




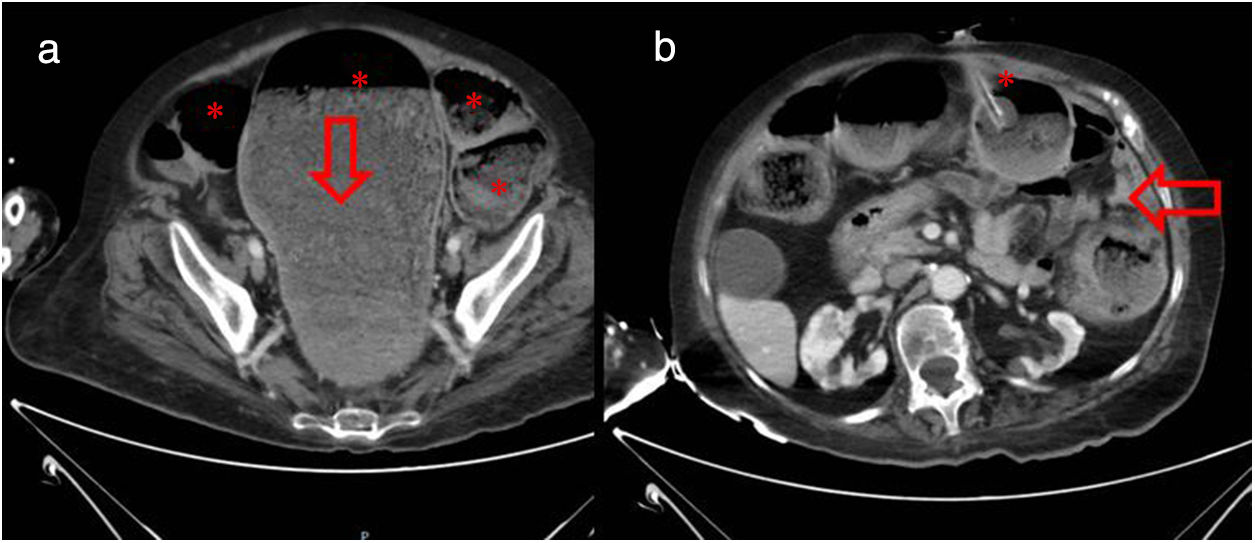
We present the case of a 74-year-old woman with dementia and a percutaneous endoscopic gastrostomy (PEG), which had been created nine months earlier. She went to Accident and Emergency 48h after replacement of the PEG tube, with balloon-tube placement, because of the emission of faeces through the tube. Abdominal CT was performed in view of suspected intestinal obstruction, showing the colon to be distended with abundant stools and a faecaloma in the sigmoid colon/rectum (Fig. 1A). As an incidental finding, the PEG tube balloon was seen in the colon and a fistulous tract between the gastric wall and the colon (Fig. 1B).
 Distension of the colon with abundant stools (asterisks) and faecaloma in sigmoid colon/rectum (arrow). (b) PEG balloon tube located in lumen of colonic (asterisk) and fistulous tract 17mm long between gastric wall and colon (arrow).")
In the light of these findings, it was deduced that the PEG had been mistakenly inserted between the abdominal wall and the stomach nine months previously, causing asymptomatic transluminal perforation of the colon. When the tube was replaced, it ended up in the lumen of the colon without passing through the gastric-colonic fistula.
To resolve the situation, enemas were initially administered with a rectal probe and evacuating solution through the PEG tube. Subsequently, the patient was admitted to general surgery with conservative treatment being decided on. The PEG tube was removed with spontaneous closure of the cutaneous-colonic fistula without incident. In the end, it was decided to insert a balloon tube under radiological control.
Please cite this article as: Diéguez Castillo C, Roa Colomo A, Díaz Alcázar MM, Martínez Tirado P, Palacios Pérez Á. Detección tardía de complicación precoz tras colocación de gastrostomía endoscópica percutánea: perforación transluminal de colon asintomática. Gastroenterol Hepatol. 2019;42:39–40.
