




We report the case of a 48-year-old man with a history of myelodysplastic syndrome, treated two months earlier with allogeneic haematopoietic stem-cell transplantation (allo-HSCT), who was admitted with diarrhoea for the past week and a low-grade fever in the 12 h prior to admission. Laboratory testing revealed leukocytosis (17.87 × 103/μl), elevated C-reactive protein (CRP) (233.6 mg/l), elevated procalcitonin (5.76 ng/ml) and asymptomatic hyponatraemia (113 mEq/l), with no significant liver abnormalities.
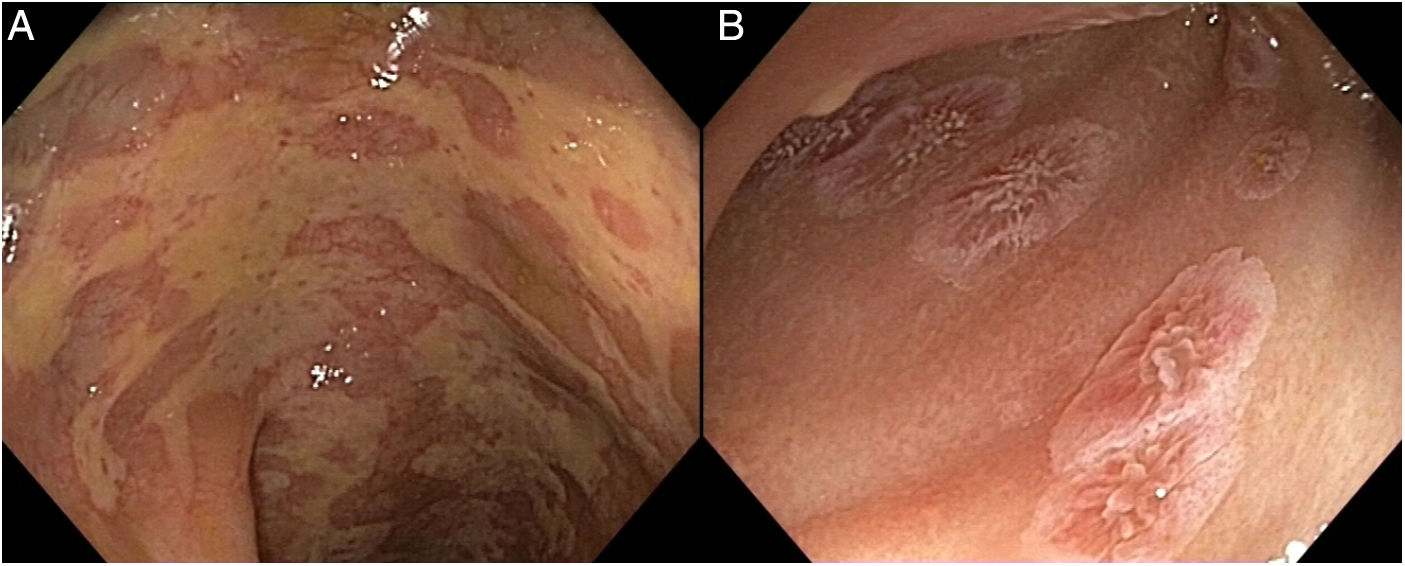
In view of the possibility of an opportunistic infection, given the patient's degree of immunosuppression, empirical antibiotic therapy was started and microbiological tests were performed, including stool culture and a stool Clostridium difficile toxin test, as well as viral load tests for cytomegalovirus (CMV), adenovirus and Epstein–Barr virus, all of which were negative. Ultimately, as acute graft-versus-host disease (GvHD) was suspected, a colonoscopy was performed, revealing diffuse involvement of the entire colon, with superficial ulcers and denuded ileal mucosa (Fig. 1) suggestive of GvHD. Biopsies were taken (Fig. 2) which confirmed the diagnosis.
 Colonic mucosa showing large, irregular, superficial ulcers. B) Denuded ileal mucosa with near-complete loss of intestinal villi, except for some circumferential areas of partially preserved mucosa.")
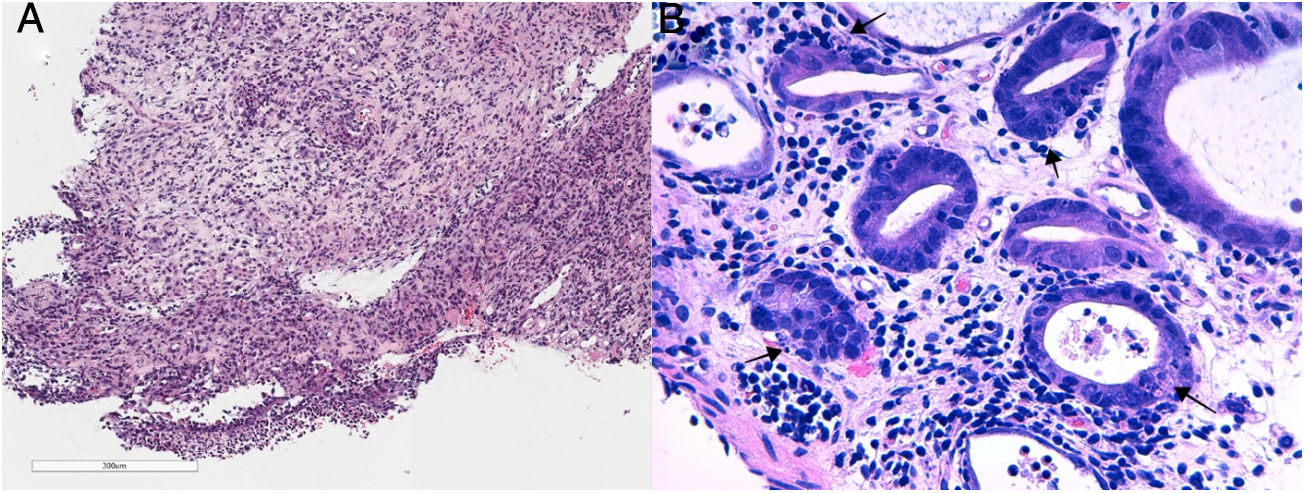
, showing much evidence of cell apoptosis at the bottom of the crypts (arrows) (B, 20× magnification).")
Haematoxylin–eosin staining: Intestinal mucosa with extensive erosion and ulceration of the surface epithelium accompanied by mixed inflammatory infiltration extending through the lamina propria (A, 4× magnification), showing much evidence of cell apoptosis at the bottom of the crypts (arrows) (B, 20× magnification).
Acute GvHD is a common complication of allo-HSCT in which activated donor T lymphocytes attack healthy recipient tissue. It has a cumulative incidence following allo-HSCT of 40%–80%1 and may affect the skin, the liver or any segment of the gastrointestinal tract. In cases of gastrointestinal involvement, it usually manifests with symptoms such as abdominal pain, vomiting and secretory diarrhoea.2 Measurement of lost volume is very important as it determines the seriousness of the condition, along with skin and liver involvement.
Diagnosis is based on ruling out possible infectious causes, combined with endoscopic studies (with colonoscopy being preferred over gastroscopy)3 including biopsy. It is important to note that GvHD may be present even in a macroscopically normal colon; therefore, in that case, complementary ileoscopy should be performed in search of ileal lesions, in addition to biopsy of apparently healthy tissue.4
Conflicts of interestThere are no conflicts of interest to declare.
Please cite this article as: Soutullo-Castiñeiras C, Plumé G, Zac C, Bustamante-Balén M. Afectación intestinal grave por enfermedad injerto contra huésped aguda. Gastroenterol Hepatol. 2022;45:297–298.
