




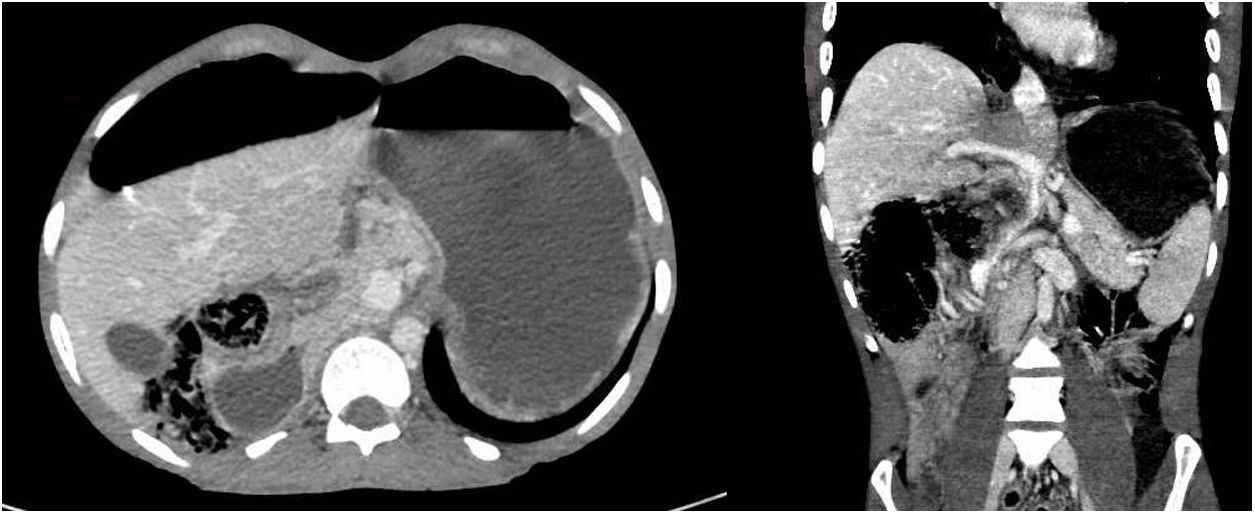
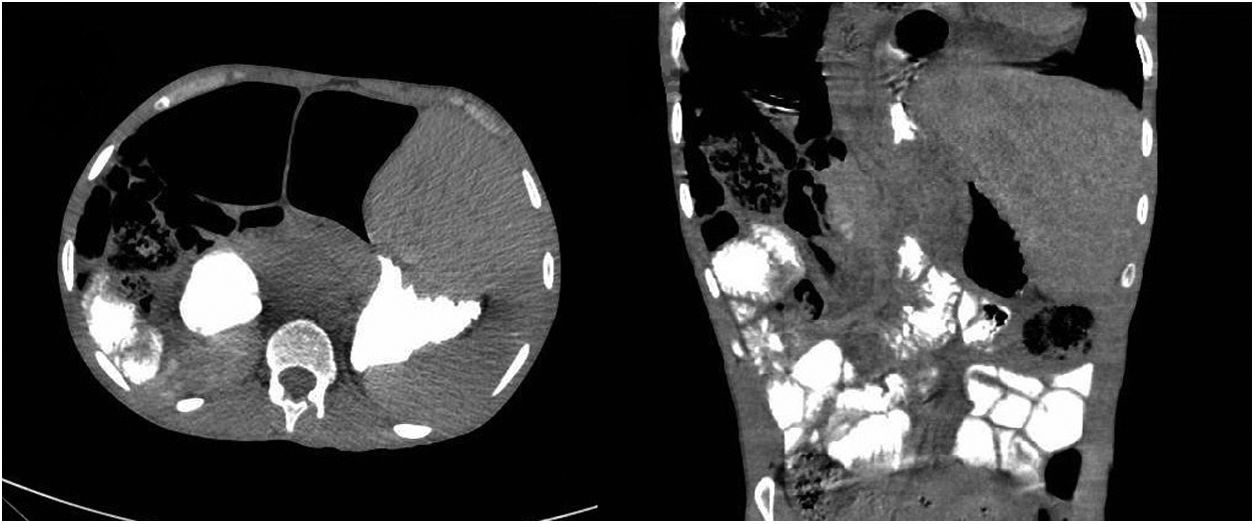
A 31-year-old man with severe intellectual disability came in with signs and symptoms of vomiting, constipation, abdominal distension and low-grade fever for the past two days. As bowel obstruction was suspected, abdominal computed tomography (CT) was ordered and showed gastric dilatation and a probable internal hernia (Fig. 1). Repeat CT with oral contrast to confirm and identify the site of obstruction showed the passage of contrast past the supposed obstruction to the small bowel loops, stomach decompression and the location of the liver in the left hypochondrium (Fig. 2).
 and coronal (right) CT imaging showing the liver in the right hypochondrium and gastric dilatation.")
 and coronal (right) CT imaging showing the location of the liver in the left hypochondrium and the passage of oral contrast to the small bowel loops, past the obstruction.")
After receiving nothing by mouth for 24 h and having a nasogastric tube placed, the patient showed recovery of normal intestinal transit and resolution of his abdomen distension. Oral nutrition was started and tolerated well. Given that hepatopexy, the only surgical option available, has a high relapse rate, taking into account the patient's stability and the self-limiting nature of his signs and symptoms, expectant management was pursued. The patient was discharged from hospital; he remained asymptomatic four months later.
Wandering liver or hepatoptosis is a congenital disease caused by abnormalities in liver fixation that could lead to free movement of the liver.1,2 Symptoms range from nonspecific symptoms to symptoms related to rotation of liver structures, complicating diagnosis. It is very uncommon, with fewer than 30 cases reported since 1890,3 and therefore it is difficult to arrive at a consensus on its management. In a patient with bowel obstruction caused by an excessively mobile liver, hepatopexy is an option,1,3 although it is associated with high rates of recurrence. Expectant management may be a valid option in an asymptomatic patient with resolved obstruction in whom close follow-up is possible2; our decision to pursue this approach was based on these considerations.
FundingNo funding was received for this study.
Please cite this article as: Forneiro Pérez R, Ramos Sanfiel J, Dabán López P, García Rubio J. Hígado errante como causa de obstrucción intestinal. Gastroenterol Hepatol. 2022;45:295–296.
