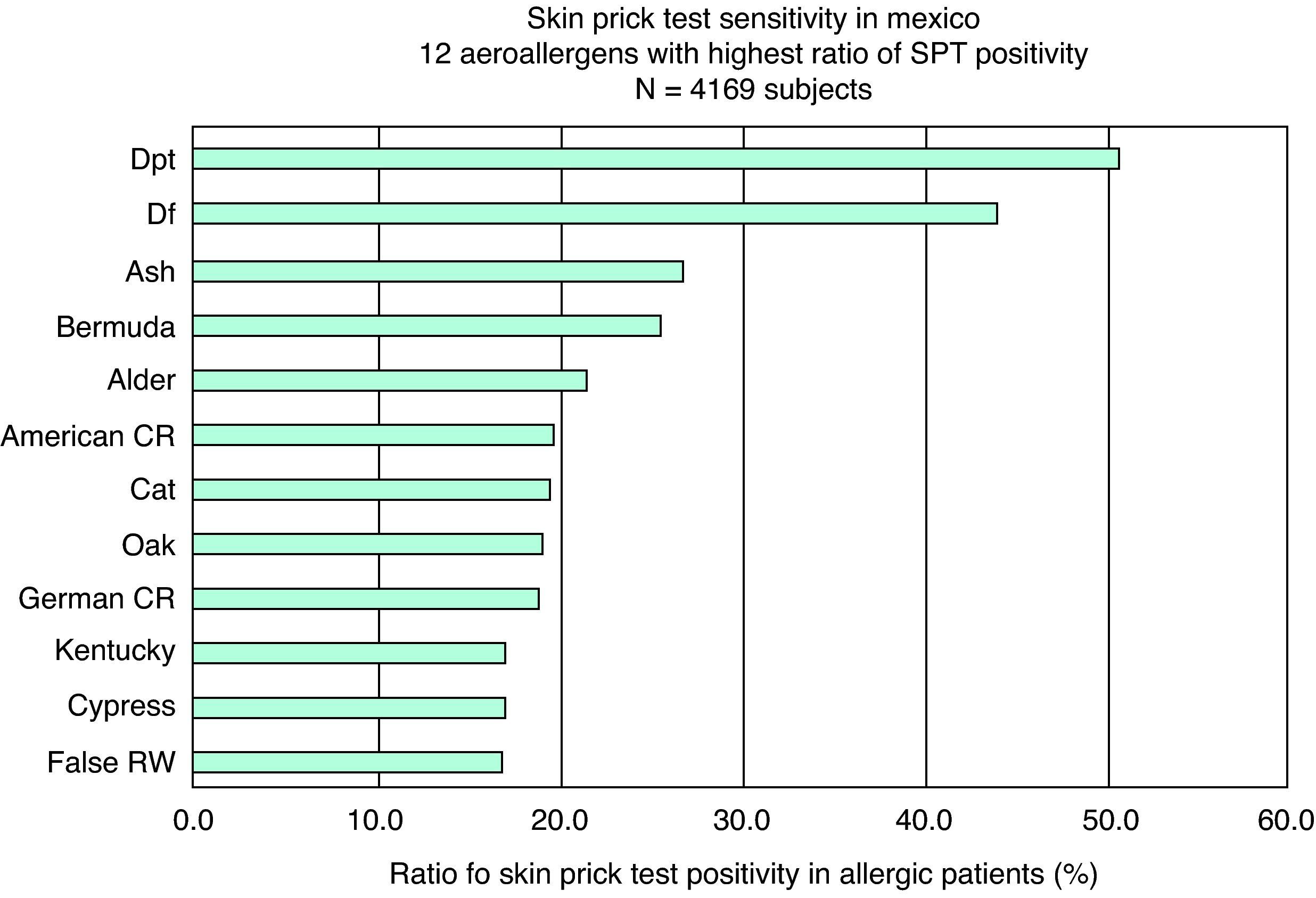
Nationwide resultsThe single allergen which is by far the most important in causing allergic sensitisation in all regions in Mexico is house dust mite, more commonly statistically significant than all other allergens (p<0.0001). For the whole of Mexico the five most important allergens are house dust mite; tree pollen; Bermuda grass; cockroach; and cat (Fig. 1). Although there are marked climate differences throughout Mexico, especially in humidity, this pattern is quite consistent in all zones. Some local differences can, however, be detected.

Nationwide data of skin prick test positivity for the 12 most frequent allergens in Mexican allergic patients. Data were obtained by calculating the average values for SPT positivity of each allergen in each of the six different climatic zones in Mexico. N = 4169 subjects. Pearson's Chi-squares (all with 1 degree of freedom): Dpt versus Ash p<0.0001 (Risk Ratio: 1.88; 95% CI: 1.755<0.0013 (Risk Ratio: 1.24; 95% CI: 1.0847<0.0001 (Risk Ratio: 1.36; 95% CI: 1.2228<0.0001 (Risk Ratio: 1.6; 95% CI: 1.4131
Looking at individual groups of allergens, for dust mites the extract that gives skin test positivity most frequently is Dermatophagoides pteronyssinus in all regions. Between 46-70% of all patients present a positive SPT to this allergen, with the exception of one centre in Queretaro, where only 21% of the patients had a positive result, reducing the average for that zone to 29%. Storage mites have shown positive SPT in 23-35% of the patients in one study-centre, but they have not been tested in other centres and therefore were not shown in the global presentation.
Trees, grasses, and weedsFor trees, Ash (Fraxinus) and Oak (Quercus) are the two extracts that provoke a positive skin test with major frequency in the humid, sub-humid and semi-dry areas and in one centre Alder (Alnus) was found with very high frequency (52%). However, in the dry areas Ash and Oak are much less important and the most allergenic trees are Mesquite (Prosopis) and Poplar (Populus).
The primary grass that sensitises Mexican allergic patients is Bermuda grass (Cynodon dactylon), followed by Kentucky Bluegrass (Poa pratense). Orchard grass (Dactylis glomerata) provoked a positive SPT in 34% of the patients in one centre, but this grass was not tested in other centres, so -as stated above- it was omitted from the global presentation. Grasses are more important in the drier areas of Mexico.
False ragweed (Franseria) is the weed with the highest prevalence of SPT positivity, followed by ragweed (Ambrosia). The distribution pattern of this pollen is interesting: it is only of importance in the drier northern regions. Only false ragweed, but not ragweed, is among the 12 most important allergens nationwide, ranked 12.
MouldsMoulds are a frequently found allergic sensitiser for patients in hot climates, both humid and dry (respectively, Veracruz-Eastern region and Yaqui valley-Northern region). Of all moulds Aspergillus has the highest percentage of positive skin tests.
Other inhalantsOne of the most important allergens causing SPT sensitivity in Mexico are cockroaches, both the American (Periplaneta Americana) and the German (Blatella germanica). This allergen has a clear distribution in big cities and humid areas, where the ratio of sensitised patients is higher than for cat. It is of minor importance in smaller cities with a semi-humid to dry climate (Toluca, Pachuca, Querétaro) where SPT positivity to cat becomes more frequent.
Results per climatic zoneIf the regions of the Mexican Republic are divided according to humidity, taking temperature only as a secondary factor (see Table 1), the following trends can be observed when analysing results from Zone 1 to Zone 6.
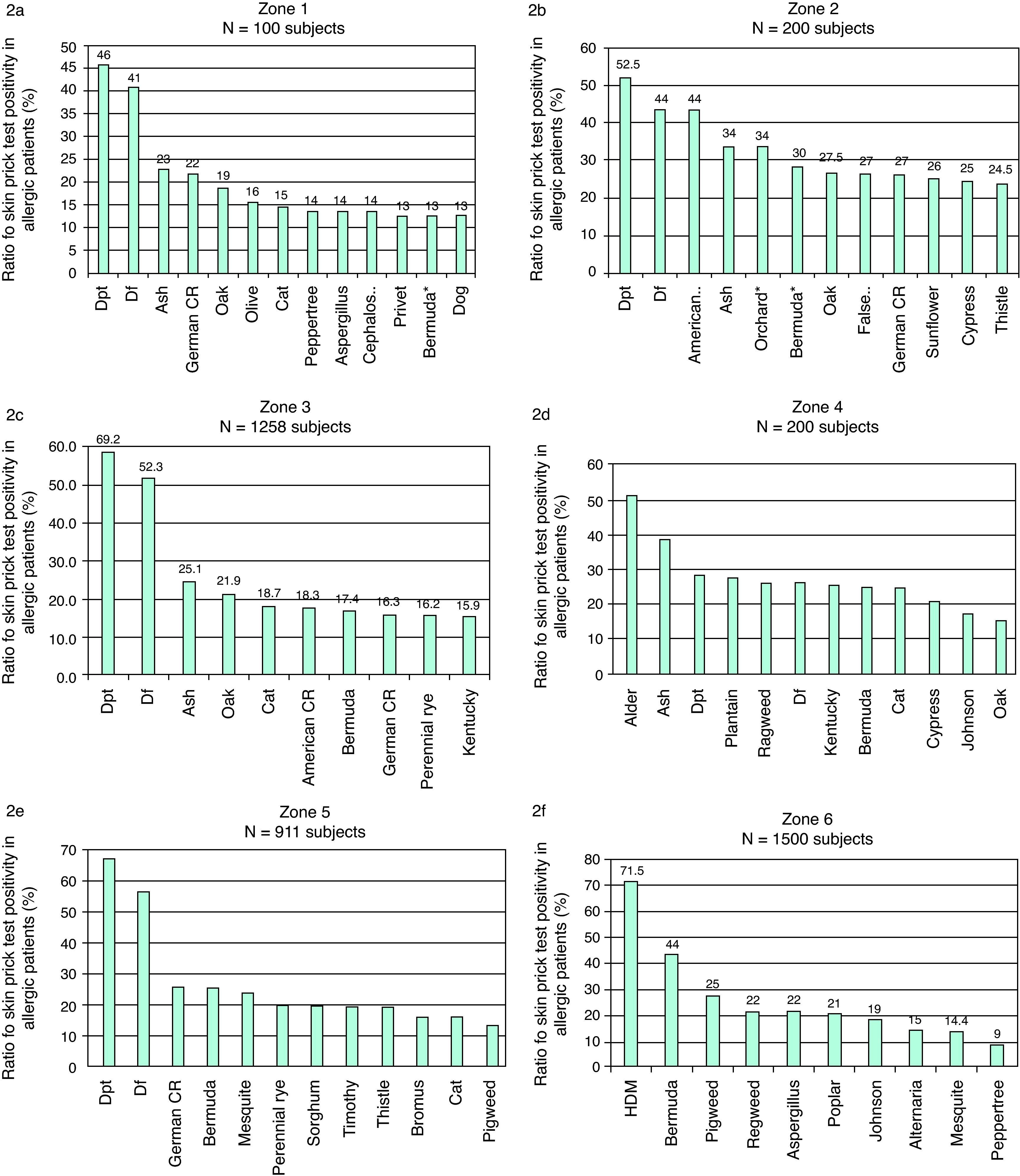
Data from the Eastern region of the National Health Security Institute (Instituto Mexicano del Seguro Social), involving mostly the humid state of Veracruz, show house dust mite is the most important allergen, followed by various trees and cockroaches. In this hot and humid climate Zone 1, moulds frequently cause allergy. Only around 10% of the patients are sensitised to weeds and grasses (Fig. 2a).
 Zone 1, Eastern part of the country, semi-hot, humid, with rainfall all year long. N=100 subjects. 2b) Zone 2. Guadalajara, semi-hot, sub-humid, with rainfall during summer. N=200 subjects. 2c) Zone 3. The centre of the country including Mexico-city, Toluca and Pachuca, temperate temperature, sub-humid, with rainfall during summer. N=1258 subjects. 2d) Zone 4. Querétaro, temperate temperature, semi-dry. N=200 subjects. 2e) Zone 5. Monterrey, semi-hot, semi-dry to dry. N=911 subjects. 2f) Zone 6. Sonora, with temperatures ranging from temperate to very hot, dry. N=1500 subjects.")
Skin prick test positivity for 10 to 13 most frequent allergens in Mexican allergic patients living in:
2a) Zone 1, Eastern part of the country, semi-hot, humid, with rainfall all year long. N=100 subjects.
2b) Zone 2. Guadalajara, semi-hot, sub-humid, with rainfall during summer. N=200 subjects.
2c) Zone 3. The centre of the country including Mexico-city, Toluca and Pachuca, temperate temperature, sub-humid, with rainfall during summer. N=1258 subjects.
2d) Zone 4. Querétaro, temperate temperature, semi-dry. N=200 subjects.
2e) Zone 5. Monterrey, semi-hot, semi-dry to dry. N=911 subjects.
2f) Zone 6. Sonora, with temperatures ranging from temperate to very hot, dry. N=1500 subjects.
In the sub-humid zones (Guadalajara, Mexico City, Pachuca, Toluca) apart from house dust mites, trees and cockroaches, grasses become important with Bermuda grass in the first place (Fig. 2b-c).
Moving on to the semi-dry climate of Queretaro (Zone 4, Fig. 2d) weeds start appearing among the 10 most important allergens, and in still drier climates -apart from the importance of weeds- there is a change in the families of trees that cause a wheal with the SPT, moving away from the Fagaceae (Quercus), Betulaceae (Alnus) and Oleaceae (Fraxinus, Ligustrum) toward trees which are more resistant to drought: Mesquite and Poplar (Zones 5 and 6, Figs. 2e and f).
SPT positivity for Aspergillus is more frequent in the Eastern zone than in the rest of Mexico (with the exception of the North) with statistical significance (p=0.003, Risk Ratio: 2.25; 95% CI: 1.351<R.R.<3.757). In the Northern dry and hot zone both Aspergillus (p < 0.0001; Risk Ratio: 3.36; 95% CI: 2.8039
PolysensitisationMost of our study-subjects presented polysensitisation, with monosensitised patients varying between zero (Civil Hospital of Guadalajara ‘Juan I Menchaca’, Guadalajara) and 10.4% (Hospital Juarez, Mexico City).
DiscussionWith the current survey we showed that a simple well-structured chart-review of SPT positivity in multiple clinics can result in useful data on sensitisation in allergic patients, which are in line with the climatic conditions reported by national institutes.
For the allergic patients in Mexico the most frequent allergen causing SPT sensitivity is Dermatophagoides pteronyssinus, followed by trees, and cockroaches. Some patterns can be detected in SPT sensitivity according to the different climatic zones in Mexico, varying from tropical humid, through sub-humid temperate to hot dry desert climates. Statistically significant differences can be found between the frequencies with which certain allergens cause SPT sensitivity in some zones in comparison with others.
The present investigation is a retrospective study in which each clinic was allowed to use their own SPT routine, without standardising between centres. As such, allergen panels, quality of the allergens used for SPT and skin prick test technique varied between centres.11 These are probably confounding factors. To reduce bias, the allergens that were tested in one only study-centre were not taken into account for the presentation of the global data. In some cases, however, their SPT positivity was over 20%. Those cases have been mentioned in the results section, as they might present important exploring areas for the future: for example the storage mites and Orchard grass.
Two zones had a very high number of patients, which might skew the nationwide results if they had been given a weight according to the number of patients included. To avoid this confounding factor it was decided to give the same weight to all zones for the calculation of the nationwide data and only average the percentages.
Even though our study has the methodological shortcomings of being a retrospective, observational study, some interesting points can be learnt from the present work. Despite the fact that there are large climate differences throughout the Republic of Mexico, in all tested areas Dermatophagoides pteronyssinus is the most important allergen. Three previous studies in Mexico City pointed at this same allergen12 (Espinosa Leal, personal communication; Cariño, personal communication). This is in accordance with the findings of both a pan-European13 and an American14 study on the prevalence of SPT sensitivity, and of a very recent study in France,15 all reporting that the main allergen causing sensitisation is house dust mite. However, the second most important allergen found in Mexico is Ash tree pollen, as opposed to grass pollen in the pan-European, American and French reports. In Italy, grass pollen was far more important than perennial allergens.16 The third allergen in the NHANES III survey in the US was ragweed, immediately followed by cockroach; in the pan-European survey;13 and the French15 study it was cat. In Mexico, cockroach and cat sensitisations were also frequent, coming in fifth and sixth places, preceded by Bermuda grass and Alder.
Looking at individual groups of allergens we find that the specific skin test sensitivity to grass differs in Mexico from the US and Europe. In Mexico, Bermuda grass sensitisation is by far the most frequent, while in the US the prime grass allergen is Lolium perenne and in Europe it is Phleum pratense, two species with high cross-reactivity, which they do not share with Bermuda grass.4,6 The most important trees causing skin sensitisation in allergic patients in Mexico were Ash (Fraxinus), Alder (Alnus) and members of the Cupressaceae family, all trees growing in moist to wet soil. They are somewhat related to Oak and Birch, the most frequent skin sensitisers in the US and Europe, respectively, but have definitely their own allergens and should as such be skin prick tested separately.4 In the semi-dry to dry climate zone in the North of Mexico these trees can hardly be found. The few trees still thriving under these conditions are trees resistant to droughts, adapted to arid soil due to an extremely deep root system: the Mesquite (Prosopis) and Poplar (Populus). Finally, ragweed, a very important cause of allergy in the US, is not of prime importance in Mexico. In our study the weed most frequently causing skin sensitivity was false ragweed, Franseria, a plant growing in the dry desert climate zone in North Mexico and part of the family of the Ambrosiaceae.17 In general, we found weeds gained some significance in this Northern zone, but in many other areas weeds did not even appear among the first 12 allergens.
Polysensitisation in Mexico is very common and in some centres no monosensitised patients could be detected, this is in contrast to the recent French study reporting 36% of the patients to be monosensitised.15
Aerobiological reports are still scarce in Mexico, but some data do exist for Mexico City and Monterrey.18 Results from this kind of air-sampling only partly reflect what can be seen in the sense of skin sensitivity. Some pollen is highly concentrated in the air during a given season, but causes relatively few allergic reactions (e.g. Cypress). For the selection of the optimal SPT panel, aerobiology data can only be of limited help and analysing results from previously done skin tests might be of higher value.
For the future two further studies might be planned, to even further disclose the aeroallergens that cause allergic symptoms in Mexican patients. In the first place, a similar study as the one presented here, but using a prospective design and the same panel of allergens, allergen provider and technique of application and documentation in all study-centres. This could lead to more reliable results. In such a study pan-allergens, such as lipid transfer protein and profilin should also be included in the test-panel. In the second place, in vitro allergy diagnostic testing is gaining in accuracy with speed. One of the techniques -using micro-array plates- allows for the detection of specific IgE to a vast range of allergenic epitopes with minor quantities of patient's sera. This technique might give way to the discovery of other aeroallergens to which the patient is sensitised and that are not routinely used in skin prick testing.
It can be concluded that the most important aeroallergens in Mexico, causing SPT positivity in clinically allergic patients, are partly dissimilar from the most important allergens found in European and American surveys. A specific sensitisation pattern for Mexican allergic patients is presented, given the fact that the grasses and weeds that cause positive SPT most often in Mexico are different from the ones found in the United States of America and in Europe. In general, allergists should be well acquainted with the skin test sensitisation pattern of their population, in order to select the optimum SPT panel for their allergy clinic. Using solely aerobiological data to select the optimal skin testing panel is not recommendable. A retrospective observational study of structured SPT chart-review, such as the one here presented, is more suitable for this goal, is not too laborious to conduct and could raise useful data also in other parts of the world to guide allergists in the correct selection of their SPT allergen-panel.
FundingThe study has been conducted as part of a set of studies undertaken by the Immunotherapy Committee of the Colegio Mexicano de Inmunología Clínica y Alergia (CMICA), and was done with the good-will of the participating centres in the spare time of the investigators, without any external funding.
Conflict of interestNo specific conflict of interest can be detected.
We would like to thank the following allergists, many of them Head of the Department of Allergy of their respective hospitals: José G. Huerta-López of the National Institute of Pediatrics, Mexico City; Blanca del Río Navarro and Virginia Blandón of the Pediatric Hospital of Mexico, Mexico City; María Isabel Rojo and Daniel Aguilar of Hospital Juarez, Mexico City; and Sandra Nora González Díaz from the University Hospital of Nuevo León, Monterrey, for allowing us to compile data from the files of their departments in the different hospitals throughout Mexico City. Moreover, we thank José Cariño for sharing his personal data of a previous study on the subject carried out in Mexico City around the end of the past century.
