



In this article we highlight the importance of cardiac imaging techniques and proper differential diagnosis to tackling the evaluation of cardiac masses in the right chambers.
En este artículo queremos resaltar la importancia de las técnicas de imagen cardiaca en el adecuado diagnóstico diferencial a la hora de abordar el estudio de las masas cardiacas en las cavidades derechas.
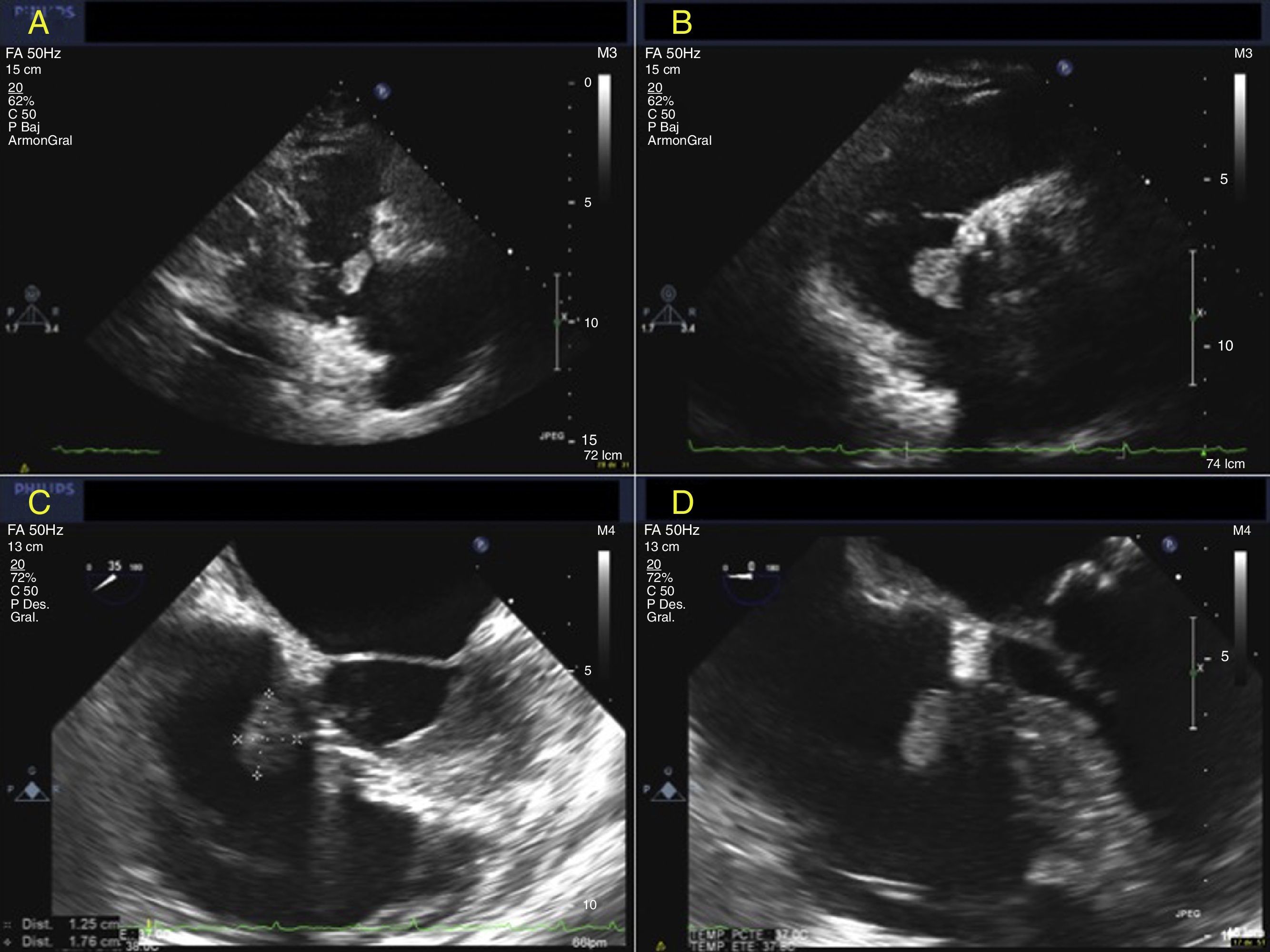
A 68-year old woman with previous aortic valve replacement with a mechanical prosthesis three years ago was admitted to our hospital with a recent onset atrial fibrillation. Transthoracic echocardiography was performed. It described a well-circumscribed polypoid mass in the right atrium which seemed to be attached to the septal leaflet of the tricuspid valve (Fig. 1A and B). Subsequently a transesophageal echocardiography confirmed this finding (Fig. 1C and D: 17mm×12mm ovoid mass without obstructing tricuspid valve). Otherwise, right cavities were normal and prosthesis had also a normal function.
 and (B) TTE polypoid mass in the right atrium attached to the septal leaflet of the tricuspid valve. (C) and (D) Transesophageal echocardiography confirmed de previous findings.")
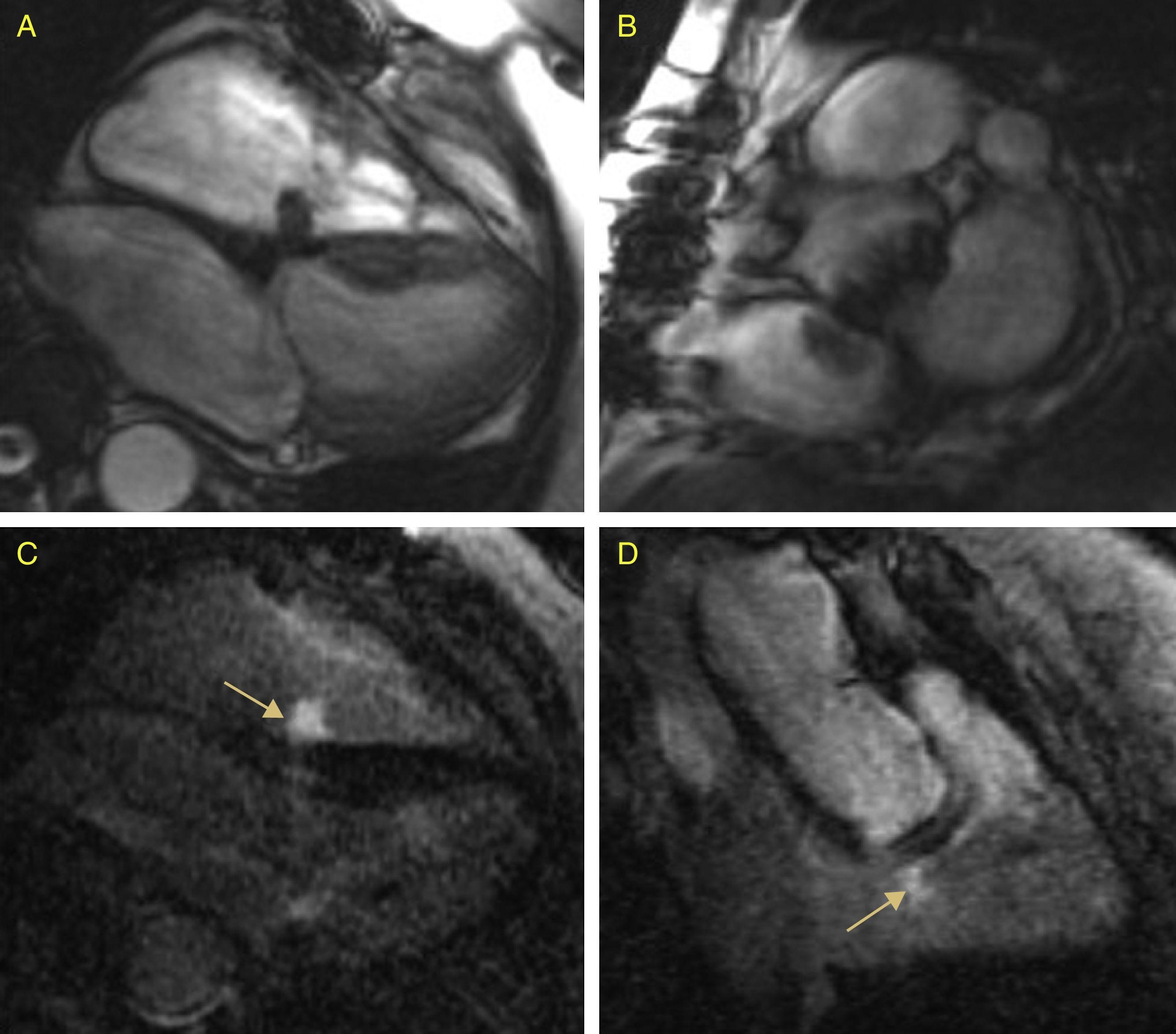
In the absence of clinical signs of endocarditis, suspected diagnosis of tumor was established.1,4 Cardiac MRI for a better characterization was performed. It confirmed a well-defined mobile mass in the right atrium attached to the septal leaflet of the tricuspid, hypointense in gradient echo sequences and with early and late heterogeneous gadolinium hyperenhancement (Fig. 2A–D). Once the study was completed the most likely diagnosis of myxoma was established.1–3
 and (B) Gradient echo sequences. A mass in the right atrium attached to the septal leaflet of the tricuspid, hypointense. (C) and (D) Enhancement sequences. Early and late heterogeneous gadolinium hyperenhancement.")
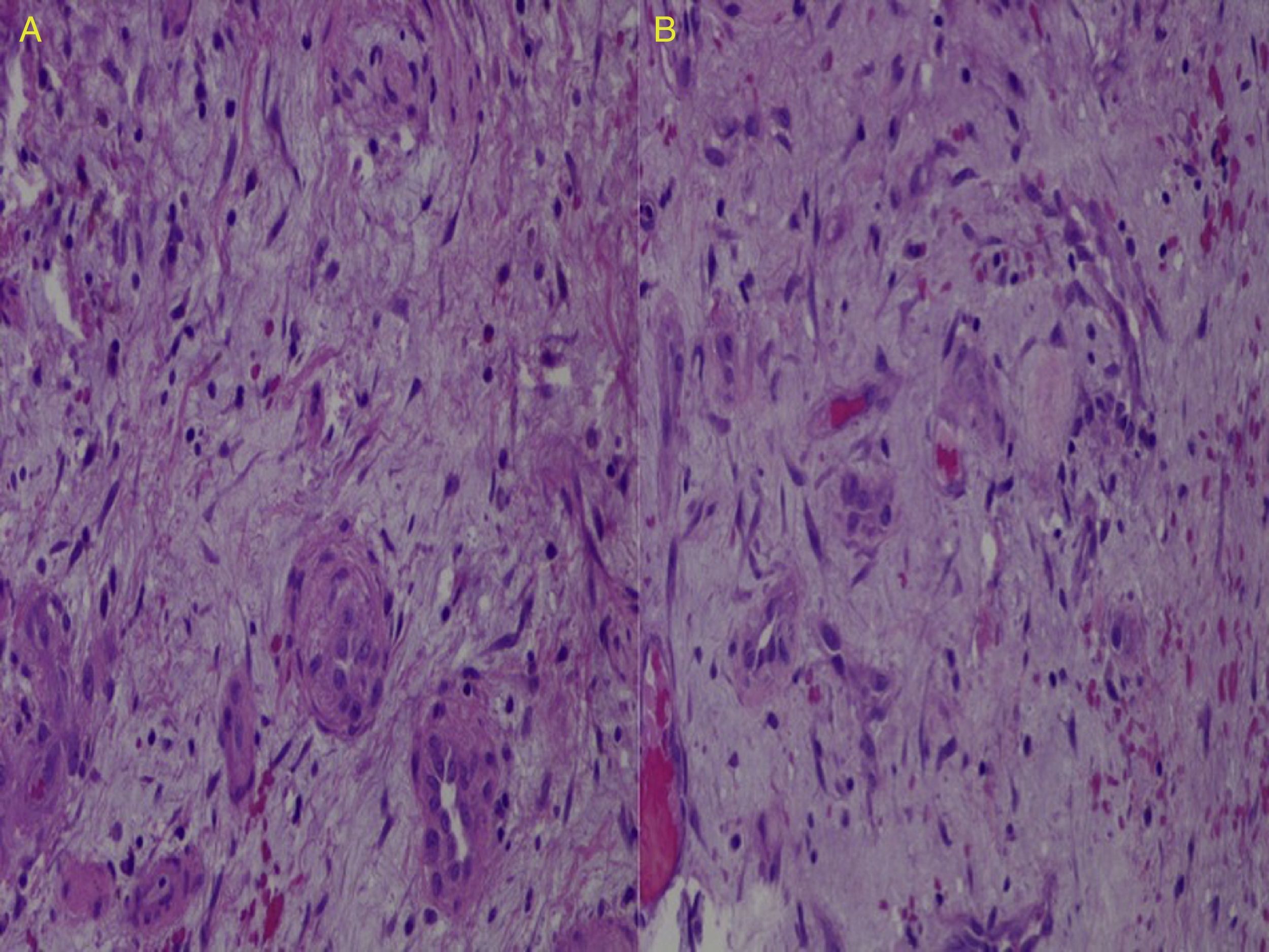
Surgical resection was performed. Intraoperative biopsy was compatible with myxoma and histopathological study confirmed the diagnosis (Fig. 3 A and B)

Intracardiac primary tumors are rare and highly variable in their clinical expression. It can range from incidental diagnosis, as in our case, to sudden death. Although myxomas are the most frequent primary tumors, right atrial is an atipical location leading to a diagnostic dilemma.2–4 Differential diagnosis with malignant tumors, metastasis, vegetations and even with normal variants must be taken into account.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this investigation.
Confidentiality of dataThe authors declare that no patient data appears in this article.
Right to privacy and informed consentThe authors declare that no patient data appears in this article.

