





In daily surgical practice, inguinal hernioplasty is a frequent procedure that is frequently accompanied by severe postoperative pain. Multiple regional blocks have been described for analgesia after such operations. Retrolaminar block (RLB) is a paravertebral block (PVB) variant that provides excellent analgesia and reduces the risk of complications. This prospective trial compared the analgesic efficacy of PVB and RLB in the inguinal hernioplasty.
MethodsThe 56 patients included were randomly assigned into two equal groups according to the block performed under ultrasound guidance at the T12 level: PVB group (28 patients) and RLB (28 patients). Time until the first rescue analgesia was our primary outcome. Other outcomes included the time to perform the block, changes in intraoperative hemodynamic parameters, postoperative VAS, 24-h morphine consumption, the level of patient satisfaction, and the incidence of block-related complications.
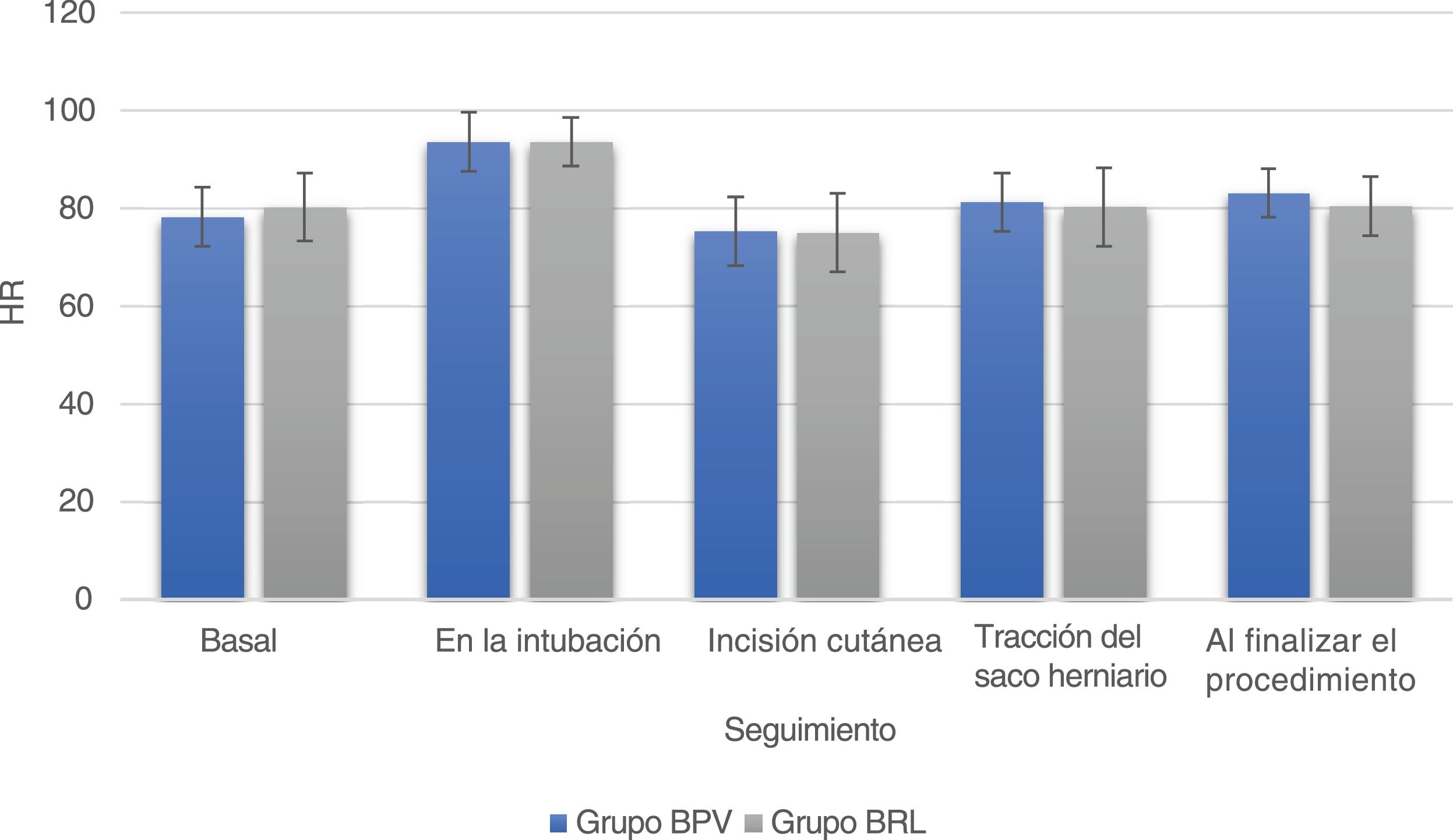
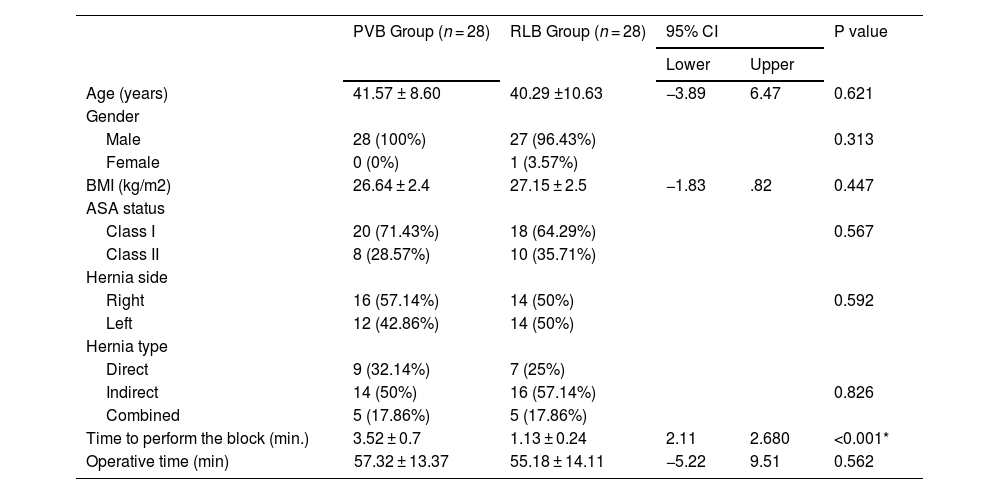
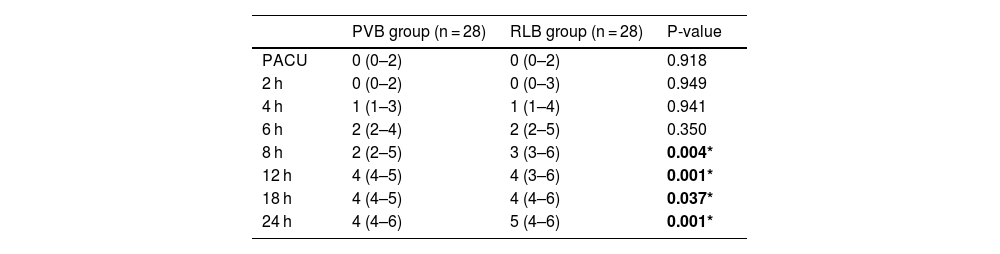
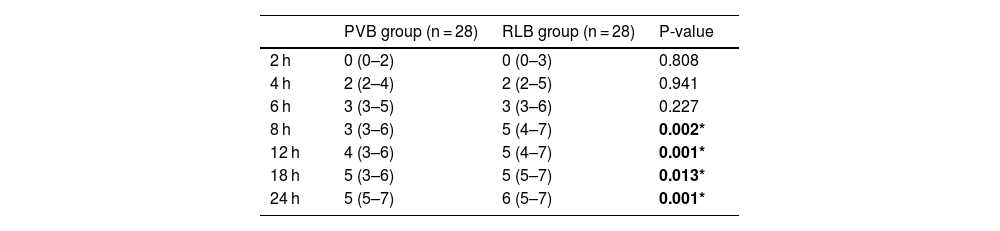
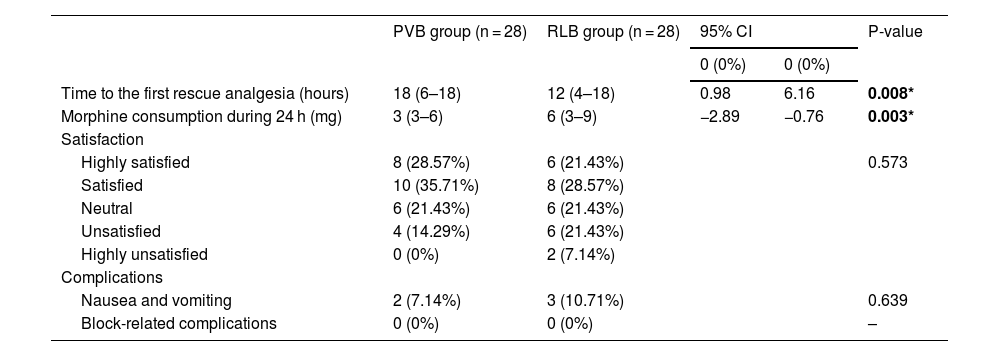
ResultsDemographic data were comparable in the two groups. However, the time needed for the block was significantly shortened with the RLB (p < 0.001). Patients in the PVB groups expressed better pain scores and lower opioid consumption. Additionally, the time to the first call for opioid analgesia showed a significant prolongation in association with the PVB. There was no discernible difference in the frequency of adverse events and recorded MAP and HR.
ConclusionThe PVB has a superior perioperative analgesic profile compared to the RLB, which manifested in the prolonged duration to the first rescue analgesics, better pain scores, and less opioid consumption, with no significant increase in block-related complications.
La hernioplastia inguinal es un procedimiento quirúrgico común que está asociado frecuentemente a dolor postoperatorio severo. En este context, se han descrito muchos bloqueos regionales diferentes. El bloque retrolaminar (BRL) es una variante del bloqueo paravertebral (BPV) que aporta analgesia excelente y reduce el riesgo de complicaciones. Este estudio prospectivo compara la eficacia analgésica de BPV y BRL en la hernioplastia inguinal.
MétodosSe aleatorizó a los 56 pacientes incluidos en dos grupos: el grupo BPV (28 pacientes) y el grupo BRL (28 pacientes). Todos los bloqueos nerviosos fueron realizados con guía ecográfica en T12. La medida del resultado primario fue el tiempo hasta la primera solicitud de analgesia de rescate. Los resultados secundarios incluyeron el tiempo necesario para realizar el bloqueo, los cambios de los parámetros hemodinámicos intraoperatorios, el dolor postoperatorio calificado con la escala visual analógica (EVA), el consumo de morfina durante 24 horas, la satisfacción del paciente, y la incidencia de complicaciones relacionadas con el bloqueo.
ResultadosLos datos demográficos fueron similares en ambos grupos. El tiempo necesario para realizar el bloqueo fue significativamente menor en el grupo BRL (p < 0,001). Los pacientes del grupo BPV tuvieron menores puntuaciones EVA, menor consumo de opioides y un tiempo significativamente mayor hasta la solicitud de opioides de rescate. No existió diferencia discernible en cuanto a la frecuencia de episodios adversos y cambios de la presión arterial y frecuencia cardiaca.
ConclusiónLos pacientes que recibieron BPV perioperatorios reflejaron un tiempo más prolongado hasta la primera solicitud de analgesia de rescate, menores puntuaciones para el dolor, menor consumo de opioides, y ausencia de incremento significativo de complicaciones relacionadas con el bloqueo, lo cual refleja que esta técnica es superior a BRL en la hernioplastia inguinal.

