




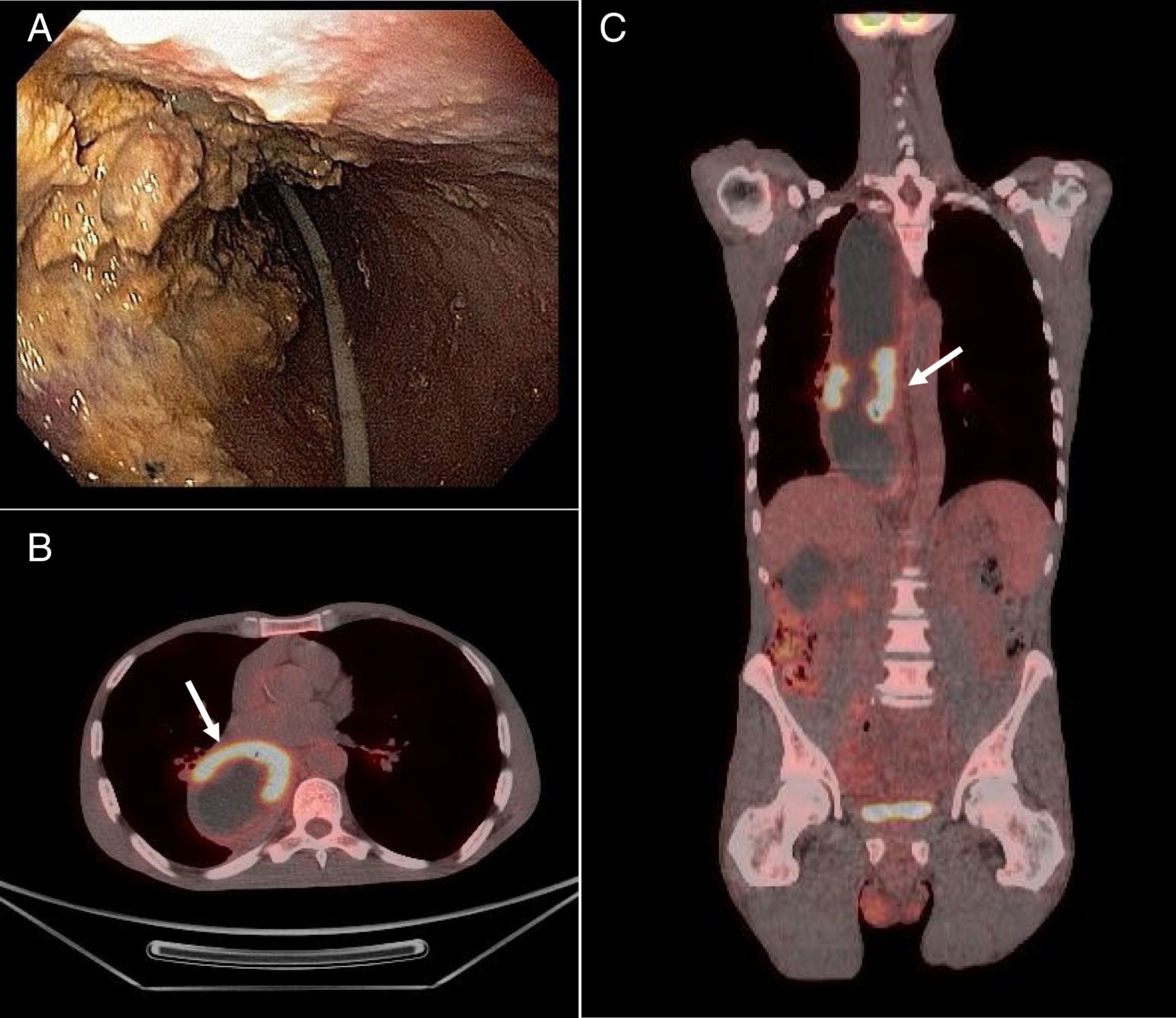
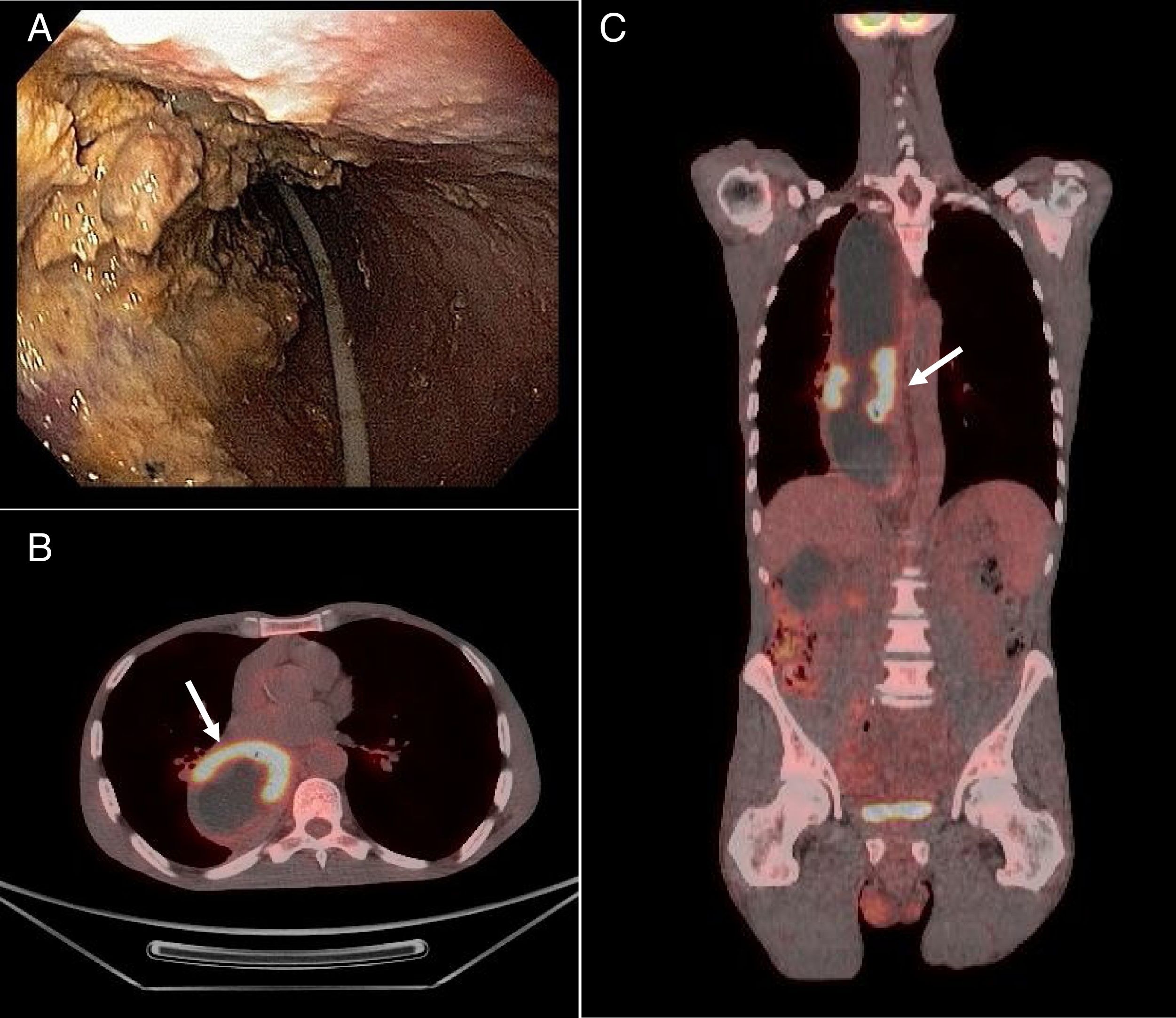
A 62-year-old man from a rural area in Brazil presented with progressively worsening dysphagia over 2 years. An upper gastrointestinal-endoscopy showed an enlargement of the esophagus and an infiltrative lesion located 25cm from the upper incisor teeth (Fig. 1A). Biopsy revealed a squamous cell carcinoma (SCC) and serologic test for Trypanosoma cruzi was positive. Positron-emission tomography showed an increased glycolytic metabolism in a semicircular thickening of the esophageal left anterolateral wall (Fig. 1B and C). These findings were consistent with the diagnosis of locally-advanced SCC and Chagasic megaesophagus. A nasogastric feeding tube was fitted and chemotherapy (cisplatin/5-fluorouracil) was started. After 3 months, the patient presented with progressive disease and eventually died due to recurrent pneumonia.
Chagas disease is a tropical disease caused by the protozoan Trypanosoma cruzi. It is transmitted to humans by Triatominae insects, found in rural areas of Latin America, Asia and Africa.1 Migratory flows have spread the disease worldwide. The United States and Spain are the non-endemic countries with more cases.2 Approximately 30% of infected individuals develop chronic stage disease. Gastrointestinal motor disorders, such as achalasia/megaesophagus, are a result of enteric nervous system injury caused by the protozoan.3 Among patients with Chagasic megaesophagus, an increased incidence of SCC is expected.
Conflict of interestsDa Fonseca, LG: lecture fees from Bayer and Roche.
Hashizume, PH: nothing to declare.
